Abstract
Background:
Femoral version’s role in the adolescent pre-arthritic hip pain remains increasingly recognized, including in femoroacetabular impingement (FAI). Increased or decreased femoral version may play a role in hip biomechanics contributing to instability or impingement, respectively.
Hypothesis:
The purpose of this study was to compare the outcomes of hip arthroscopy for FAI across femoral version groups in a multicenter prospective cohort study of adolescent hips.
Methods:
A prospective multicenter cohort of adolescent FAI patients undergoing primary hip arthroscopy was collected, including assessments of femoral version. Inclusion criteria were FAI patients aged 14-18.9 years at the time of index surgery. Exclusion criteria were aged ≥19 years, previous ipsilateral hip procedures, associated disorders, or Tönnis grade 2 or greater osteoarthritis. Femoral version was measured on low-dose CT using the Yoshioka oblique method and categorized into five subgroups: <5º, 6º-15º, 16º -25º, 26º -35º, and 35º+. Patient-reported outcomes (PROs) were collected at ≥1-year follow-up. The modified Harris Hip Score (mHHS) was assessed against the minimal clinically important difference (MCID) of 8 and the patient acceptable symptom state (PASS) of 74. Additional PROs included HOOS Pain and Sports/Recreation and iHOT-12 scores. Composite failure was defined as reoperation for persistent symptoms or failure to achieve either the mHHS MCID or PASS. One-way ANOVA and chi-square tests compared groups for continuous and categorical measures, respectively..
Results:
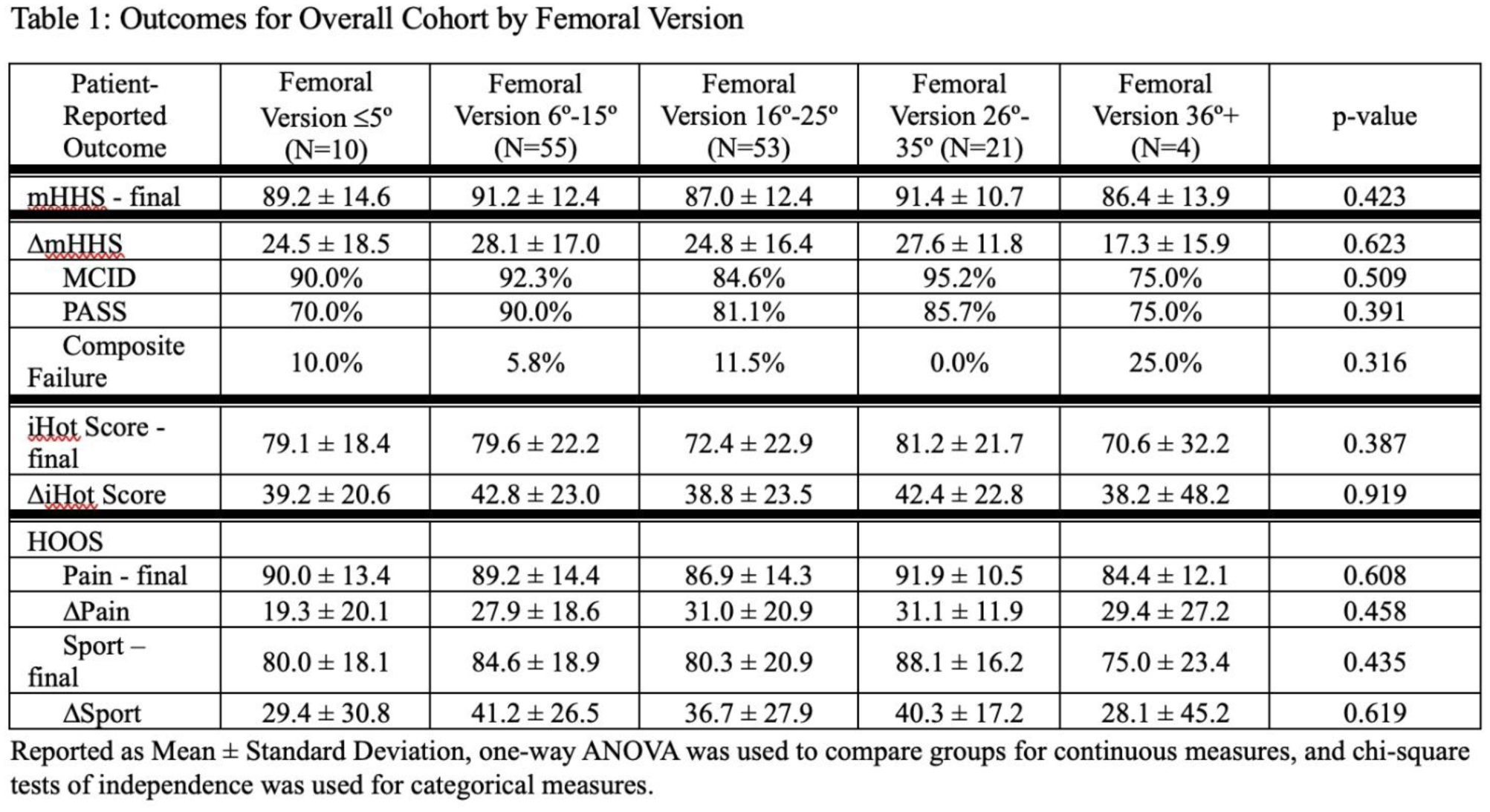
One hundred forty-three adolescent FAI patients were tracked for an average of 1.1 ± 0.2 years after surgery, with 37.1% were male and 62.9% female. Femoral version varied: 2.8% had >35°, 14.7% were between 25º-35°, 37.1% were between 15º-25°, 38.5% were between 6º-15°, and 7.0% were ≤5°. Males had significantly lower femoral version than females (15.5º vs 18.8º; p=0.016). Outcomes in the mildly (16º-25º) and moderately (26º-35º) increased femoral version groups were like those in the normal femoral version group (6º-15º) by mHHS, iHOT-12, and HOOS (all p >0.05). Severely increased femoral anteversion (>35º) was seen in 2.8% of patients (n=4) and had a higher composite failure rate (25.0%) compared to moderately increased femoral anteversion (0%). The decreased femoral version group (≤5º, n=10) had a 10.0% composite failure rate compared to the normal version group (6º-15º) with a 5.8% failure rate.
Conclusion:
Over half of adolescents undergoing FAI surgery have some level of increased femoral version. In the absence of associated acetabular dysplasia, mild to moderately increased femoral version does not appear to negatively affect the short-term outcomes in adolescents.