Abstract
Background:
Morel-Lavallée lesions (MLLs) are degloving injuries from traumatic shearing forces. Multiple pathways exist for treating MLLs, including surgery, percutaneous aspiration, sclerodesis, and conservative methods. These lesions present differently in pediatric and adult patients, both in cause and location. There currently is no evaluated algorithm specific to pediatric and adolescent MLLs. Our goal was to describe the patient population, treatment pathways, and outcomes of pediatric MLLs to characterize the presentation and management of these injuries.
Objectives:
Patients receiving conservative nonsurgical management as initial MLL treatment would avoid the need for further invasive care via interventional radiology (IR) and/or surgery.
Methods:
Retrospective review was conducted on patients ages 8-25 treated for an MLL with at least three months of treatment from January 1, 2018, to September 31, 2024. Demographic information, lesion location, injury details, treatment modalities utilized by orthopedics, IR, plastic and general surgery, and patient outcomes were collected.
Results:
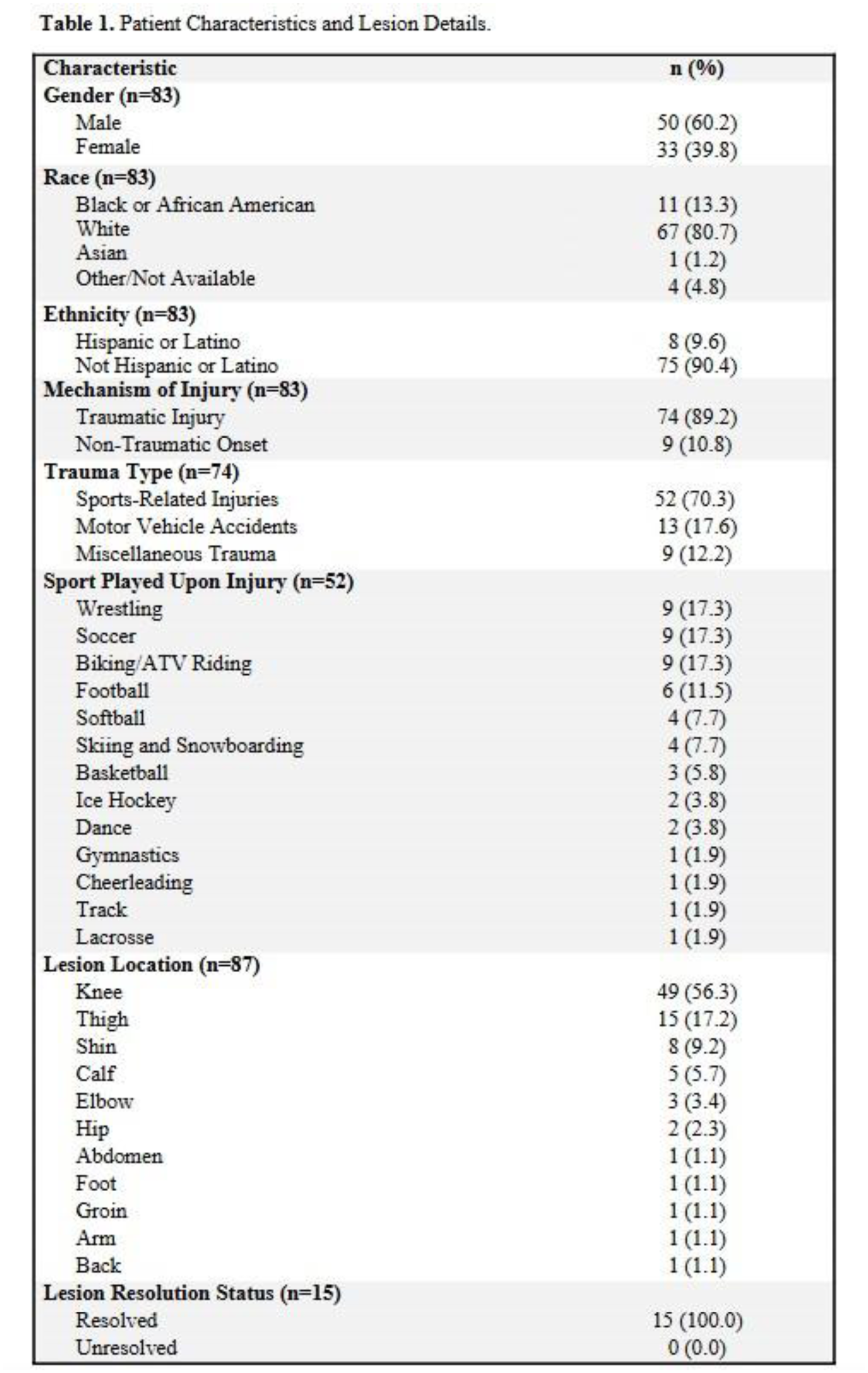
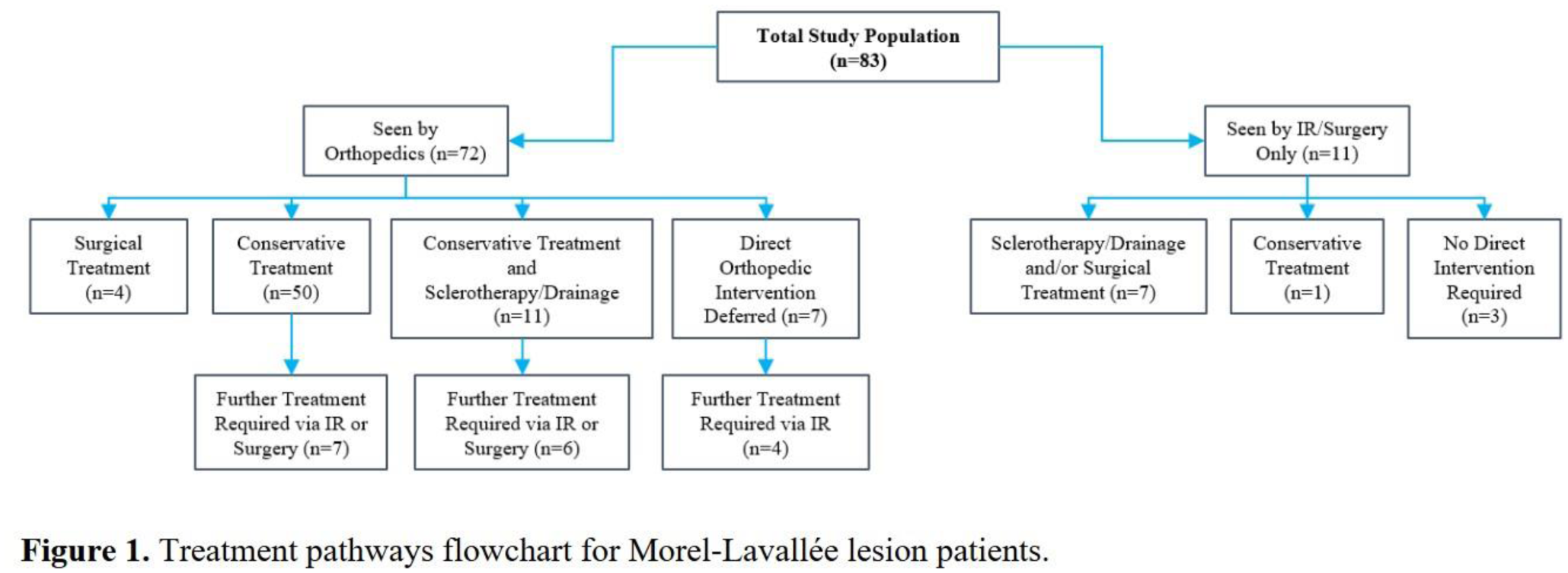
83 patients met study criteria, 74 with trauma-induced MLLs (89.2%), consisting of sports-related injuries (n=52, 70.3%), motor vehicle accidents (17.6%) and miscellaneous trauma (12.2%). 9 patients experienced non-acute/atraumatic onset. 87 total lesions were characterized, most commonly at the knee (n=49, 56.3%) and thigh (n=15, 17.2%). 72/83 patients (86.7%) were seen by an orthopedist, with the most common treatment being conservative management, consisting of targeted compression and/or other conservative measures, such as immobilization, weight bearing restrictions, and physical therapy referral (n=50). Of these, 7 patients (14%) required further treatment via IR or plastic/general surgery. Other orthopedic treatment included conservative care with drainage and/or sclerotherapy (n=11, 15.3%), surgery (n=4, 5.6%), or no orthopedic intervention (n=7, 9.7%). 11 patients (13.3%) were initially seen by IR or surgery and not orthopedics. Only 15 patients (18.1%) had sufficient clinical or radiographic documentation to confirm the status of lesion resolution. Of those 15 patients, however, 100% demonstrated full resolution.
Conclusion:
Traumatic sports injuries were the most prevalent cause of pediatric/adolescent MLLs, and the knee was the most common location. Most patients receiving conservative management did not require further IR or surgical treatment. Collaboration among specialties can ensure treatment progression is best suited to patients' needs. Maximizing follow-up to ensure resolution and prevent recurrence could improve outcomes from both clinical and patient satisfaction standpoints. Characterizing current treatment progressions for pediatric and young adults with MLLs and understanding how patient and lesion characteristics influence outcomes can help clinicians provide the most effective pathways.