Abstract
Background:
Traditionally, nonoperative care has been the standard treatment for adolescents with first-time patellar dislocations (1). However, some recent literature has suggested advantages of early operative stabilization (2,3). Deciding between these strategies can be challenging for parents who must weigh the competing advantages and disadvantages of each option.
Objectives:
We hypothesized that conjoint analysis, a form of discrete choice experiment, would offer insight into parental preferences for treatment of adolescents with first-time patellar dislocations.
Methods:
A survey was developed using Sawtooth Software (Lighthouse Studio version 9.2.0) to gather demographic information and preferences on surgical scenarios via choice-based conjoint (CBC) analysis. Anonymous participants, recruited through the Prolific crowdsourcing platform, qualified if they were adult U.S. residents with children aged 13-17. The Hierarchical Bayes (HB) method was applied to assess the desirability of six treatment attributes: risk of re-dislocation, persistent symptoms after treatment, risk of major complications, cost, time to return to normal activities, and likelihood of needing surgery. Specific levels (options) for each attribute were determined through a comprehensive literature review, and each scenario presented to participants combined these levels to simulate realistic treatment decisions.
Results:
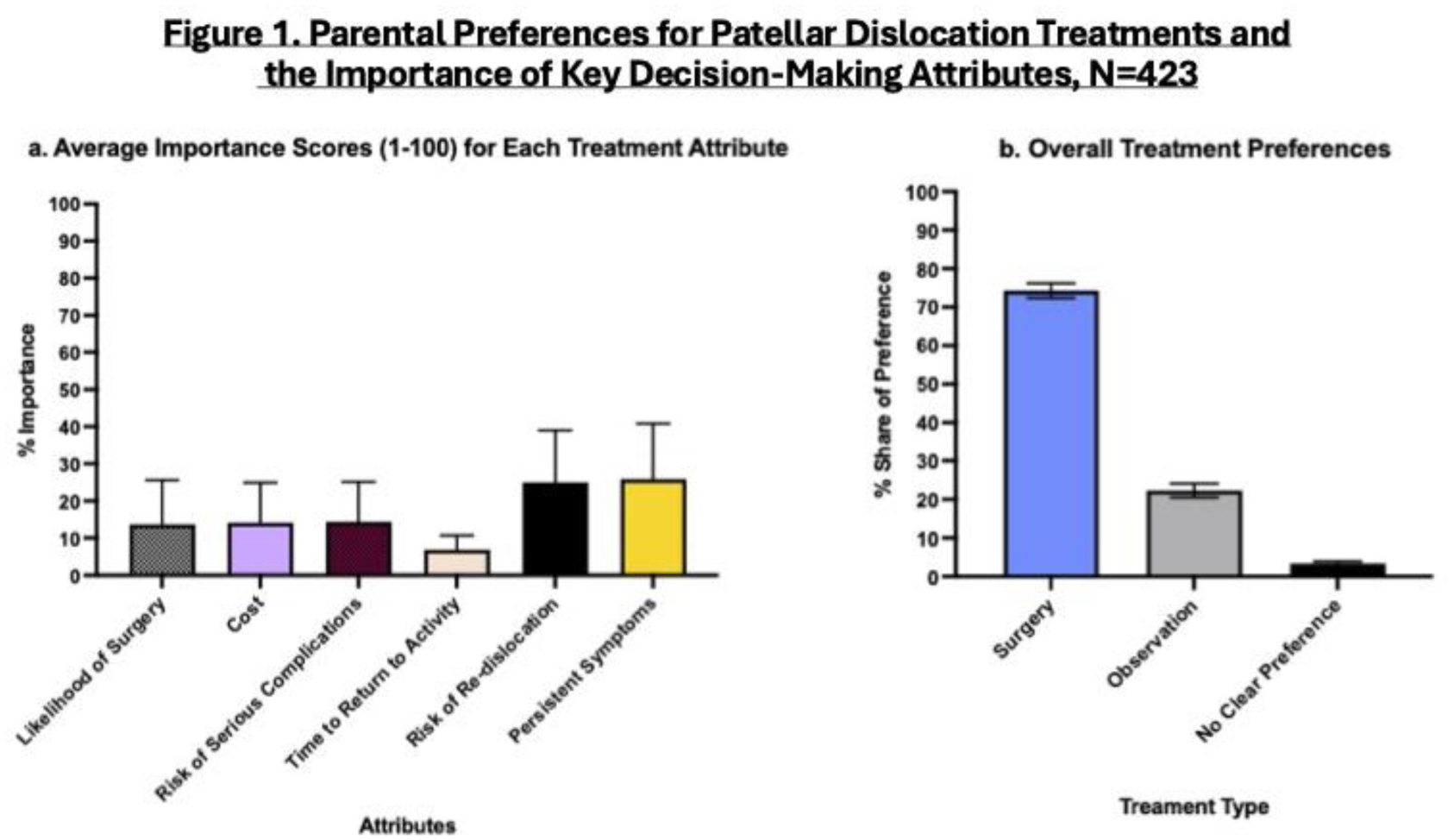
Among 423 participants, having persistent symptoms after treatment and the risk of re-dislocation emerged as the most critical factors in decision-making, with 25.9% and 25% importances respectively (Figure 1a). Surgery was preferred by 74.3% of participants, while 22.3% favored non-surgical options (Figure 1b). 3.3% of participants did not have a clear preference for either option. No major difference was identified among participants based on their demographics, though parents of female children assigned slightly lower utility to treatment courses with a lower likelihood of surgery (p = 0.039).
Conclusion:
These findings indicate a significant preference for surgical treatment as parents prioritized preventing recurrent instability and its associated complications. Only 3.3% of participants did not express a clear preference for surgical or non-surgical treatment, with the majority favoring surgery (74.3%) over non-operative care (22.3%). This trend illustrates the importance of communicating treatment options to parents during shared decision-making. Interestingly, participants with female children were less inclined to opt for a lower likelihood of surgery, suggesting a preference for more definitive treatment. These findings highlight the need for personalized treatment discussions and emphasize the importance of shared decision-making tools that take individual family values into consideration. Future research should focus on developing instruments to help these patients and parents choose a treatment course that accurately matches their values.