Abstract
Background:
Upper extremity fractures are common orthopedic injuries observed in children who participate in sport. These injuries can increase risks of growth irregularities, early onset osteoarthritis, and functional limitations, posing challenges for pediatric athletes during their developmental years. Developing a better understanding of how upper extremity fractures are distributed among sport and age can help identify strategist to reduce the burden of injury on pediatric athletes.
Hypothesis:
Pediatric upper extremity fractures are more common in athletes engaged in collision or contact sports and their incidence is further influenced by age and sporting environment.
Methods:
Data was collected from the NEISS database from 2015-2024 for patients 5-18 years old with upper extremity fractures. Fractures were assessed by variables including age, sex, sport (NEISS Product Code), and categorical modifiers: collision/contact, team-based vs. individual sports, and environment setting (indoor/outdoor). Age groups were defined by developmental stage, based on literature from AJSM and AOSSM: Young Childhood (5–8yo), Late Childhood (9–11yo), Early Adolescence (12–14yo), and Late Adolescence (15–18yo).
Results:
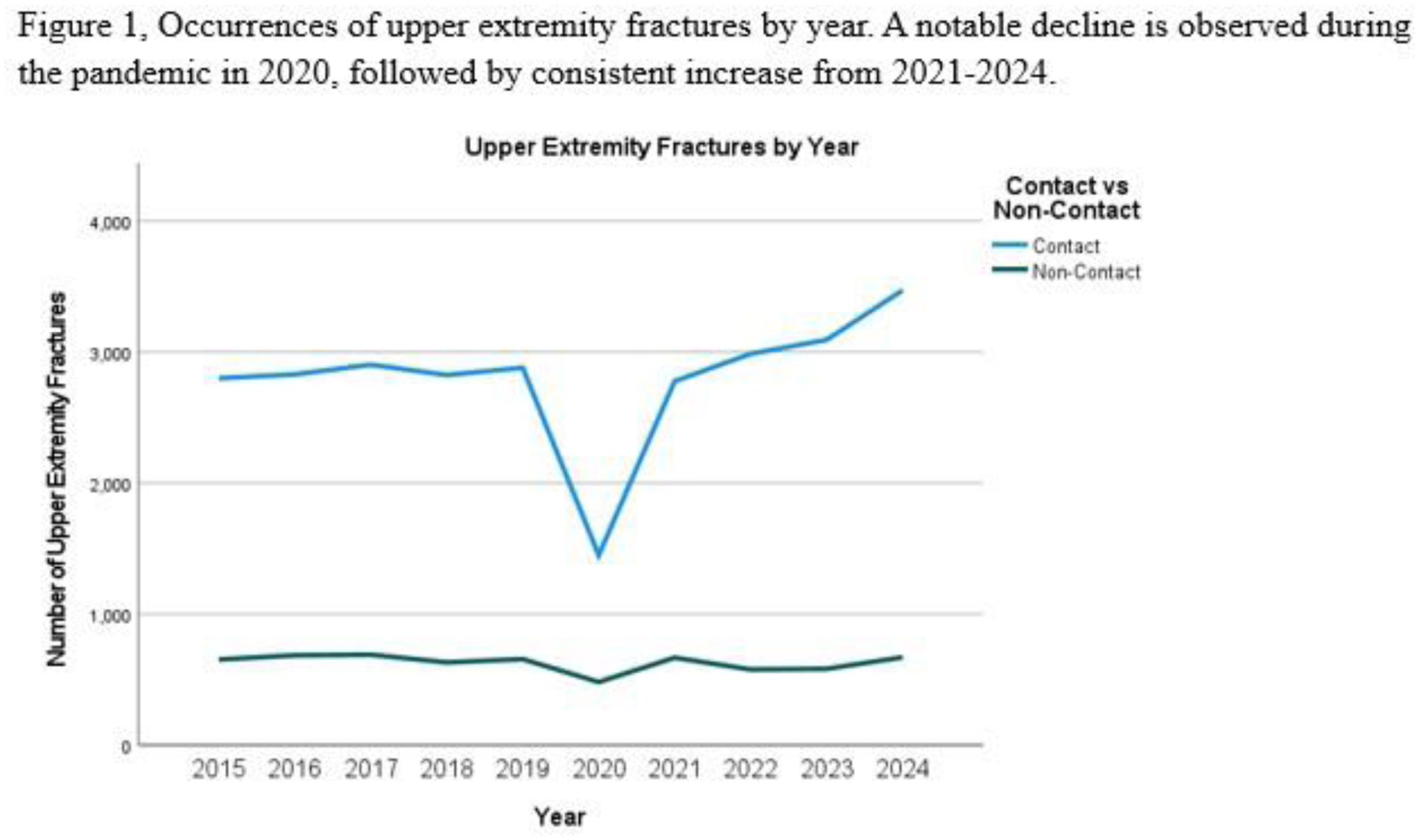
34,324 upper extremity fractures were identified. 74.8% of fractures presented in males. Incidence of fractures were highest in 2024 (4,134), with a significant decline noted during the pandemic in 2020 (Figure 1). Fractures most commonly occurred with football (9,142), soccer (6,197), and basketball (5,448). Non-collision sports accounted for 67.2% and contact sports accounted for 81.6%. Team sports and outdoor sports contributed 79.3% and 58.7% of fractures in their respective categories (team vs. individual sports and setting of sport played). Additionally, the age of injury peaked between 12-14 years old, with 39.8% of all fractures. Fractures had a higher incidence in the Fall Season (33.6%), followed by Spring (23.5%), Summer (22.3%), and Winter (20.6%).
Conclusion:
The results of this study demonstrate several factors that may influence the risk of upper extremity fractures in pediatric athletes. Physicians, coaches and athletic trainers should be encouraged to discuss risks of injury with athletes and the higher likelihood of upper extremity fractures that can be attributed to factors such as biological sex, contact vs. non-contact sports, and collision vs. non-collision sports. In doing so, athletes can be better prepared for their specific sport with training and protective gear that can help minimize the risk of upper extremity fracture. The results of this study help to better understand demographic based risks of upper extremity fracture in pediatric athletes and it supports the need for further developing sports safety policies in youth sports.