Abstract
Background:
Inability to return to sport after anterior cruciate ligament reconstruction (ACLR) is well documented and reduction in overall physical activity is common. The ACL Reasons survey is a validated tool to assess patient perceptions of barriers to physical activity after ACLR. While this tool has been used qualitatively, an updated version of the survey allows patient to quantify the importance of perceived barriers of physical activity.
Hypothesis:
The purpose of this study was to describe the frequency of patient-reported barriers to physical activity and rate the importance of selected barriers at multiple sites with the use of visual analog scales. Our hypothesis was that fear of injury, fear of symptoms and knee symptoms would be the most commonly reported reasons across our sample.
Methods:
A retrospective analysis was completed of participants between 13-30 years who underwent primary ACLR between 2018-2024 at two different institutions. Descriptive statistics were calculated for groups based on answers to question 1 on the ACL Reasons survey. Independent sample t tests were use to calculate differences in visual analog scores (VAS) scores, and chi square analyses were used to calculate frequency differences in ACL reasons between groups.
Results:
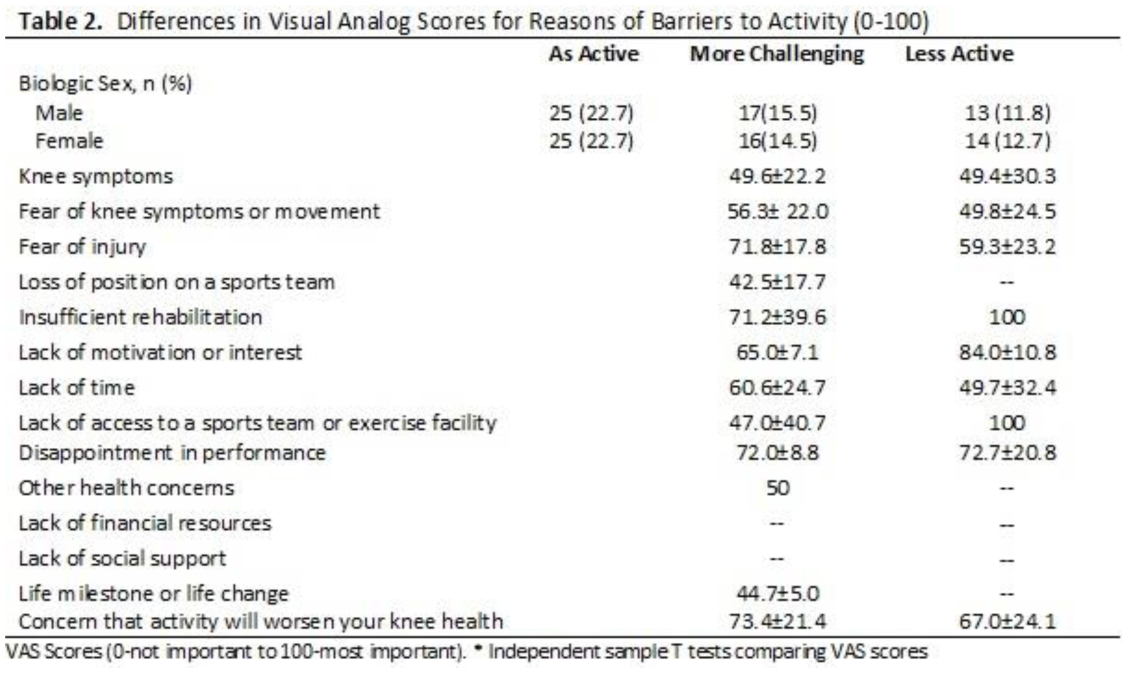
A total of 110 participants (sex: 50% female, age= 17.5±3.4 years) completed the ACL Reasons survey at 9.3±1.6 months after ACLR. 43.9% of participants indicated they were as active before surgery, and 24.6% of participants reported being as active as before surgery but it was more mentally or physically challenging. 31.6% of participants reported being less active than before surgery. Knee symptoms, fear of knee symptoms or movement, and fear of injury were the most common barriers to activity (Figure 1). Concerns activity would worsen knee health was selected more often in the less active group (p=0.01; 0.09 (0.01-0.8). There were no other significant differences between the two groups frequencies or VAS scores in the less active and more challenging groups. VAS scores (0-not important to 100-most important) ranged from 44.7-72.0 in the less active group, while in the same activity level but more challenging group scores ranged from 49.7-72.7 (Table 1).
Conclusion:
The ACL Reasons survey performed similarly across sites, and 56.2% of participants reported being less active or experiencing mental or physical challenges when engaging in activity after ACLR. VAS scores were lowest when participants selected knee symptoms, fear of knee symptoms and fear of injury, though there were no significant differences between groups.