Abstract
Background:
Distal radial physeal stress injury is a repetitive stress injury commonly encountered in young athletes. Diagnosis is typically made through clinical examination and radiographic features showing widened distal radial growth plate with irregular borders. Recent research has highlighted the role of musculoskeletal ultrasound (MSK-US) as a cost-effective tool for screening and diagnosis of stress related changes in other physeal injuries, such as medial elbow apophysitis. However, this topic has yet to be explored within the context of distal radial physeal injuries.
Hypothesis:
Novel MSK-US based techniques for measuring the distal radial physis will yield good to excellent reliability in healthy young athletes.
Methods:
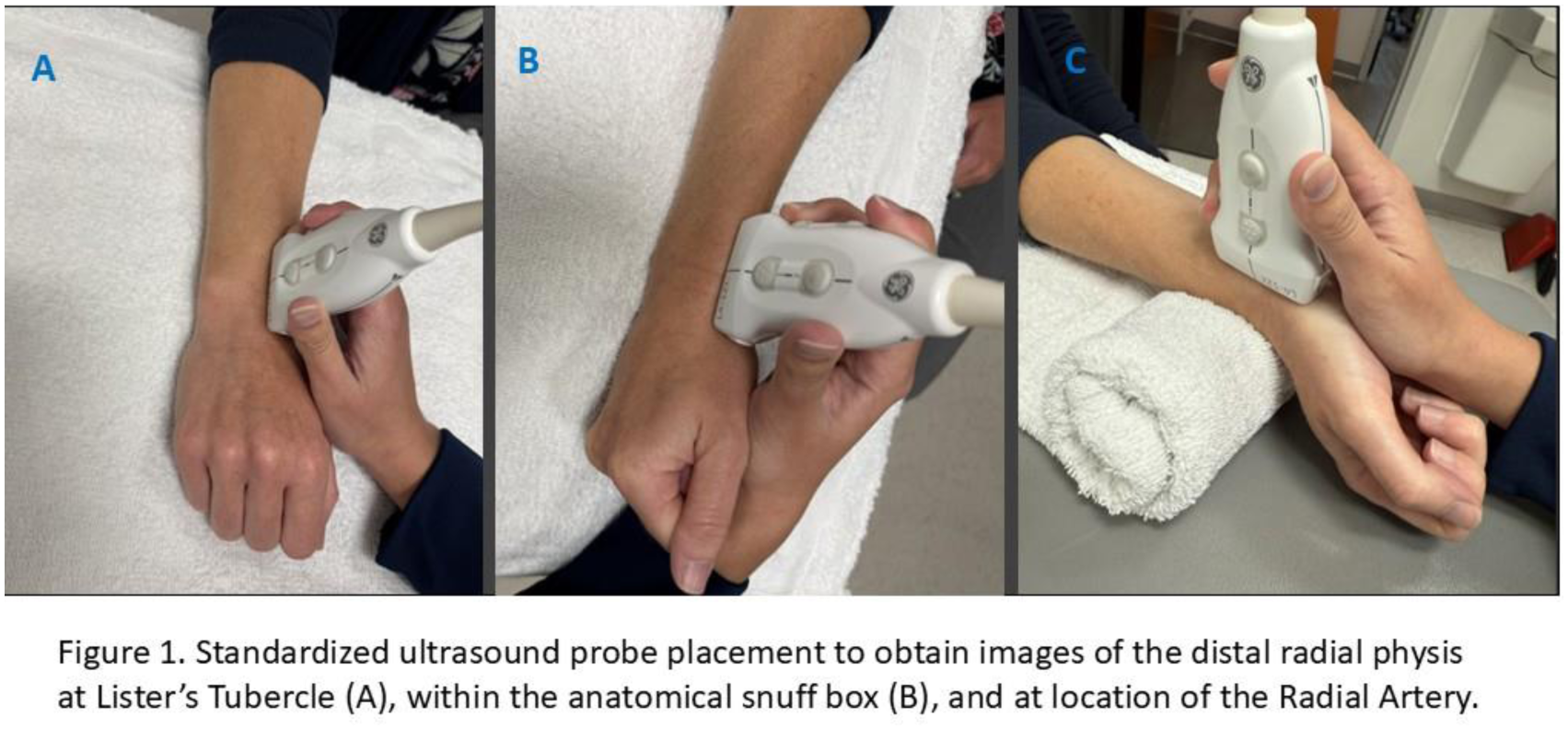
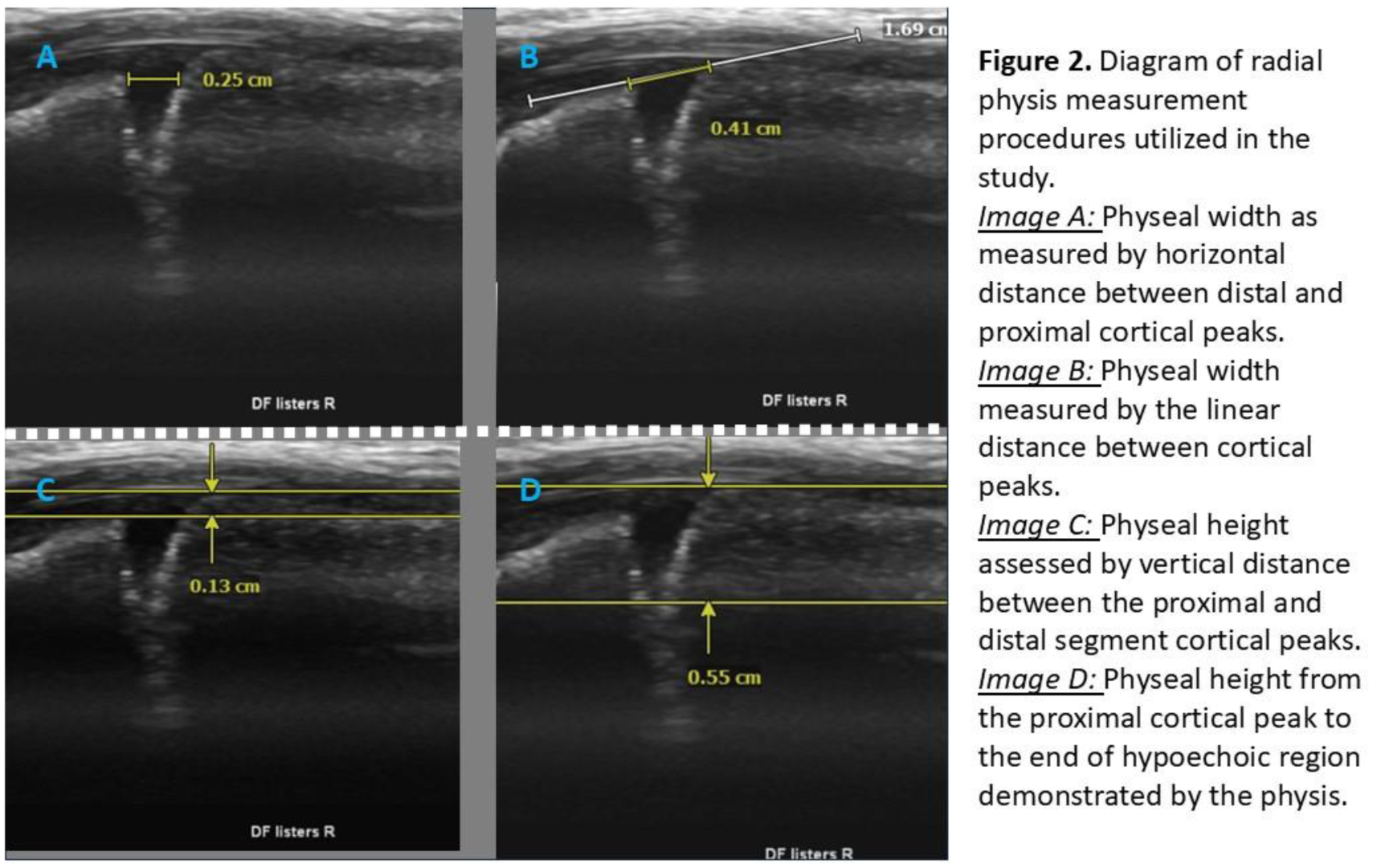
Subjects aged 8-14 years-old without any current pain, or history of radial physeal injury participated. Bilateral images of the distal radial physis were captured at Lister’s tubercle, the anatomical snuff box, and at the radial artery. (Figure 1) Physeal width and height (cm) were measured as follows: a) Width measurement #1 linear distance between proximal and distal cortical peaks, b) Width measurement #2 from cortical peaks along a line connecting the proximal and distal cortex, c) Vertical measurement #1 difference between proximal and distal cortex, d) Vertical measurement #2 height from cortex to deepest point of hypoechoic signal within growth cartilage. (Figure 2) Image collection and measurements were performed independently by two examiners. Summary statistics were calculated for the sample and Intraclass Correlation Coefficients (ICC 2,1) and 95% CI were calculated to examine interrater reliability.
Results:
Thirteen subjects (mean age 10.3 years-old, 77% female) participated with a total of 25 evaluable datapoints. Mean physeal measures ranged from 0.2-0.43cm and 0.07-0.41cm for width and height, respectively. Measurements taken at the anatomical snuff box and radial artery demonstrated the highest reliability with width measures ICC=0.762 (.531 – .888) and 0.761 (.529-.887) and vertical height of 0.571 (0.236 – 0.785) and 0.787 (.575 - .900), respectively. Other measurement procedures explored during this study demonstrated poor to moderate reliability ranging from 0.099 to 0.494.
Conclusion:
While the distal radial physis can be clearly visualized using MSK-US, only some of the measures demonstrated moderate to good reliability and may not demonstrate adequate reliability to justify clinical use at this time. The physis has highly irregular borders making the application of strict, linear measurement procedures difficult to apply consistently. Future investigation using different measurements, including cortical irregularity or hyperemia, and comparison to MRI are warranted to improve reliability and understand the limitations of physeal assessment using MSK-US.