Abstract
Background:
Anterior cruciate ligament reconstruction (ACLR) leads to an abrupt cessation of physical activity due to post-operative restrictions and stepwise rehabilitation progressions. Persistent reductions in physical activity following ACLR may contribute to increased body mass index (BMI). At the time of return to sport (RTS) following ACLR, several factors, including changes in BMI, may influence patients’ perceived function and psychological readiness. The purpose of this study was to investigate the association between change in BMI from the time of surgery to the time of RTS test completion with self-reported knee symptoms, function, and psychological readiness to RTS after primary ACLR.
Hypothesis:
Our hypotheses were that individuals with greater increases in BMI would report worse knee symptoms and function and poorer psychological readiness at the time of RTS test completion.
Methods:
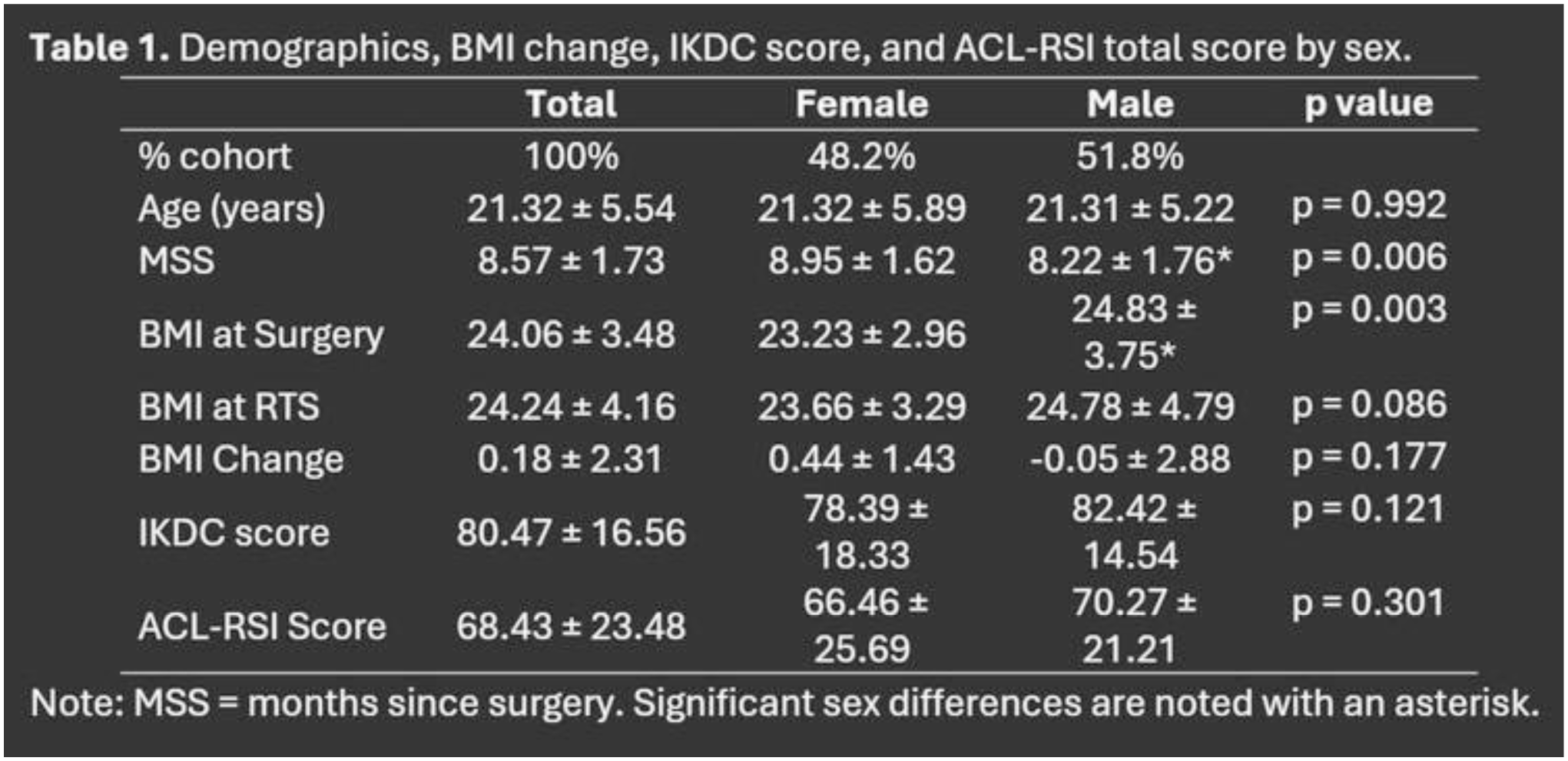
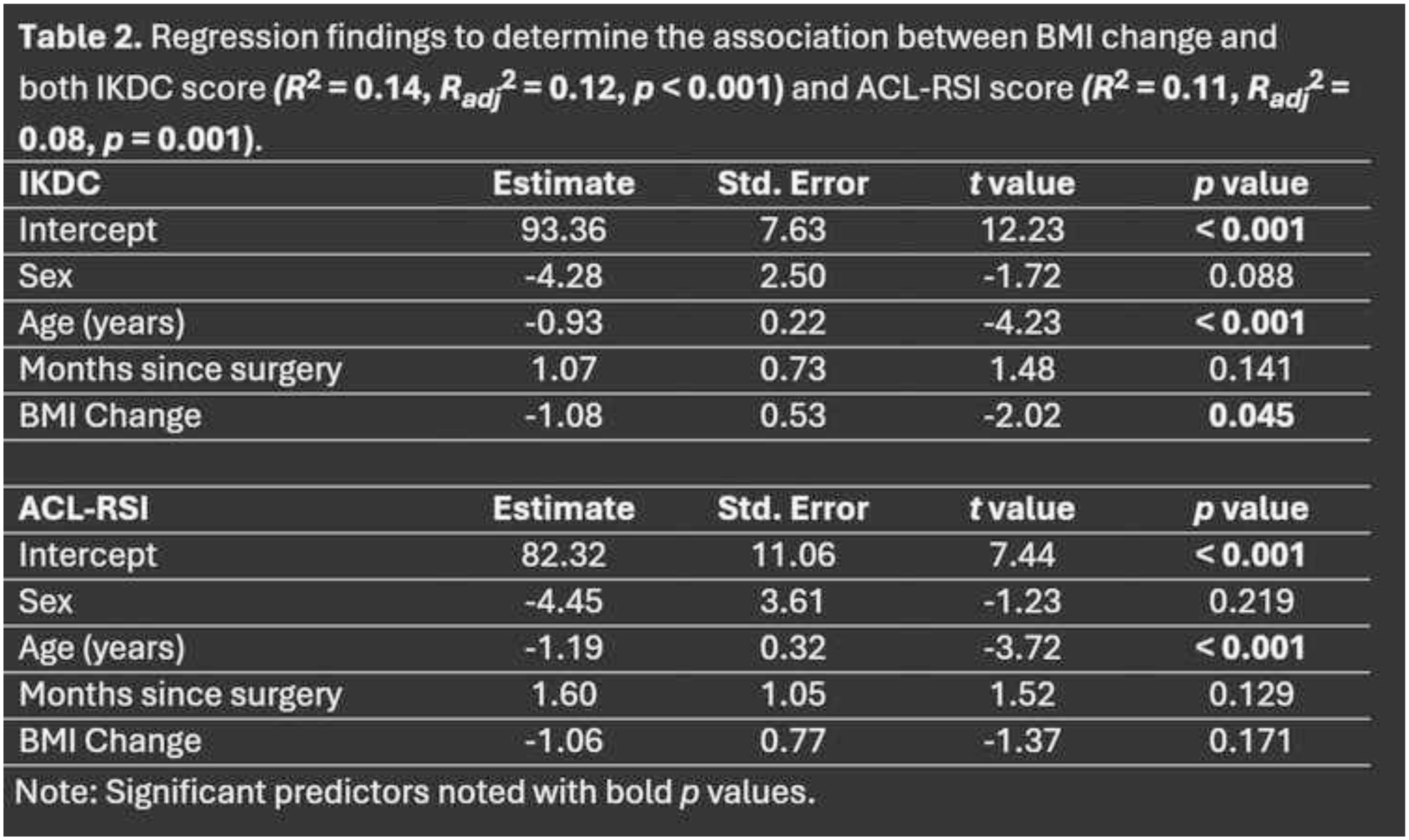
164 participants (48.2% female; 21.3±5.5 years; 8.6±1.7 months post-ACLR) were included from two sites in a multisite clinical outcomes registry. Participants completed the ACL Return to Sport after Injury Scale (ACL-RSI) and the International Knee Documentation Committee (IKDC) or the pediatric (Pedi)–IKDC subjective knee form at the time of RTS test completion. BMI change was calculated by subtracting BMI at surgery from BMI at the RTS test. Means and standard deviations were computed for all continuous variables. A paired samples t-test was performed to determine whether BMI at surgery differed from BMI at the time of RTS test. Finally, two linear regressions were performed to determine the association between the change in BMI and both IKDC score and ACL-RSI total score, with sex, age, and months since surgery as covariates.
Results:
There was no difference between BMI at surgery and at the time of RTS test. Females experienced significantly longer times from surgery to RTS test, and the BMI of male patients was significantly higher at surgery compared to females (Table 1). For each unit increase in BMI, IKDC score decreased by 1.1 points, but BMI change was not significantly associated with ACL-RSI score (Table 2).
Conclusion:
Increases in BMI after ACLR were associated with worse knee-related function but did not impact psychological readiness. However, given the small decrease in IKDC scores per unit increase in BMI, substantial increases in BMI would have to occur to surpass the minimal clinically important difference for the IKDC which ranges from 9-16.7 points. Thus, clinically meaningful reduction in knee symptoms and function may not be present.