Abstract
Background:
Pediatric sports medicine clinicians lack consensus on the diagnosis and management of youth athletes with isthmic spondylolysis (1). Thus, the Pediatric Research in Sports Medicine (PRiSM) Spine/Spondylolysis Research Interest Group (RIG) conducted a Delphi study among physicians with expertise in spondylolysis to inform clinical practice for youth athletes with spondylolysis.
Hypothesis:
We hypothesized that physicians would agree on the primary imaging modalities and that physical therapy (PT) would be recommended in the management of spondylolysis. We also hypothesized that there would be a lack of agreement on the timing for PT and the usage of bracing for spondylolysis management.
Methods:
Physicians with clinical and/or research expertise in spondylolysis were recruited to the Delphi panel through PRiSM and other sports medicine professional organizations. Panelists completed open-ended questions regarding the diagnosis, work-up, and management of spondylolysis in round zero to generate 107 closed-ended questions for rounds one and two. Participants rated questions on agreement and importance using a 9-point Likert scale. Agreement was set a priori at 80% (e.g., strongly agree/moderately agree/agree ≥ 80%, mildly agree/neutral/mildly disagree ≥ 80%, disagree/moderately disagree/strongly disagree ≥ 80%).
Results:
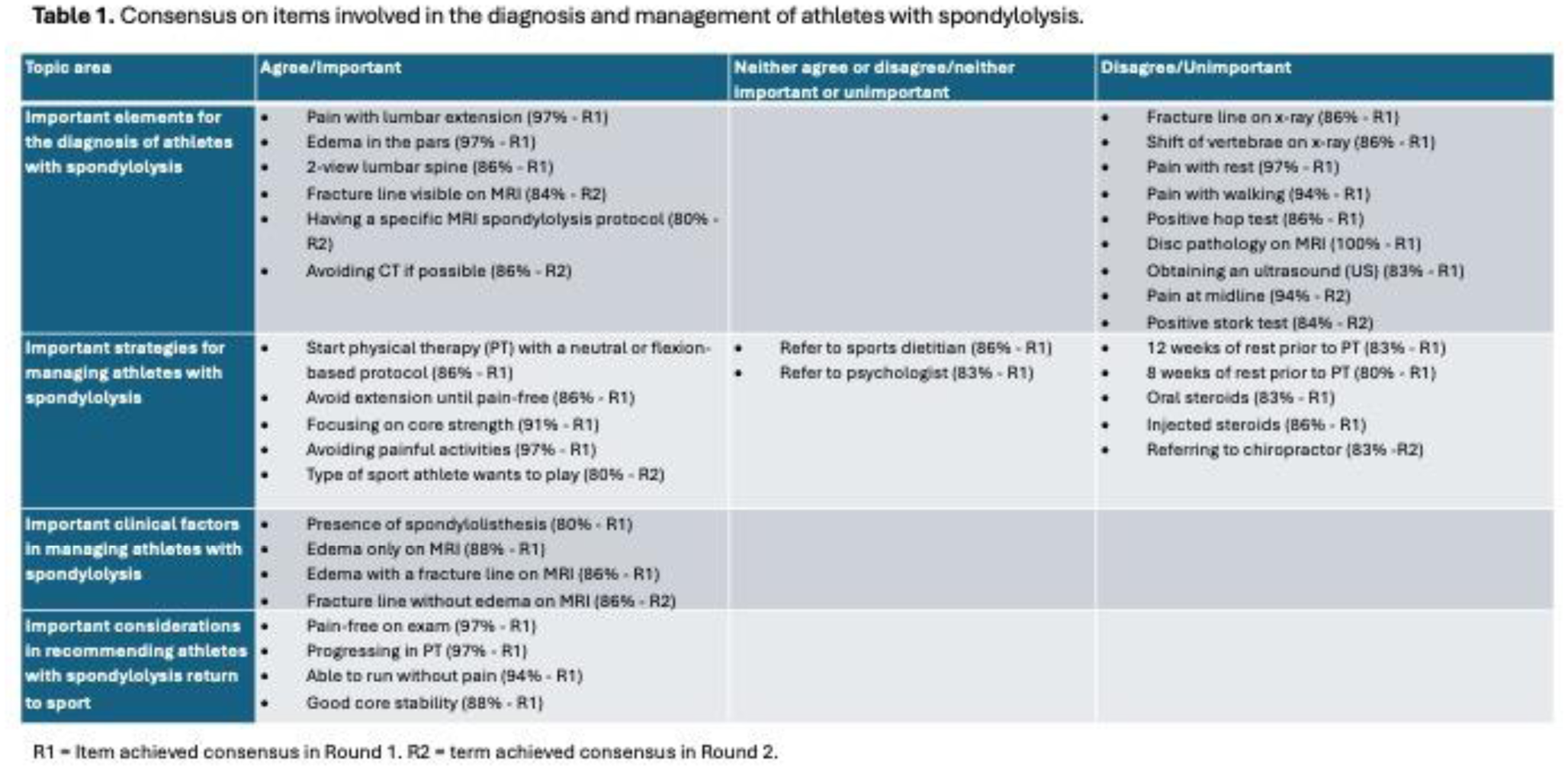
35 panelists (30 primary care sports medicine physicians and five pediatric spine surgeons) participated in Round 0 (R0) and Round 1 (R1), and 34 panelists completed Round 2 (R2). Thirty-three items met consensus in Round 1, and nine additional items met consensus in Round 2. Sixty-five items did not reach consensus after two rounds. Panelists agreed on a number of diagnostic criteria and management strategies for youth athletes with spondylolysis (Table 1). Physicians agreed that obtaining 2-view lumbar spine radiographs and seeing edema in the pars articularis on MRI is important in the diagnosis of spondylolysis. Panelists also agreed that patients do not need to wait 8-12 weeks to begin PT; however, there was no agreement on the most advantageous time to begin PT. Consensus on important considerations in recommending patients return to sport included: being pain-free on exam, progressing in PT, running without pain, and good core stability.
Conclusion:
Our study provides expert guidance on the optimal diagnostic and management strategies for youth athletes with spondylolysis. Higher-quality studies on the benefits of bracing and other specific management strategies would be beneficial in optimizing care for young athletes with spondylolysis.