Abstract
Background:
Imaging via radiology is considered the gold standard for diagnosing spondylolysis following a clinical exam. This study aimed to evaluate the diagnostic value of clinical exam maneuvers in identifying acute spondylolysis in adolescent athletes with low back pain as they relate to positive radiographic findings.
Hypothesis:
The addition of a single leg hop test alongside lumbar hyperextension pain on physical examination will increase sensitivity in predicting acute spondylolysis on MRI in pediatric and adolescent patients.
Methods:
Data was abstracted from a Musculoskeletal Registry that prospectively collects data from the electronic health record (EHR) for patients seen across a regional healthcare network. Patients aged 8–18 years presenting with lumbar back pain and who underwent a lumbar MRI between January 2019 and February 2024 were included. A standardized lumbar back pain physical assessment was performed. Demographic information, pain duration, radiographic findings, and responses to lumbar physical exam maneuvers were extracted from the EHR.
Results:
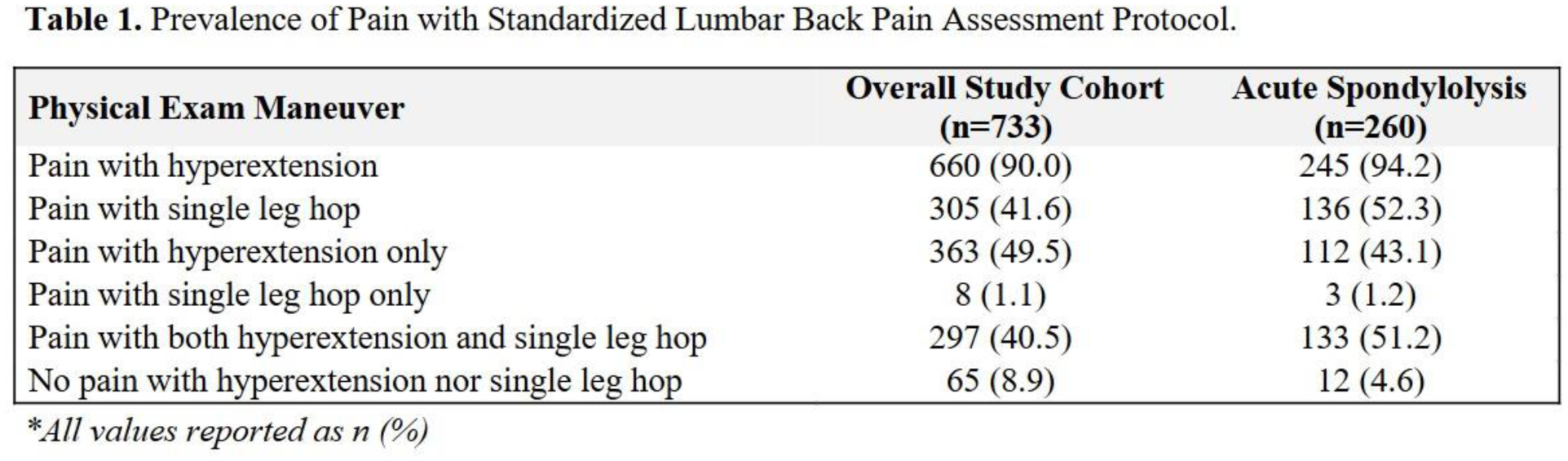
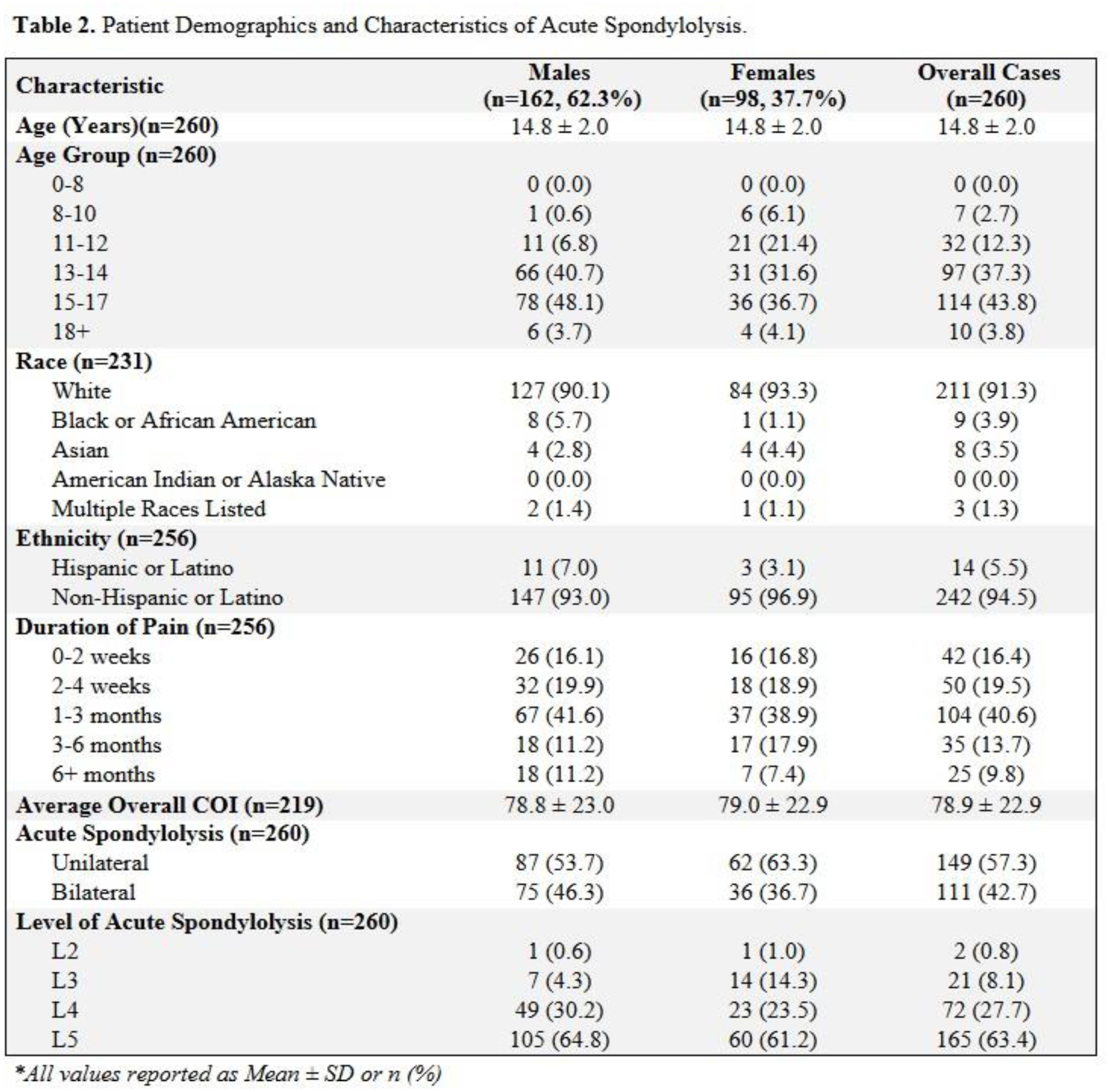
733 patients met study criteria, with 260 (35.5%) showing acute spondylolysis on MRI. The mean age at presentation was 14.8 years; most patients (40.6%) reported 1–3 months of lumbar back pain. Among patients with acute spondylolysis, 245 (94.2%) had pain with hyperextension of the lumbar spine, and 136 (52.3%) had pain during single leg hopping. 133 patients (51.2%) with spondylolysis reported both hyperextension and single leg hop pain, compared to 297 (40.5%) across the full cohort. Males had a higher prevalence (53.6%) of spondylolysis compared to females (22.7%). The 13–14 age group had the highest proportion of positive MRIs (97/240, 40.4%). Patients with 2–4 weeks of back pain had a 50% prevalence of spondylolysis (50/100). Among patients with both hyperextension and single leg hop pain, 44.8% (133/297) had spondylolysis, versus 30.9% with hyperextension pain alone.
Conclusion:
Hyperextension pain alone yielded a 30.9% sensitivity in detecting acute spondylolysis on MRI. When combined with single leg hop pain, the prevalence rose to 44.8%. These findings support incorporating single leg hop testing into the clinical exam in conjunction with hyperextension pain testing when evaluating for spondylolysis. Together with patient age, sex, symptom duration, and sport involvement, these exam findings can improve clinical decision-making and guide the need for advanced imaging.