Abstract
Background:
Patellofemoral instability (PFI) and anterior cruciate ligament (ACL) rupture are two of the most common knee injuries in adolescents requiring surgical intervention. Within PFI, the trajectory of postoperative quadriceps and hamstring strength recovery guiding rehabilitation milestones is largely extrapolated from ACL-reconstruction (ACLR) literature. Whether ACLR-derived standards are appropriate for patients undergoing isolated medial patellofemoral ligament reconstruction (MPFLR) remains unknown. To address this gap, we compared isokinetic strength recovery in a propensity-score–matched cohort of MPFLR and ACLR patients.
Hypothesis:
MPFLR patients will demonstrate slower quadriceps strength recovery than matched ACLR patients over the postoperative period.
Methods:
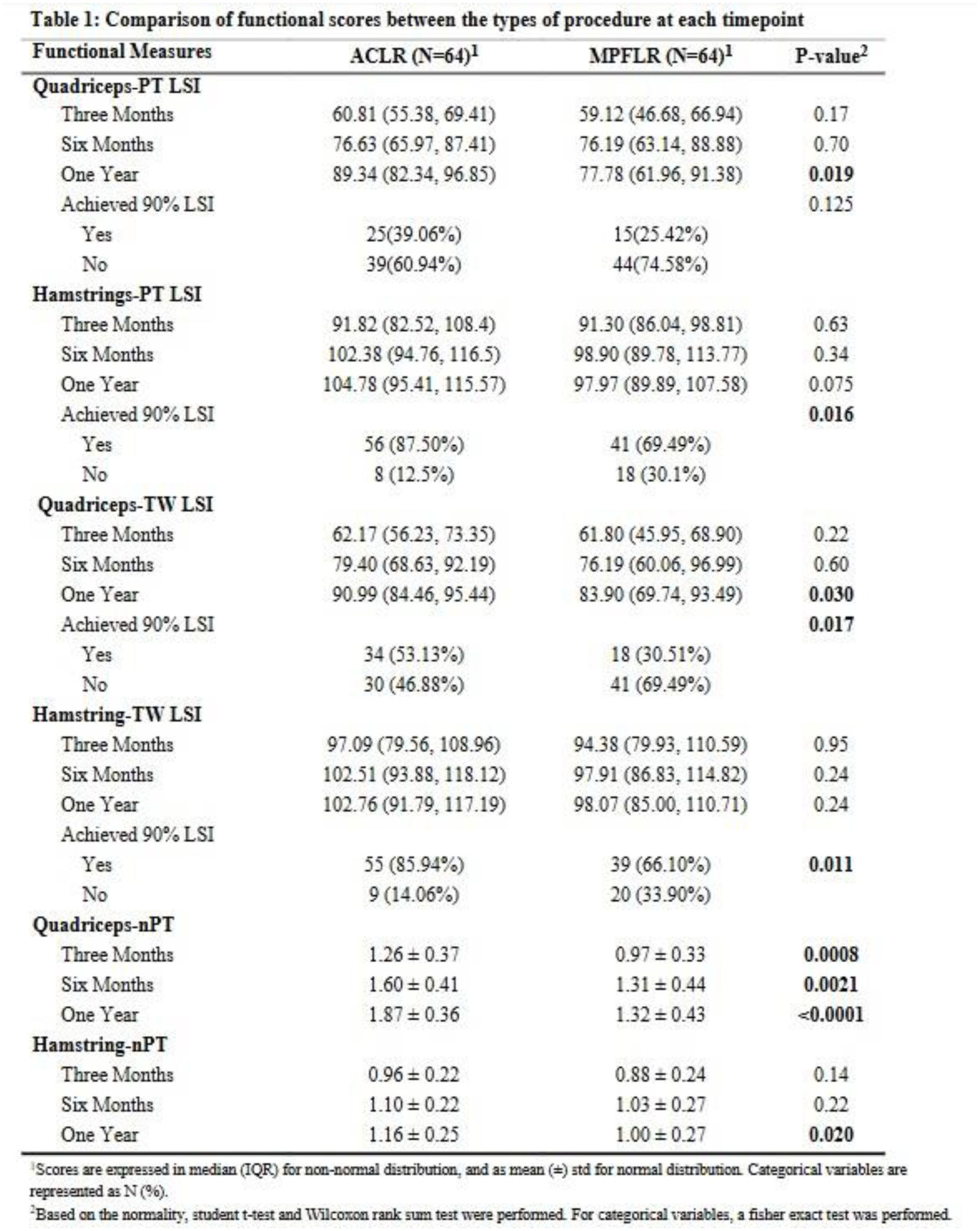
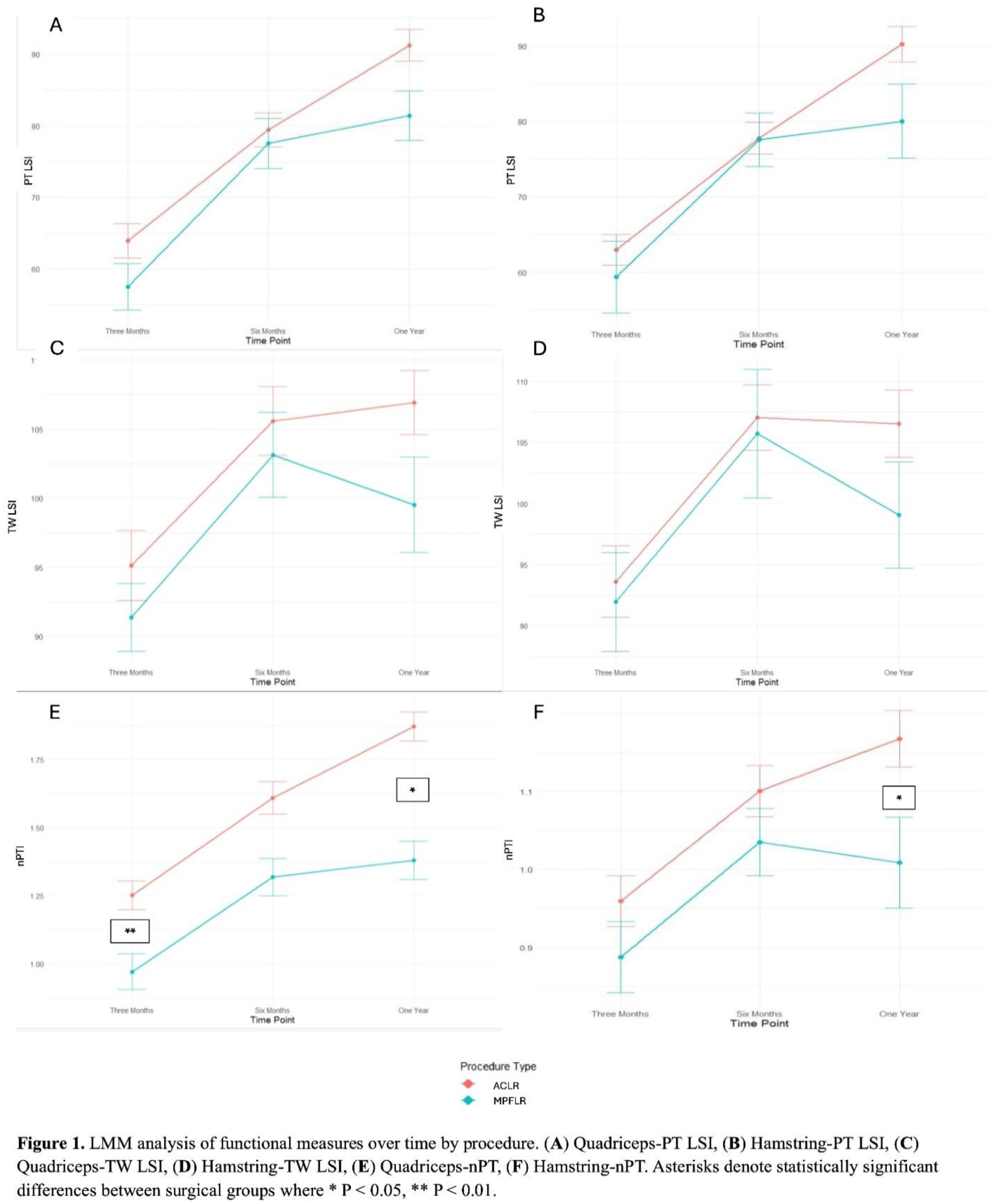
We conducted a retrospective matched cohort study of patients aged 10-18 years who underwent either isolated MPFLR or primary arthroscopic ACLR at a tertiary children’s hospital from 2011–2023. Patients were excluded if they had multiligamentous injuries, concomitant tibial tubercle osteotomy, or additional ipsilateral knee procedures. One-to-one propensity score matching was performed using nearest-neighbor methodology, treating age as a continuous variable and exact-matching on sex and BMI category. Isokinetic strength was assessed using the Biodex dynamometer at 180°/s at 3, 6, and 12 months postoperatively. Measures included quadriceps and hamstring peak torque (PT) and total work (TW) limb symmetry index (LSI), and peak torque normalized to body weight (nPT). Between-group differences were assessed using t-tests or Wilcoxon rank-sum tests. A linear mixed effects model (LMM) evaluated interaction effects of time and procedure type.
Results:
A total of 128 patients (64 MPFLR, 64 ACLR) with balanced baseline characteristics were included. By 1 year postoperatively, ACLR patients achieved significantly higher quadriceps PT LSI (89.3 vs. 77.8, P = 0.019), nPT (1.87 vs. 1.32, P < 0.0001), and TW LSI (90.99 vs. 83.90, P = 0.030) compared to MPFLR patients (Table 1). Hamstring PT and TW did not significantly differ between groups at any timepoint. LMM confirmed a significant procedure-by-timepoint interaction in quadriceps strength at 1 year favoring ACLR (P = 0.012), while hamstring strength trajectories were comparable (Figure 1). About 20% more ACLR patients achieved >90% LSI across all metrics by 1 year compared to MPFLR patients.
Conclusion:
Pediatric patients undergoing MPFLR demonstrate slower quadriceps strength recovery than matched ACLR peers despite similar hamstring recovery. Utilizing ACLR-based strength criteria at these designated timepoints may be unrealistic for many patients post-MPFLR. Future research should focus on developing MPFLR specific milestones based upon population-specific outcomes and their relationship to functional performance.