Abstract
Background:
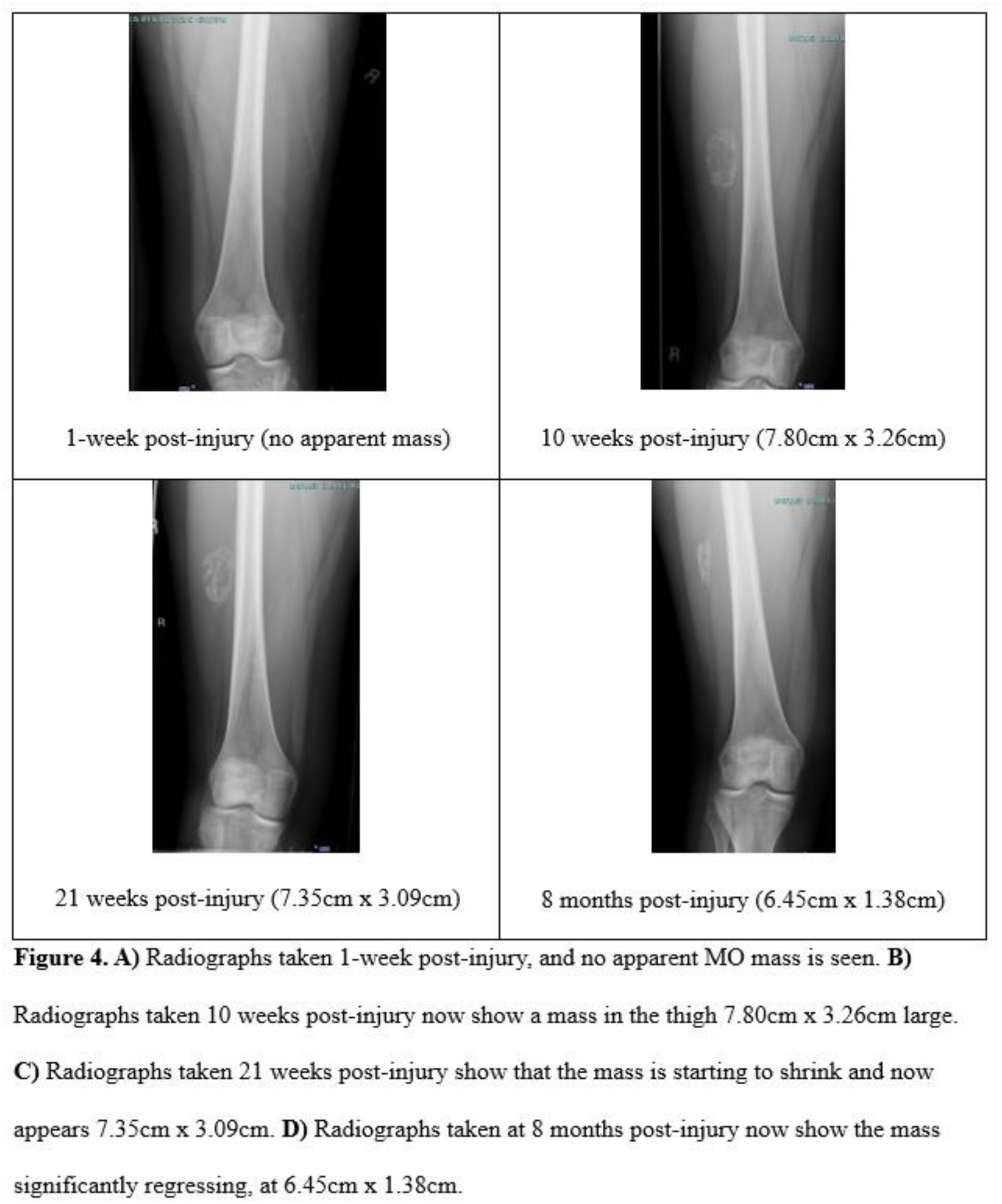
Sports-related injuries are common in adolescents, including muscular lesions. Myositis ossificans (MO) is an uncommon, but significant, sequela of muscle injury that is often misdiagnosed. A benign, localized, and self-limiting soft tissue mass, MO is characterized by the formation of heterotrophic bone within muscles, ligaments, and/or fascia, often leading to prolonged periods of disability. There is scant literature regarding the condition, particularly in the adolescent population.
Hypothesis:
The study hypothesis was that MO patients would return to sports (RTS) greater than 3 months following injury, with mean delays in diagnosis over 4 weeks.
Methods:
A departmental database was queried to identify all patients ≤19 years-old who presented between 2003-2024 ultimately diagnosed with myositis ossificans. Clinical, radiologic, and surgical data were retrospectively collected from medical records and analyzed.
Results:
83 patients (69 males, 83%; mean age 15.8 years, 96% athletes) met study criteria. Sixty-two 75% MO lesions occurred in the thigh. 76 cases (92%) were caused by a direct blow, muscle strain, or microtrauma, while 7 (8%) had an unknown origin. Six patients (7%) were originally given a neoplastic diagnosis, before ultimate diagnosis of MO, occurring approximately 4.6 weeks post-injury across the cohort. Common treatments included physical therapy (n=53, 64%), while shockwave therapy (n=5, 6%), intra-muscular/intra-lesional hematoma aspiration (n=3, 4%), and surgical excision (n=3, 4%) were relatively rare, with all operative patients reporting symptom resolution without peri-operative complications. Four patients (5%) developed complications, 3 of whom reported persistent pain and 1 with a postoperative fever requiring hospital admission but no intervention. RTS averaged 4 months post-injury, with all patients achieving RTS within 1 year.
Conclusion:
The vast majority of adolescent athletes with myositis ossificans were successfully treated non-operatively, though surgery may be beneficial in rare instances. Delays in diagnosis and prolonged periods of rehabilitation prior to RTS were not uncommon, making familiarity with the diagnosis and natural history of MO essential for sports medicine providers caring for young athletes.