Abstract
Background:
Recent literature has shown that the ulnar collateral ligament (UCL) and flexor pronator mass (FPM) can act either independently or jointly on the humeral medial epicondyle to produce distinct patterns of medial epicondyle fractures.
Hypothesis:
Assess the reliability and performance of a novel classification system for bony injuries of the humeral medial epicondyle.
Methods:
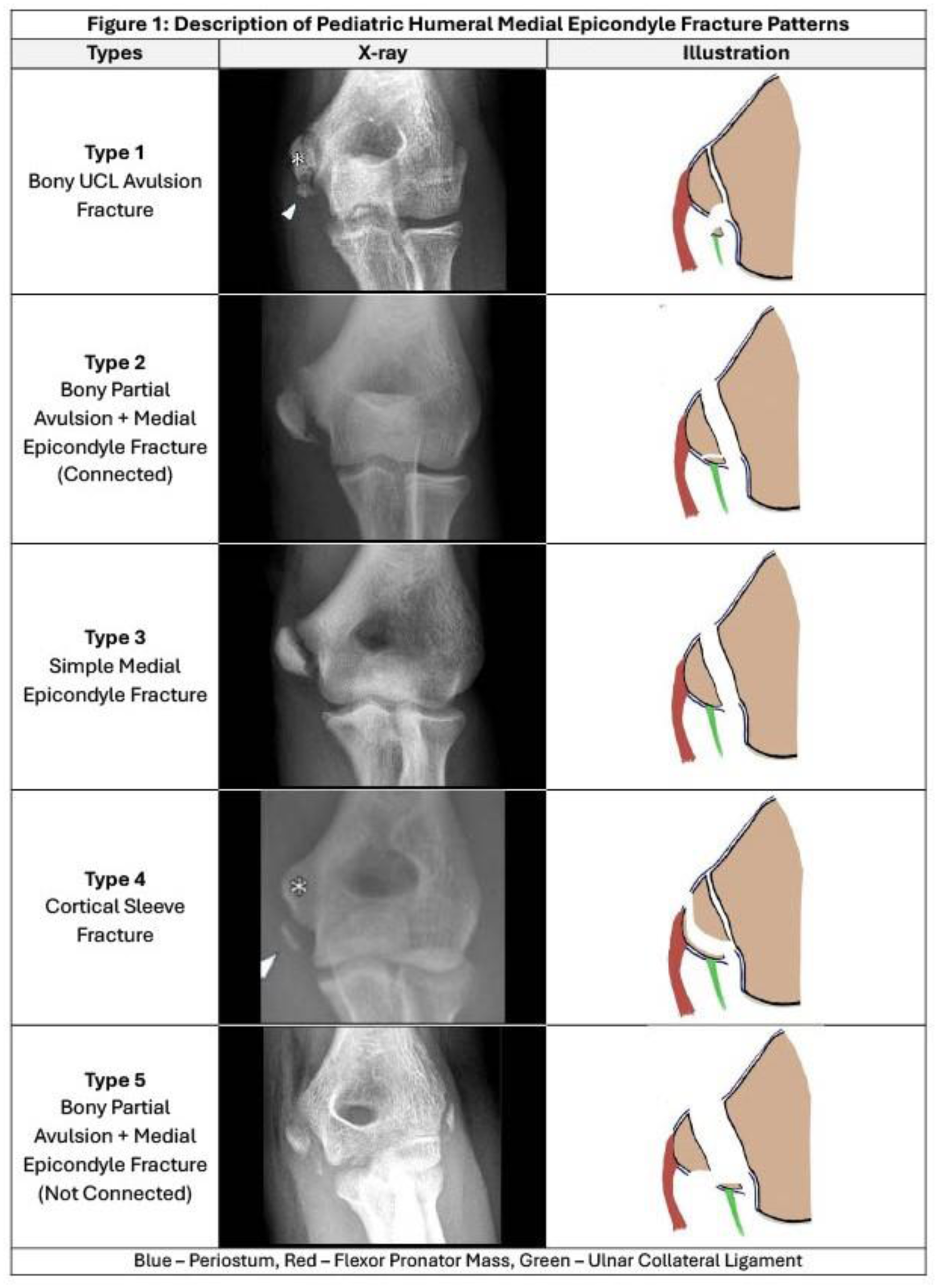
Following institutional board approval, 55 unique patients with bony injuries involving the medial epicondyle (ME) were randomly selected from a group of over 700 medial bony elbow injuries, varying in classification types (Figure 1). Eight orthopaedic surgeons and one resident assessed the fracture morphology using standard AP or lateral views, and other views when available. Fracture survey participants classified fractures as Type 1: A well-corticated fragment attached to the UCL off the inferior pole of the ME, Type 2: A combination of Type 1 and ME where the fracture fragments are still connected through soft tissue attachments as a single unit, Type 3: A ME fracture through the physis with both the UCL&FPM attached to one large fragment, Type 4: A well-defined cortical sleeve/shell-like fragment off the inferomedial aspect of the ME with the main ME physis intact and both the UCL&FPM attached, Type 5: A combination of Type 1 and ME with two separate unconnected fragments. Intra-observer reliability was then calculated for each fracture type to assess agreement using Gwets AC1.
Results:
The overall reliability estimate for the five categories showed substantial interobserver reliability, with an overall GwetsAC1 score of 0.714 (95% CI: 0.594 - 0.833). Almost perfect observer reliability was shown for Type 1 (AC1 = 0.890; 95% CI: 0.747- 1.00), Type 3 (AC1 = 0.932; 95% CI: 0.874 -0.990) and Type 4 (AC1 = 0.961; 95% CI: 0.899- 1.00). Type 5 showed substantial reliability (AC1 = 0.6491; 95% CI: -0.142 - 1.00) whereas Type 2 (AC1 = 0.585; 95% CI: 0.371-0.798) showed moderate reliability.
Conclusion:
Overall, the classification system demonstrates substantial reliability with bony UCL avulsions, classical medial epicondyle fractures, and cortical sleeve fractures, showing almost perfect reliability. Raters reported difficulty distinguishing between Type 2 and Type 3 fracture patterns, raising the possibility that a revised classification system combining these two categories may provide overall better reliability. Future studies will be required to investigate this possibility, as well as the potential for sub-classification.