Abstract
Background:
Adolescent athletes after anterior shoulder instability surgery should be physically and psychological prepared before returning to sport (RTS). The Shoulder Instability Return to Sport after Injury scale (SI-RSI) measures confidence in shoulder performance, fear of reinjury, and emotional responses to returning to sport. The SI-RSI is associated with improved shoulder function (1) and successful RTS (2,3), but not yet validated for adolescents. The purpose of this study was to assess the validity of the SI-RSI in a post-labral repair adolescent population at time of RTS testing.
Hypothesis:
We hypothesized that the SI-RSI would demonstrate convergent validity with patient reported outcomes of subjective function.
Methods:
A review of patient’s charts who were between 12-18 years old and had completed a RTS testing battery after arthroscopic shoulder stabilization was performed. Convergent validity testing was performed against the QuickDASH, Pediatric Arm and Shoulder Scale (PASS), American Shoulder and Elbow Surgeons Scale (ASES), and peak torque asymmetry of shoulder internal and external rotation strength using Spearman correlations. Discriminant validity testing was performed against age, body mass index (BMI), sex, and ethnicity using Spearman correlations and Mann-Whitney U test. The presence of floor and ceiling effects were explored by assessing the frequency of minimum and maximum scores. Significance was set to p<0.05.
Results:
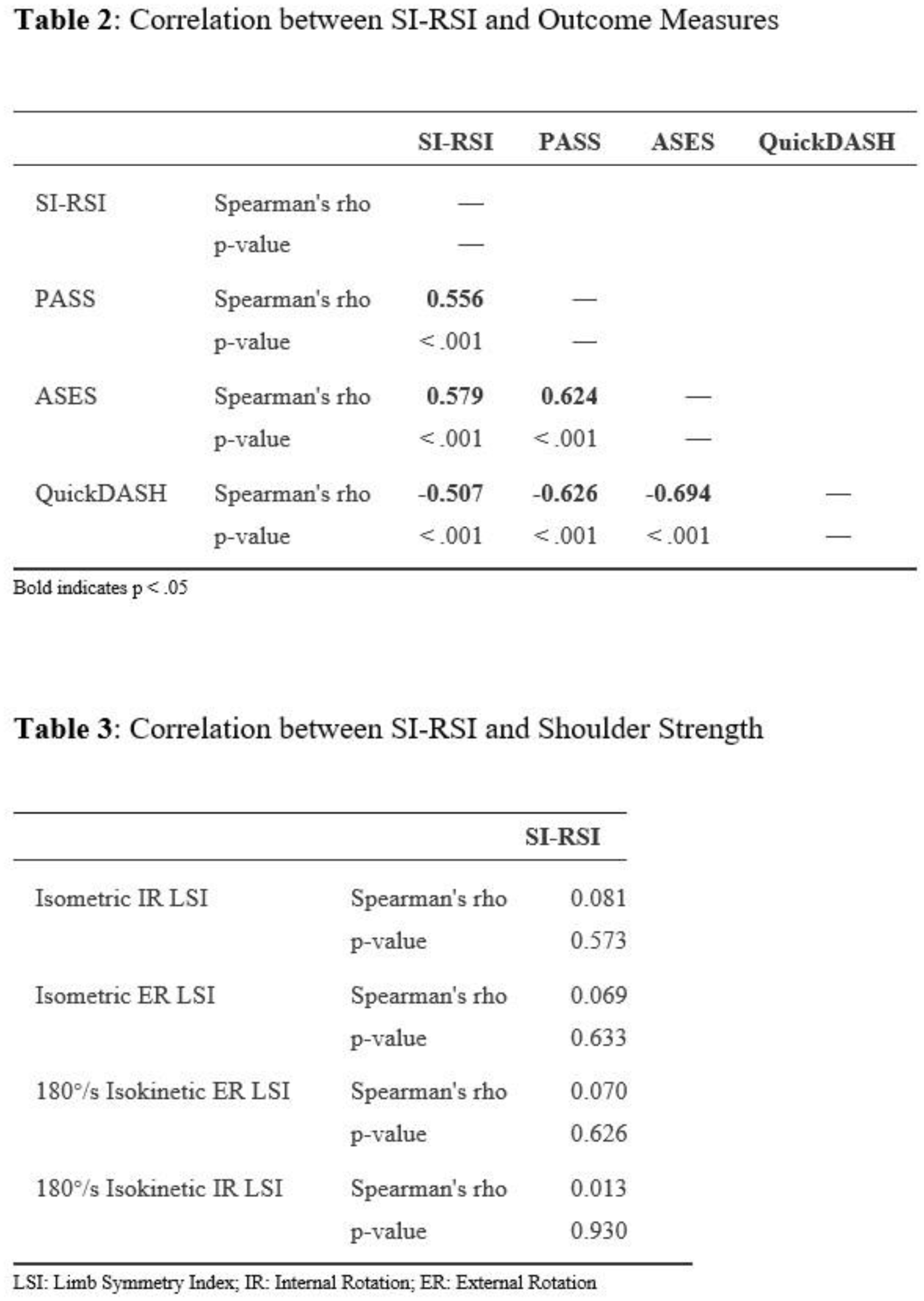
A total of 51 patients (20 females, 16.5 ± 1.3 years old, 5.74 ± 0.67 months post-operation) were analyzed. Mean SI-RSI score was 69.7 ± 21.4 and demonstrated a significant moderate correlation with QuickDASH (r=-0.507, p<0.001), PASS (r=0.556, p<0.001), and ASES (r=0.579, p<0.001). No significant correlations were noted between SI-RSI and isometric or isokinetic shoulder rotation strength (Table 3). Discriminant validity was demonstrated as age (r=-0.013, p=0.931), BMI (r=0.089, p=0.535), sex (p=0.084), and ethnicity (p=0.461) all were not significantly associated with the SI-RSI. No floor or ceiling effects were observed.
Conclusion:
The SI-RSI scale was moderately correlated with QuickDASH, PASS, and ASES scores, demonstrating convergent validity. It’s intended psychological construct was highlighted by the lack of correlation with physical strength measures. With discriminant validity against age, BMI, sex, and ethnicity, and no presence of floor or ceiling effects, these results support the utilization of the SI-RSI as a valid tool in the adolescent population. Further psychometric assessment of this scale, including item analysis for reliability, would be beneficial to improve utilization of the SI-RSI with adolescents.