Abstract
Background:
Trochlear dysplasia is common in patients with patellofemoral instability (PFI) and a strong risk factor for recurrence. While trochleoplasty addresses severe dysplasia, concerns about complications have limited its adoption in young patients. A learning curve likely exists when adopting new, complex surgical techniques during which procedural efficiency and surgical indications evolve and procedural morbidity may be higher. This study evaluates the initial adoption of trochleoplasty by a single surgeon in adolescents to characterize patient selection, operative efficiency, and early complications.
Hypothesis:
During initial adoption, trochleoplasty reliably addresses instability in patients with severe dysplasia and/or prior failed surgical stabilization with an acceptable early complication profile.
Methods:
A retrospective review was performed of adolescent patients (<20 yo) who underwent thin-flap (Bereiter-type) trochleoplasty by a single surgeon from 2020–2025. Outcomes were assessed in patients with ≥3 months of follow-up. Demographics, clinical presentation, and radiographic measures (trochlear morphology, patellar height, and axial alignment) were examined. Surgical treatment and early outcomes were recorded. Descriptive statistics were performed of cohort characteristics and correlation analysis of surgical time versus case number for primary trochleoplasty procedures.
Results:
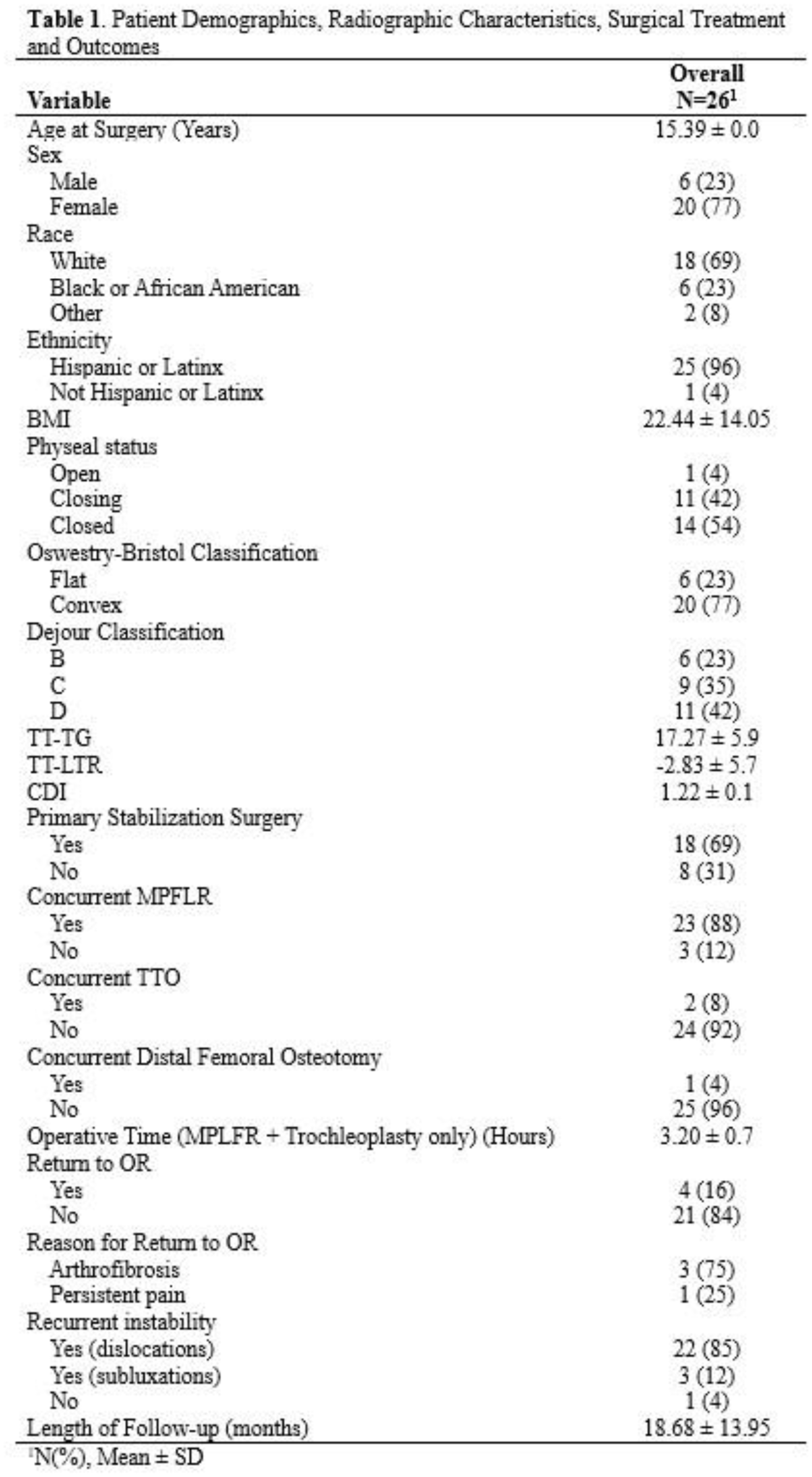
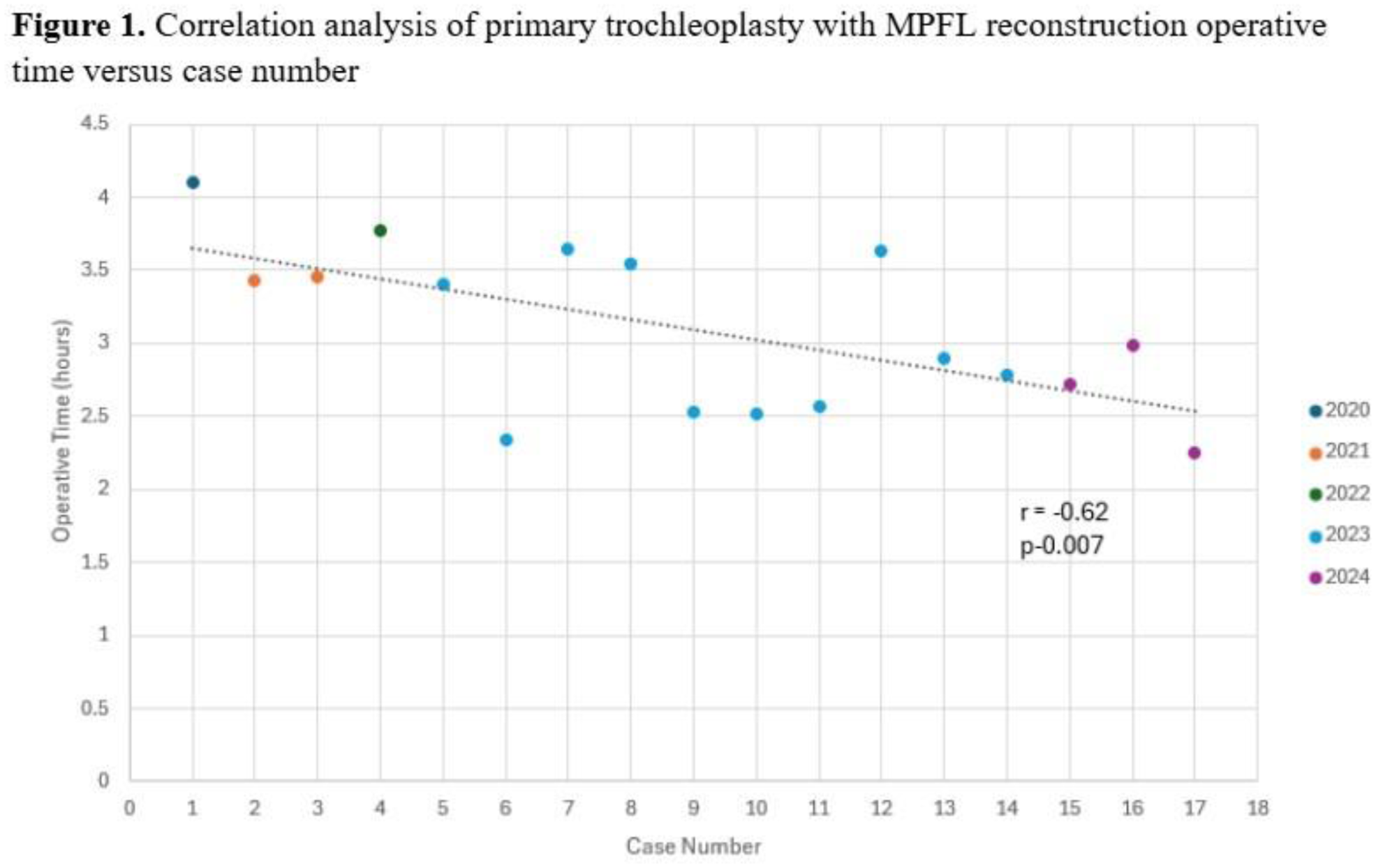
Trochleoplasty was performed in 26 adolescent patients (16.09 ± 1.6 years, 77% female) between 2020-2025. All patients had moderate or severe trochlear dysplasia. The cohort had modestly elevated patellar height and axial alignment measures. Eight (31%) patients failed prior stabilization (MPFL [n=6] and MPFL+TTO [n=2]). MPFL reconstruction was the most common concomitant procedure performed with trochleoplasty. At mean 18.68 ± 14.0 months follow-up (one patient lost to follow-up after surgery), no dislocations had occurred but two patients (8%) endorsed subjective instability (subluxation) events that resolved with nonoperative modalities. Four patients (15%) required a return to the operating room, most commonly for arthrofibrosis (n=3), but no infection, flap nonunion or implant failure were observed (Table 1). All complications occurred in the first 20 patients. Mean operative time for primary trochleoplasty (n=17) was 3.37 ± 0.8 hours with a downward trend observed over the study period (r=-0.62, p=0.007, Figure 1).
Conclusion:
Even during early adoption, trochleoplasty provided consistent stability in these complex patients with severe dysplasia and/or prior surgical failure, with an acceptable complication profile. Trends in operative time and complication patterns were indicative of a learning curve. Further research is needed to refine indications and compare long-term outcomes to other patellar stabilizing surgeries in patients with severe trochlear dysplasia.