Abstract
Background:
Suture bridge fixation (SBF) has demonstrated excellent rates of osseous integration for osteochondral fractures and has been adapted for knee OCD lesions.1 The study purpose was to evaluate radiographic healing and patient reported outcomes (PROs) of trochlear OCD treated with SBF.
Hypothesis:
Suture bridge fixation will provide high levels of osseous integration and improvement in PROs.
Methods:
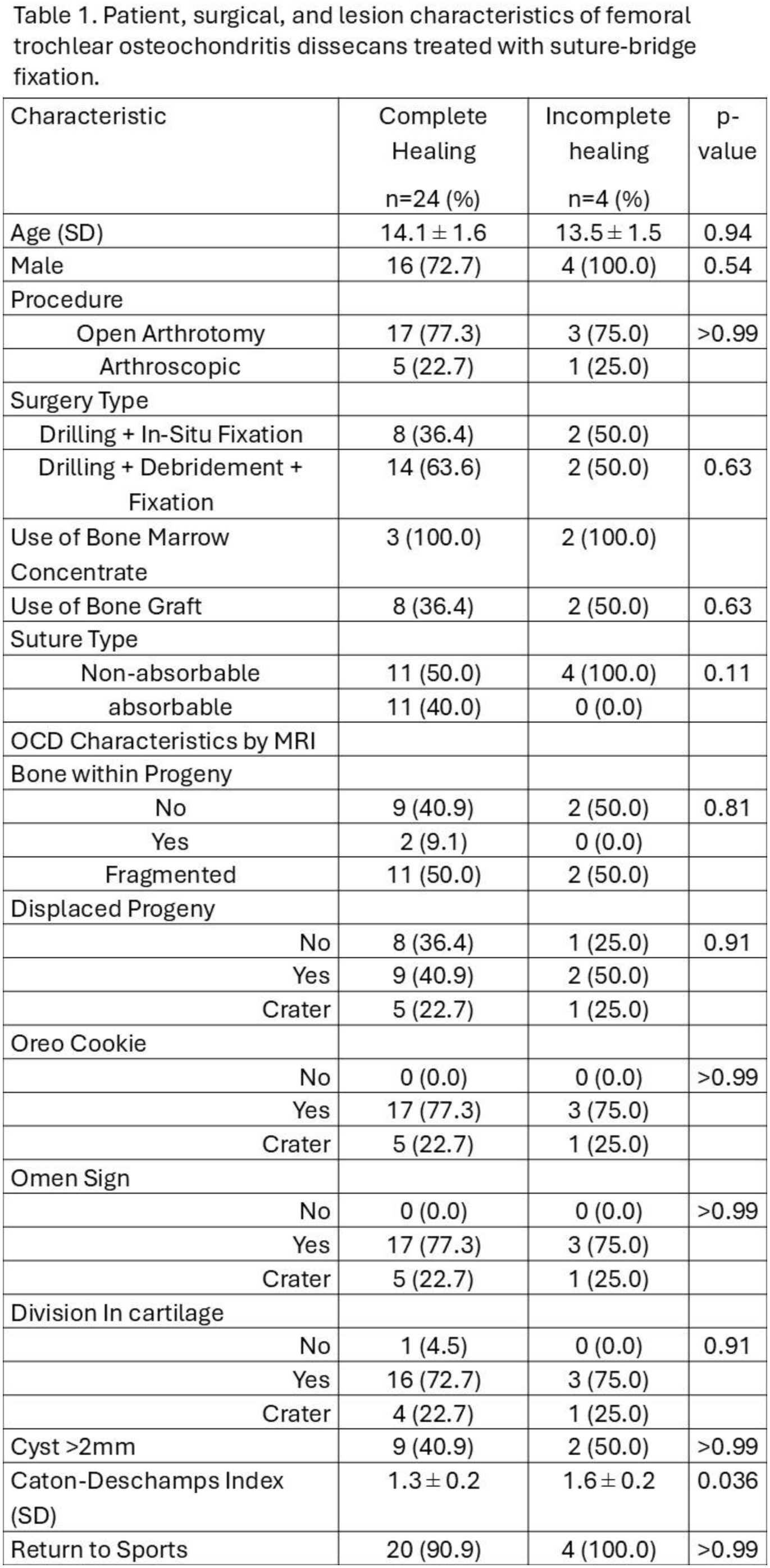
All femoral trochlear OCDs managed with SBF over 5 years (10/2019 – 10/2024) were analyzed. All SBF utilized bioabsorbable knotless anchors or sliding suture anchors in combination around the margins of the lesion with multiple strands of hand-tensioned bridging suture. Demographics, peri-operative imaging data, complications, and reoperations (excluding suture removal), return to sport, and baseline and 6 months PROs [Knee injury and Osteoarthritis Outcome Score (KOOS)] were collected. Healing was assessed by radiography and/or magnetic resonance imaging (MRI) as follows: 1) Complete osseous integration 2) ≥50% integration 3) <50% integration.
Results:
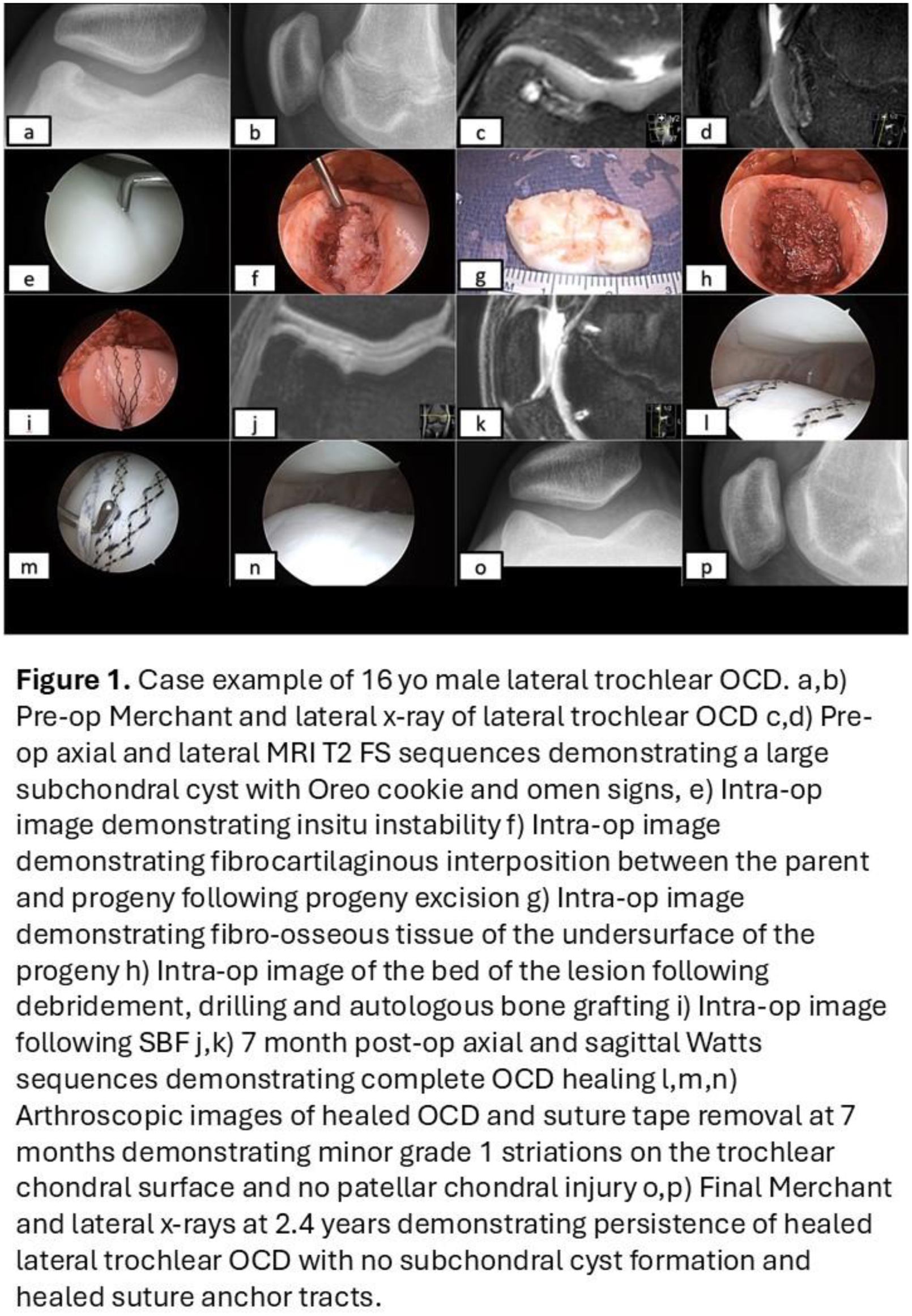
26 trochlear OCDs (24 knees, 22 patients) with mean follow-up of 19.2 months (range, 5-57) were included. Patients were 14.1 ± 1.5 years, 81.2% male, with BMI of 21.1 ± 3.1. All lesions were unstable; 6 were displaced, and the remaining 20 had an Oreo cookie sign and division of the cartilage or an omen sign on MRI. Mean trochlear OCD size were179.4 mm2 (range, 36.8-482.2 mm2) and mean major length was 21.1 mm (range, 11.0-34.2 mm) and mean major depth was 9.4 mm (range, 9.4-14.1). 10 (38.5%) underwent arthroscopic in-situ fixation with drilling, and 16 (61.5%) underwent subchondral debridement +/- bone graft and SBF. (Table 1) At first postoperative MRI (3.81 ± 1.0 months), 57.7% (15) of lesions achieved complete union, 30.8% (8) had ≥50% healing, and 11.5% (3) <50% integration. At final follow-up (10.8 ± 13.2 months) 22 (84.6%) had complete union and only 1(9.1%) lesion remained <50% healed. (Figure 1) Caton-Deschamps Index was greater in those who had suboptimal healing (1.6 vs 1.3, p=0.036). 20 (90.1%) returned to sports at 7.8 ± 2.9 months postoperatively. Improvements were achieved postoperatively in the KOOS daily living (88.94 vs 78.2; p =0.025), KOOS Pain (90.1 vs 70.9; p= <0.001), KOOS PS (vs 20.6; p =0.025), KOOS JR (84.7 vs 66.6; p= <0.001). No patients required osteochondral allograft or reoperation for trochlear OCD.
Conclusion:
Suture Bridge Fixation of unstable femoral trochlear OCDs resulted in 84.6% complete osseous integration. There were no reoperations for OCD treatment and 90.1% of patients returned to sports.