Abstract
Background:
Medial patellofemoral ligament reconstruction (MPFLR) has become a standard treatment for patellofemoral instability (PFI). Tibial tubercle osteotomy (TTO) is often considered in skeletally mature patients with abnormally high tibial tuberosity–trochlear groove (TT-TG) distance, though precise indications remain controversial. Limited evidence exists for adolescents, despite being at highest risk for PFI.
Objectives:
Isolated MPFLR would provide comparable outcomes but fewer complications than MPFLR with concomitant TTO (MPFLR+TTO) in adolescents with TT-TG ≥ 20 mm.
Methods:
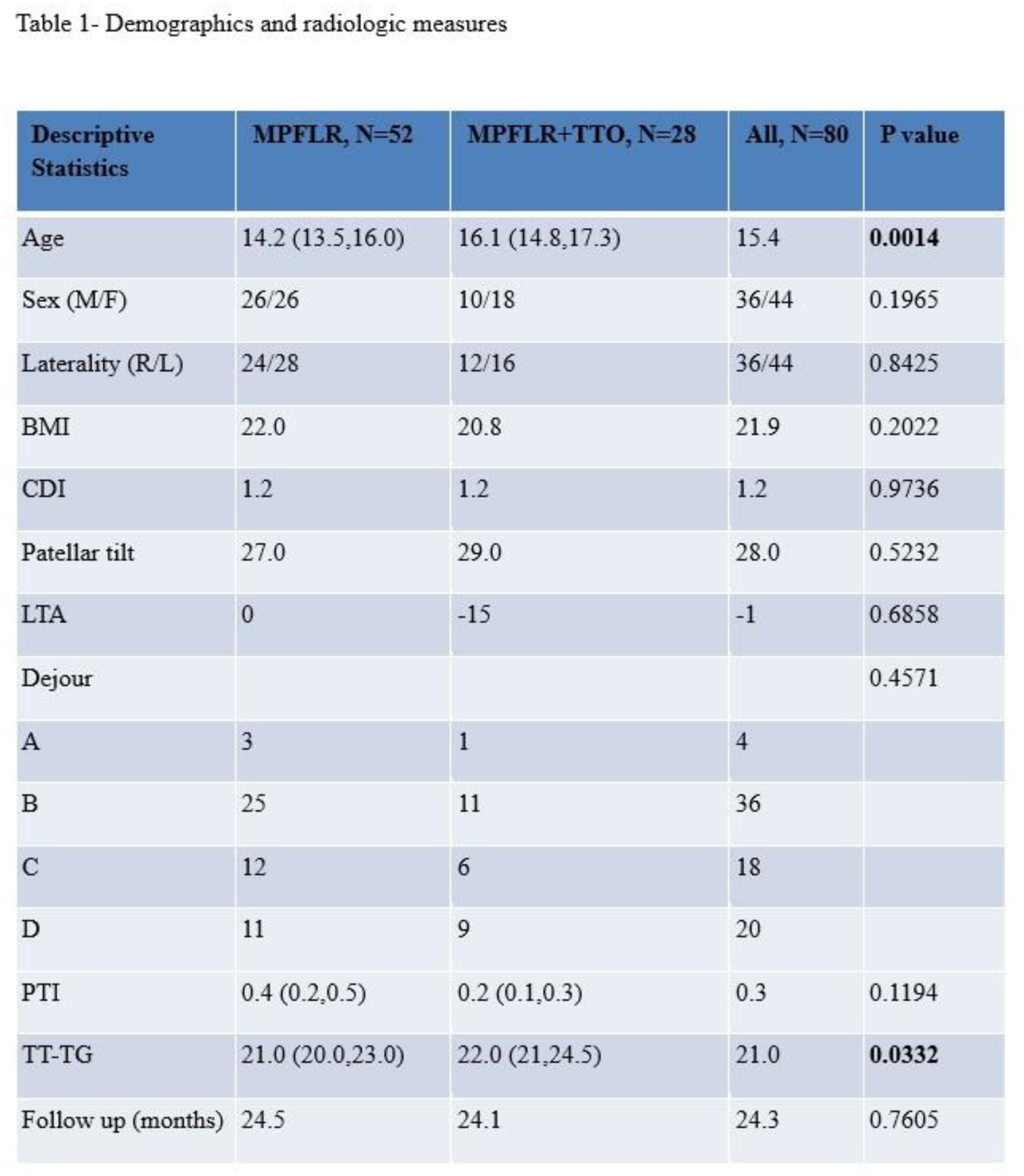
This single-institution retrospective cohort study with prospective survey data included skeletally mature adolescent athletes (ages 13–19) who underwent MPFLR ± TTO from 1/1/21–10/31/23. Inclusion criteria: TT-TG ≥ 20 mm, sports participation, and ≥1-year clinical follow-up data. Demographics, recurrent instability episodes, non-recurrence-related complications, reoperations, return-to-sport (RTS) rates and timing, and patient-reported outcomes (PROs: SANE, Pedi-FABS) were analyzed. Potential risk factors for recurrence such as age, body mass index (BMI), TT-TG, and patella alta (via Caton-Deschamps index, CDI, and patellotrochlear index, PTI), were further analyzed.
Results:
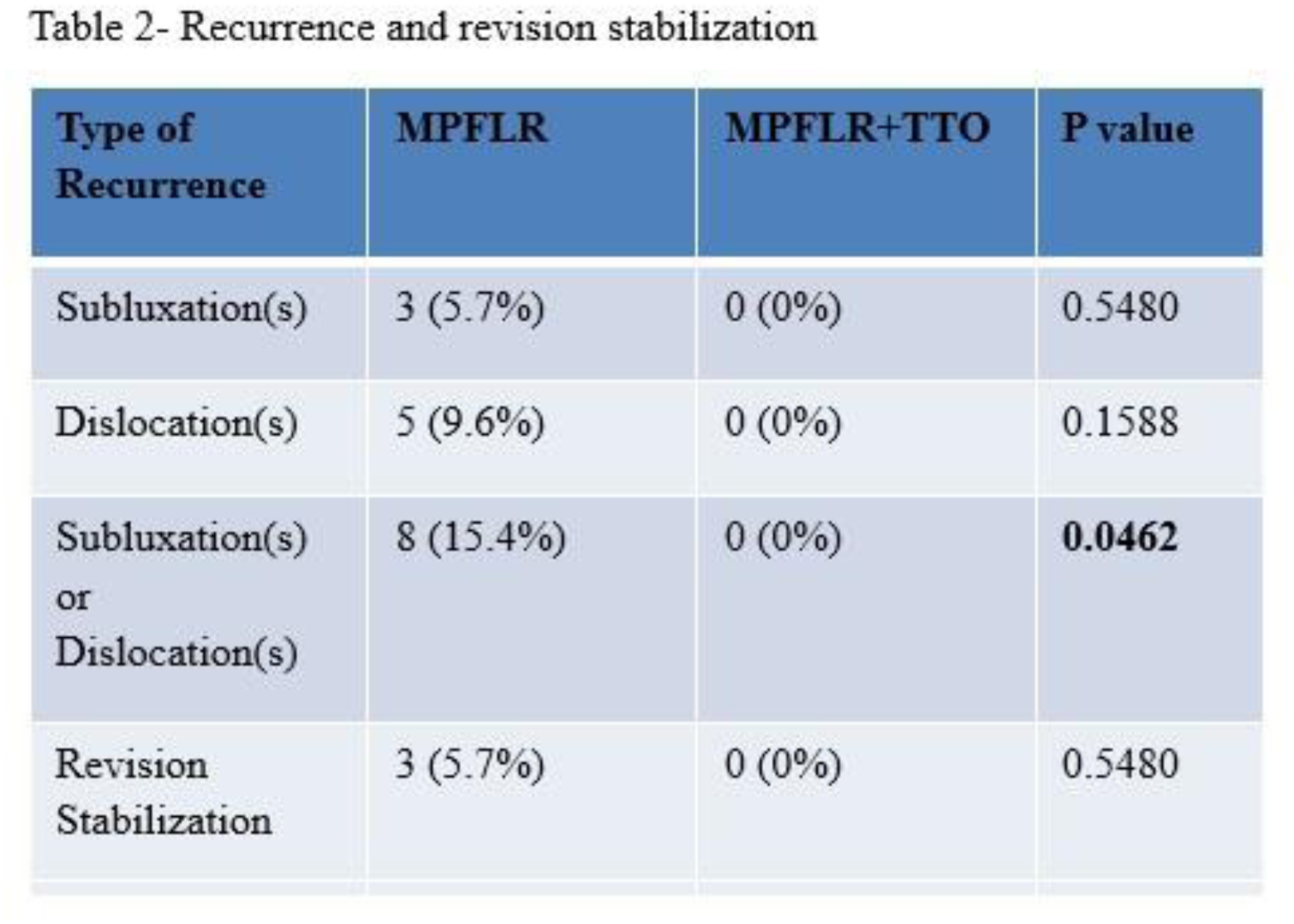
80 knees from 72 patients (52 MPFLR; 28 MPFLR+TTO) were included; median follow-up was 24.3 months. The TTO group was older (16.3 vs 14.2 years) and had slightly higher TT-TG (22 vs 21 mm). Recurrence occurred only in the MPFLR group (15.4% vs 0%, p=0.0462), as did revision (5.7% vs 0%, p=0.5480). Age, BMI, TT-TG, PTI, and CDI were not shown to be risk factors for recurrence or revision instability surgery. RTS was higher (87% vs 75%, p=0.2231) and earlier (6.2 vs 7.0 months, p=0.2257) in the MPFLR group. PROs were available in 37 patients (51%). PROs were collected in 37 individuals (51%) and the MPFLR and MPFLR+TTO cohorts demonstrated similarly minimal pain scores (median SANE 5.5 vs 11.0, respectively p= 0.0854), high levels of activity (median SANE 86.0 vs 88.0, p= 0.6983, and Pedi-FABS median 19.0 vs 14.0, respectively p=0.1020). Implant removal was more common in MPFLR+TTO (32% vs 0%).
Conclusion:
In adolescent athletes with abnormally high TT-TG values, isolated MPFLR is associated with similar PROs and RTS rates compared to MPFLR+TTO, with fewer implant-related complications. However, the isolated MPFLR group showed a higher rate of recurrence and revision, though no specific risk factors were identified. In the current era of evolving PFI techniques and research, the potential importance of TTO to lower recurrent PFI rates should not be underestimated in high-risk skeletally mature adolescent athletes. Further research is needed to improve risk stratification and guide individualized treatment.