Abstract
Background:
Hip instability is increasingly recognized in pre-arthritic hip disease, especially among adolescent females. Generalized joint hypermobility (GJH), commonly defined as a Beighton score ≥5, may contribute to pre-arthritic hip instability, pain and surgical outcomes.
Objectives:
This study aimed to (1) assess the distribution of Beighton scores in an adolescent female population undergoing FAI surgery and (2) evaluate its role in patient-reported outcomes in this population.
Methods:
A prospective multicenter cohort of FAI patients undergoing primary hip arthroscopy was used to identify a subgroup of 97 adolescent females (aged 14–18.9 years) with FAI. Inclusion criteria were patients aged 14 to 18.9 years at the time of index surgery with FAI. Exclusion criteria were age ≥19, prior ipsilateral hip procedures, associated disorders, or Tönnis grade ≥2 osteoarthritis. Patients self-reported Beighton scores (0–9) and were grouped as follows: 0–3 (normal), 4-6 (borderline/mild GJH), and 7+ (moderate/severe GJH). Patient-reported outcomes (PROs) were collected at ≥1-year follow-up, including the modified Harris Hip Score (mHHS), HOOS Pain and Sports/Recreation, and iHOT-12. The mHHS was evaluated against the minimal clinically important difference (MCID) of 8 and the patient acceptable symptom state (PASS) of 74. Composite failure was defined as reoperation or failure to achieve either MCID or PASS. One-way ANOVA and chi-square tests compared groups for continuous and categorical measures, respectively.
Results:
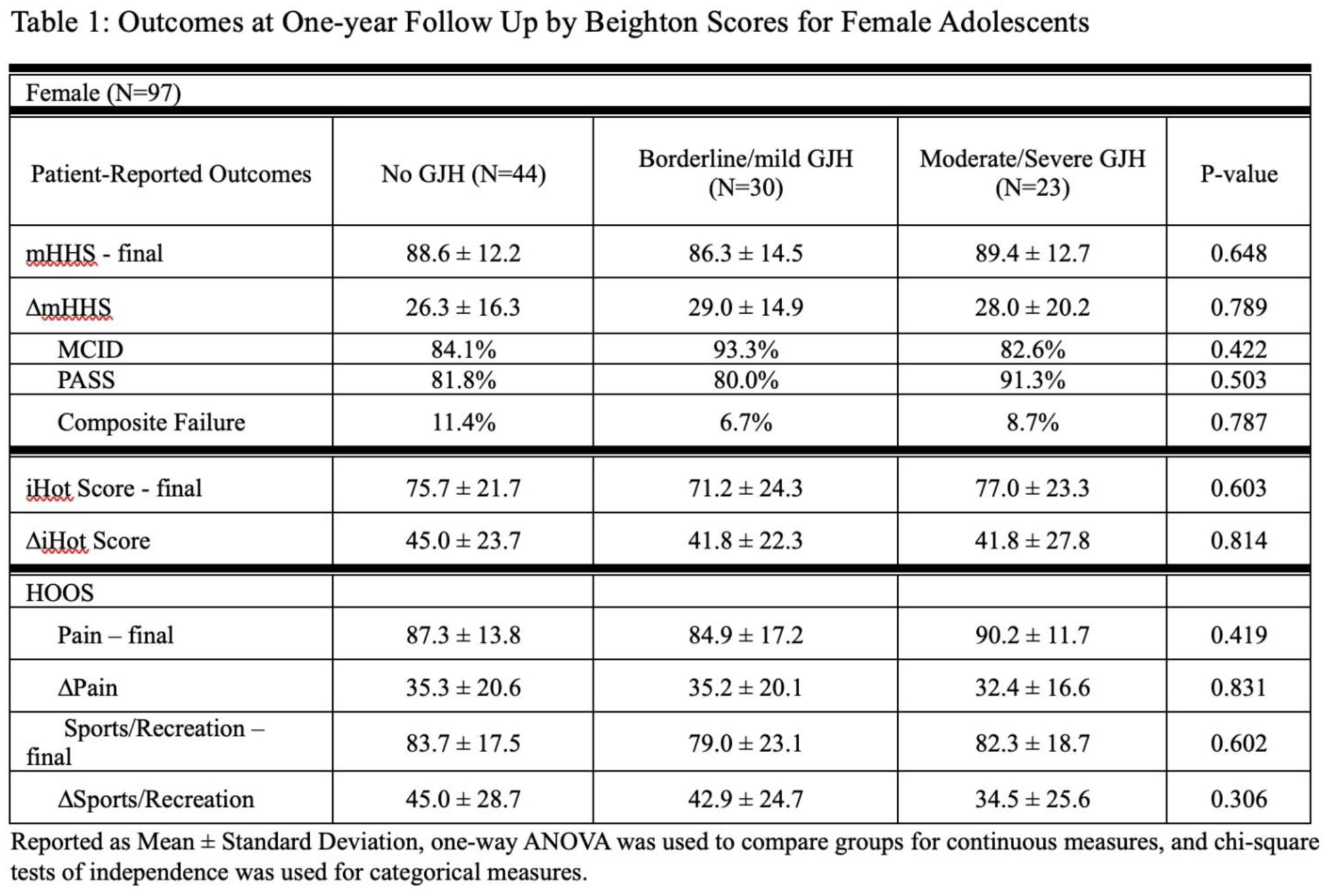
The final cohort included ninety-seven female patients from an initial group of one hundred forty-three adolescents, followed for an average of 1.1 ± 0.2 years. Beighton scores were normal in 45% of patients (0–3), borderline/mildly increased in 31% (4–6), and moderately/severely increased in 24% (7+). Elevated Beighton scores were not associated with worse FAI surgery outcomes. There were no differences in the final scores or changes in mHHS, iHOT-12, and HOOS scores, nor in rates of reaching MCID (82.6%-93.3%) and PASS (80.0%-91.3%) across different Beighton score groups. Non-GJH patients had the highest composite failure rates (11.4%), compared to moderate/severe GJH (8.7%) and mild/borderline GJH (6.7%), though differences were not significant (p = 0.787).
Conclusion:
Nearly half of adolescent females undergoing FAI surgery had elevated Beighton scores indicating generalized joint hypermobility. However, elevated Beighton scores were not linked to worse outcomes after FAI surgery in adolescent females in the setting of properly selected patients without underlying acetabular dysplasia.