
Abstract
Transgender individuals in Pakistan face physical and mental health challenges due to marginalization, discrimination, and victimization, which may increase their vulnerability to depression, anxiety, negative body image, and suicidal behaviors. This study aimed to examine the relationship between demographic factors, depression, anxiety, and low body appreciation with suicidal ideation, suicide attempts, and suicide risk among transgender individuals in Pakistan. Demographic variables included age, gender assigned at birth, gender identity, profession, education, and socioeconomic status, assessed through a self-developed semistructured questionnaire. Psychological constructs were measured using the Center for Epidemiological Studies Depression Scale, Generalized Anxiety Disorder-7, Body Appreciation Scale-2, and Suicide Behaviors Questionnaire-Revised. Reliability of instruments was evaluated through Cronbach’s alpha. Data were collected from 135 participants through respondent-driven sampling using both online and in-person interviews after informed consent, ensuring anonymity and privacy. Analyses included questionnaire validation, frequencies, descriptive statistics, mean comparisons, bivariate correlations, and logistic regressions. Results indicated that demographic factors significantly influenced suicidal ideation and attempts. Correlation analyses showed significant associations between depression (r = 0.071), anxiety (r = 0.147), low body appreciation (r = 0.110), and suicidal behaviors (r = 0.008). Depression, anxiety, and low body appreciation were significantly related to past suicidal ideation (R² = 0.395), attempts (R² = 0.376), and future suicide risk (R² = 0.415). Regression analysis further revealed that depression (adjusted odds ratio (AOR) = 1.024, p = 0.001) and low body appreciation (AOR = 1.071, p = 0.044) were associated with a higher number of past suicide attempts. These findings highlight the need for culturally sensitive mental health interventions for transgender individuals in Pakistan.
Introduction
Transgender individuals in Pakistan, known as Hijras or Khawaja Sira, face significant health and mental health challenges due to marginalization, discrimination, victimization, and body image concerns resulting from societal rejection and internalized stigma related to appearance (Kanwal, 2020). Their struggle for recognition and rights stems from historical misconceptions within a society that rigidly enforces binary gender norms (Ahmed and Yasin, 2020). Globally, transgender people encounter persecution, physical assault, and limited access to basic resources, which contribute to the development of mental health conditions such as anxiety and depression (Meyer, 2003; Trujillo et al., 2017; Valentine and Shipherd, 2018). Transphobia often results in violence, harassment, exclusion, unemployment, and restricted access to quality healthcare (Bhattacharya and Ghosh, 2020; Sartaj et al., 2021). In countries like Pakistan, where traditional gender roles are deeply embedded, transgender individuals experience systemic social rejection and marginalization (Jami and Network, 2011). Experiences of social rejection and lack of acceptance contribute significantly to the development and intensification of anxiety and depressive symptoms (Fatima et al., 2022; Majid et al., 2023; Suleman et al., 2023). Additionally, negative body image, shaped by societal pressures and unrealistic beauty standards, may be linked with reduced self-esteem and increased psychological distress (Akhtar and Bilour, 2020; Azam and Ayub, 2023). This cycle of body image dissatisfaction, social exclusion, and lack of validation can increase vulnerability to suicidal ideation and risk of suicide (Javaid et al., 2021). Moreover, the absence of adequate social support and access to mental health services further deepens this crisis, underlining the need for suicide prevention initiatives and comprehensive inclusive mental healthcare (Batool et al., 2022).
Depression and Anxiety Perspectives
A systematic review by Pinna et al. (2022) shows that transgender individuals are more likely to experience depression as compared to non transgender individuals (Pinna et al., 2022). A study by Budge et al. (2013) found that transgender individuals exhibit higher rates of anxiety (40.4%) and depression (51.4%), evaluated through the Beck Depression Inventory and Generalized Anxiety Disorder Scale (GAD-7) and explained through structural equation modeling (Budge et al., 2013). Similarly, Bouman et al. (2017) compared cisgender individuals to transgender individuals and revealed a nearly threefold increased risk of developing anxiety disorders in the latter group, primarily experiences of low self-worth and challenges in forming affirming social relationships. These findings emphasize the heightened levels of anxiety among transgender individuals and underscore the critical need to address self-esteem and interpersonal challenges (Bouman et al., 2017).
Empirical data also indicate that college students identifying as transgender, gender nonconforming, or belonging to sexual minority groups (such as pansexual or demisexual) report significantly higher levels of depression and anxiety than their cisgender or heterosexual counterparts. These disparities highlight the mental health challenges linked to discrimination, minority stress, and lack of inclusive support (Borgogna et al., 2019). A study by Gul et al. (2023) examining mental health among transgender individuals in Pakistan found high prevalence rates of both anxiety and depression. Utilizing the Siddique Shah Depression Scale and the State-Trait Anxiety Inventory, the study assessed 100 transgender individuals and revealed that 60% experienced moderate to severe depression, while 92% reported anxiety. Participants often used coping strategies such as emotional withdrawal and avoidance, reflecting responses to chronic stress (Gul and Mohsin, 2023).
In another Pakistan-based study, Rao Azeem et al. (2019) highlighted a strong association between depression and suicidal ideation among the transgender individuals, indicating that individuals suffering from depression were significantly more likely to report suicidal thoughts (Rao Azeem et al., 2019). Additionally, Chodzen et al. (2019) examined the mental health of transgender and gender nonconforming (TGNC) adolescents and found strong correlations between higher internalized transphobia and distress from incongruence between gender identity and appearance were linked with anxiety and depression. The study emphasized the urgent need for targeted interventions to support TGNC youth facing these challenges (Chodzen et al., 2019).
Low Body Appreciation
Low body appreciation, defined as a lack of positive regard for one’s body, is a significant psychological concern among transgender individuals. It reflects internalized dissatisfaction and self-criticism influenced by societal ideals of beauty and appearance norms. In this study, low body appreciation is examined as a potential correlate of suicide-related outcomes, including ideation, attempts, and future risk.
Although research directly linking low body appreciation with suicide is still emerging, available evidence suggests that individuals with low body appreciation often experience higher levels of depression, anxiety, and emotional distress, all of which are known contributors to suicide risk. In this context, low body appreciation may interact with other psychosocial vulnerabilities, potentially contributing to increased suicide risk. The findings of this study underscore the importance of addressing body image concerns within suicide prevention efforts and promoting positive embodiment and self-acceptance as protective mental health strategies for transgender individuals.
For example, Jessica et al. investigated body image concerns and depressive symptoms among both transgender and cisgender individuals, finding that the internalization of cultural beauty standards contributes significantly to body image dissatisfaction across both groups. Transgender women, in particular, reported higher levels of body-related distress and depressive symptoms compared with cisgender individuals (Strübel et al., 2020). Similarly, Williams (2017) examined the impact of body image on the mental health of the transgender population and concluded that transgender individuals experience a disproportionately high rate of suicide attempts, with body image dissatisfaction identified as a contributing factor.
In another study, Jenifer et al. explored perceptions of physical appearance among transgender individuals and emphasized how self-perception and societal feedback jointly shape levels of body satisfaction. The study found that low body appreciation, manifested as a lack of respect and acceptance for one’s body, significantly affected psychological well-being and contributed to emotional distress (McGuire et al., 2016). This body of literature supports the critical role of low body appreciation and related body image concerns in shaping mental health outcomes and influencing suicide risk among transgender individuals.
Demographic Variability in Suicide
The age factor is a significant concern, as younger transgender individuals may encounter unique challenges related to social acceptance and access to essential healthcare interventions (Bariola et al., 2015). This is particularly relevant for younger transgender individuals, who often face limited social and familial acceptance and struggle to access necessary medical and mental healthcare (Connolly et al., 2016). The discordance between gender identity and assigned sex at birth is associated with elevated mental health risks and increased stress in navigating social and medical systems (Meyer, 2003). Transgender people often experience stress and psychological difficulties due to the disparity between their gender identity and their assigned sex at birth. Societal rejection and discrimination further aggravate this distress, contributing to higher rates of anxiety and depression (Coleman et al., 2012).
Moreover, these mental health issues are exacerbated by ongoing experiences of discrimination and restricted access to supportive healthcare, which underscores the need for gender-diverse and inclusive health policies (Domínguez-Martínez and Robles, 2019; Katz-Wise et al., 2017). A review article highlights that inadequate education in transgender healthcare is associated with poorer health outcomes and heightened psychological distress, which may increase the risk of suicidal ideation and behaviors (Korpaisarn and Safer, 2018).
Education and occupational status have been significantly associated with suicidal behaviors among transgender individuals. Limited access to higher education and economic marginalization, often leading to engagement in informal or vulnerable forms of employment, have been linked to increased psychological distress and a higher incidence of suicidal ideation and attempts. These findings emphasize the necessity of implementing comprehensive educational policies and creating supportive employment opportunities to mitigate the risk of suicide within this vulnerable population. Community-based participatory research among transgender communities further supports the influence of sociodemographic variables, particularly education and profession, on mental well-being. This aligns with prior findings that transgender individuals face elevated risks of suicide due to pervasive discrimination and restricted access to educational resources. The combined effect of limited educational opportunities and engagement in marginalized professions is associated with poorer mental health outcomes and greater risk for suicidal ideation and behaviors (Smith et al., 2018).
Access to healthcare is also significantly influenced by socioeconomic status. Transgender individuals with lower socioeconomic standing encounter greater obstacles in obtaining high-quality, affirming healthcare (Khan, 2022). Literature suggests that financial hardships worsen transgender individuals’ overall living conditions and amplify their exposure to prejudice and victimization, leading to poorer health outcomes. Transgender individuals with lower incomes frequently face healthcare discrimination and limited access to medically necessary procedures (Asghar et al., 2022; Carpenter et al., 2020; Jabeen et al., 2021; Khan, 2022; Omer et al., 2021).
Research Gap
There is an increasing amount of research on transgender mental health issues, such as body image concerns, low body appreciation, depression, and anxiety. However, there remains a significant gap in understanding how these factors are associated with suicide, particularly in Pakistan, where transgender individuals commonly referred to as Hijras or Khawaja Sira experience systematic marginalization. While previous studies have established links between suicidal ideation and mental health disorders such as depression and anxiety, limited research has investigated how low body appreciation, in combination with these psychological factors, may elevate suicide risk in this population. Much of the existing literature is situated in Western contexts, making it challenging to interpret these dynamics from a sociocultural perspective relevant to transgender individuals in Pakistan.
Hypothesis and study aims
This study hypothesizes that transgender Pakistani individuals with higher levels of depression, anxiety, and low body appreciation are more likely to experience suicidal thoughts and attempt suicide. It is further hypothesized that having a lower socioeconomic status and younger age may intensify mental health issues and increase suicide risk. A correlation between depression, anxiety, low body appreciation, and suicidal ideation, attempts, and risks is anticipated.
This research aims
To identify whether experiences of low body appreciation, along with anxiety and depression, are associated with suicidal ideation, attempts, and overall suicide risk among transgender individuals in Pakistan.
To investigate the impact of demographics such as age, gender assigned at birth, identified gender, profession, education, and socioeconomic status on suicide among transgender people in Pakistan.
Methodology
Study design
This study employed a cross-sectional survey design, conducted through both online and in-person interviews in Lahore, Pakistan, over a six-month period from July 2023 to December 2023.
Recruitment
Participants included individuals who self-identified as transgender men or women. Those not meeting the inclusion criteria were excluded. Recruitment was conducted through a mixed approach: in-person outreach at roads and traffic signals where some transgender individuals engage in street begging for survival (John et al., 2021) and online using social media platforms such as Grindr, Blued, Hornet, and specific Facebook groups. The online questionnaire was created using Google Forms and was shared and communicated through these social media platforms to reach eligible participants. The detailed description is available in Figure 1.
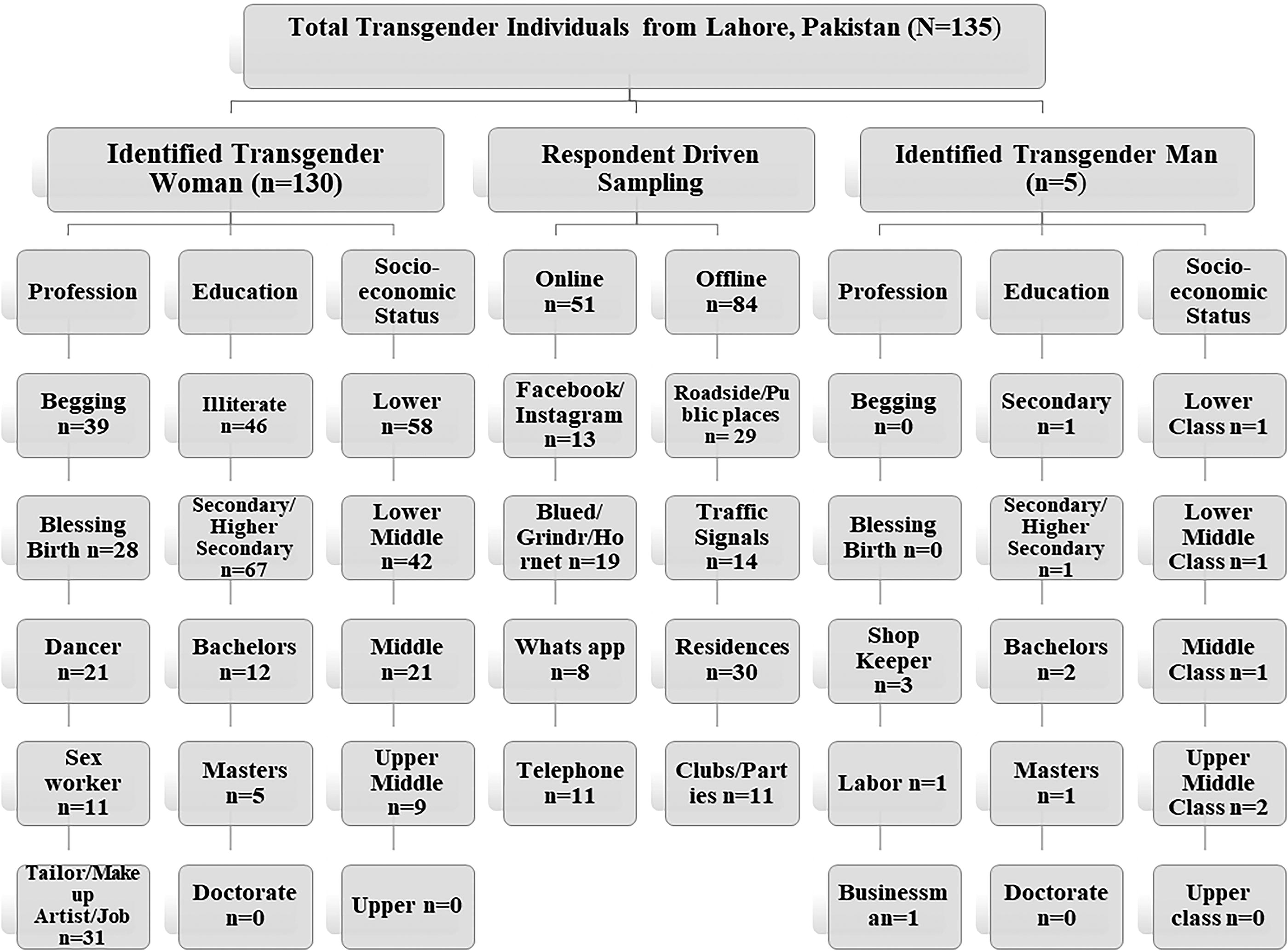
Data collection process and distribution of participants.
For online participants, eligibility screening questions were included in the Google Form to confirm age (16–50 years), gender identity, and that participants had identified as transgender for more than one year. The form was set to “limit to 1 response” to prevent multiple submissions, and responses were reviewed for inconsistencies, short completion times, or suspicious patterns. Any responses that appeared invalid were excluded from the final dataset.
While some participants opted for in-person interviews, others preferred telephone interviews due to fear and stigma. Anonymity and privacy were ensured throughout the process. Eligible participants were self-identified transgender individuals aged 16–50 years. Participants who had identified as transgender for over one year were included to ensure stability in gender identity and reduce variability from early transitional phases. Data were collected using a respondent-driven sampling (RDS) approach, with a total of 135 participants recruited through a combination of in-person and online methods. This strategy was adopted due to practical constraints and the challenges of accessing this marginalized population in Pakistan.
Ethical considerations and consent
Ethical approval was granted by the institutional review board of The University of Lahore, Gujrat Campus (Reference number: REG/GRT/24/AHS-02). The research adhered to all relevant ethical standards, including those outlined in the Declaration of Helsinki and institutional ethical guidelines. These included ensuring voluntary participation, obtaining informed consent, maintaining participant confidentiality, and implementing protocols for safeguarding participants’ mental well-being during discussions of sensitive topics such as suicide and mental health. Informed consent was obtained before participation through Google Forms for online interviews, verbal confirmation during telephone interviews, and written consent for in-person participation.
For participants under the age of 18, additional consent was obtained from their parents or Gurus (traditional guardians), ensuring ethical compliance and protection of minors.
Given the sensitive nature of the study, protocols were in place to safeguard participants’ emotional well-being. Any individual showing signs of emotional distress or suicidal thoughts during the interview was provided immediate emotional support. The researcher offered on-the-spot counseling guidance and, with the participant’s consent, referred them to professional mental health services or local support networks.
Participants were informed that participation was voluntary and that they could withdraw at any point or skip any question without consequences. All collected data were anonymized and securely stored, ensuring full confidentiality and privacy protection.
Measures
The questionnaire tools for evaluation included the Center for Epidemiological Studies Depression Scale (CES-D) (Radloff, 1977), the GAD-7 Anxiety Updated Scale (Spitzer et al., 2011), the Body Appreciation Scale-2 (BAS) (Tylka and Wood-Barcalow, 2015), and the Suicide Behaviors Questionnaire-Revised (SBQ-R) (Osman et al., 2001). These tools were selected based on their established reliability and validity, as well as their prior use among diverse populations.
Demographics
Demographic variables included age, gender assigned at birth, identified gender, profession, education, and socioeconomic status. Socioeconomic status was classified based on self-reported monthly income in Pakistani Rupees (PKR). A low socioeconomic status was defined as earning less than 10000 PKR per month, while a high status was defined as earning up to 60000 PKR per month.
Education levels were categorized into five groups: Secondary School Certificate, Higher Secondary School Certificate, Bachelors, Masters, and Doctorate. These variables were collected via self-reporting during interviews and questionnaire responses, with full assurance of anonymity and privacy.
Depression
The CES-D scale was employed to assess depressive symptoms. Responses were rated on a 4-point Likert scale: 0 = “rarely or none of the time (less than 1 day),” 1 = “some or a little of the time (1–2 days),” 2 = “occasionally or a moderate amount of time (3–4 days),” and 3 = “most or all of the time (5–7 days).”
The questionnaire was translated into Urdu. In Pakistani populations, the Urdu version of CES-D has demonstrated solid psychometric properties, with an internal consistency of 0.73. It also showed convergent validity with the Strength and Difficulty Questionnaire, yielding a Pearson correlation coefficient of 0.54 (p < 0.01) (Mustafa and Maqsood, 2021). In the current study, Cronbach’s alpha was calculated as 0.86, indicating strong internal consistency.
Anxiety
The GAD-7 Anxiety Scale was used to assess the severity of GAD symptoms experienced over the past two weeks. Participants responded on a scale from 0 to 3, where 0 represented “Never” (less than one day), 1 represented “Some or a little of the time” (1–2 days), 2 indicated “Occasionally or a moderate amount of time” (3–4 days), and 3 reflected “Most or all of the time” (5–7 days).
The questionnaire was translated into Urdu. The GAD-7 scale demonstrated strong psychometric properties, including excellent internal consistency and reliability in the Pakistani population (Urdu version: Cronbach’s alpha = 0.92). It also showed convergent validity with the Strength and Difficulty Questionnaire, with a Pearson’s correlation coefficient of 0.44 (p < 0.001) (Ahmad et al., 2017). The present study further assessed internal reliability, yielding a Cronbach’s alpha of 0.85, indicating a substantial degree of internal consistency.
Body appreciation
The study employed the BAS-2 to assess participants’ perceptions, attitudes, and sentiments toward their own bodies. The BAS-2 consists of 10 items, each rated on a 5-point Likert scale ranging from 1 (never) to 5 (always). Lower scores on this scale indicate lower levels of body appreciation, which in this study is used to reflect negative self-evaluation and diminished positive regard for one’s physical appearance.
The BAS-2 was selected for its relevance in evaluating body-related psychological experiences. It captures how individuals perceive, value, and accept their bodies, making it suitable for understanding internalized negative body perceptions within marginalized populations. In the context of this study, low body appreciation is conceptualized as a psychological construct that reflects internal discomfort, self-critical attitudes, and discontent with one’s body, shaped by societal standards, gender-based expectations, and experiences of social rejection.
According to a prior study in Pakistan, the BAS-2 demonstrated strong psychometric properties, with internal consistency and reliability reported at 0.77 (Naz et al., 2023). In this study, the Cronbach’s alpha was found to be 0.88, indicating a high level of internal consistency.
Suicide
The suicidal attempts, suicidal thoughts, and suicide risks were evaluated using the SBQ-R. This questionnaire consists of four items, with total scores ranging from 3 to 18, based on values assigned to responses in each category. Item 1 assesses lifetime suicidal ideation and attempts, scored from 1 (“never”) to 5 (“very often”). Item 2 measures the frequency of suicidal ideation over the past 12 months, scored from 1 (“never”) to 5 (“very often”). Item 3 inquires about the lifetime history of suicide attempts, with responses scored from 0 (“never”) to 6 (“4 or more times”). Item 4 evaluates the likelihood of future suicidal behavior, scored from 0 (“never”) to 6 (“very likely”). The total SBQ-R score is calculated by summing the responses to all four items, with higher scores indicating greater suicide risk. A cutoff score of 7 or above is commonly used to identify individuals at risk of suicidal behavior. Item 3 specifically captured the lifetime frequency of suicide attempts; however, the exact timing of these attempts (e.g., before or after gender identity acknowledgment) was not recorded. Although participants reported the duration since they began identifying as transgender, the relationship between this duration and suicidal behaviors was not examined in the current analysis.
A study conducted in Pakistan employed the SBQ-R and found it to have good internal consistency (Anwar et al., 2022). Another study from North India, a region with sociocultural similarities to Pakistan, also utilized the tool and reported a Cronbach’s alpha coefficient of 0.80, reflecting high reliability (Garg et al., 2022). The current study also found a high alpha coefficient value of 0.80 showing a high degree of internal consistency across the scale components.
The flow chart (Fig. 1) illustrates the data collection process from 135 transgender individuals in Lahore, Pakistan, using respondent-driven sampling. The sample is divided into two groups: transgender women (n = 130) and transgender men (n = 5). The recruitment strategy combined offline (n = 84) and online (n = 51) methods. These methods involved identifying participants’ specific locations and preferred modes of communication and interaction. The figure also presents the evaluation of transgender men and women across three key categories: profession, education, and socioeconomic status. Sub-blocks within each category provide detailed insights into the circumstances and lived experiences of the surveyed transgender individuals.
Data analysis
The data analysis was conducted on SPSS version 22. The frequencies and descriptive statistics were conducted for age, gender at birth, and gender identity. The study conducted a Pearson’s bivariate correlation analysis between the variables age, depression, anxiety, low body appreciation, and suicide. To test the hypothesis that depression, anxiety, and low body appreciation contribute to the cross-sectional association of each suicide-related outcome (ideation, attempts, and risks), bivariate logistic regressions were conducted, and Nagelkerke R2 value change scores were used to determine significance. To identify which individual variables depression, anxiety, and low body appreciation were significantly associated with suicidal ideation, past suicidal attempts, and future suicidal risks, logistic regressions were applied. For logistic regression, SBQ-R items 1, 3, and 4 were recoded as binary outcomes: responses were coded as 0 = “never” and 1 = any other response indicating presence of ideation, attempt, or risk.
Results
The participants (n = 135) were recruited into the survey primarily through online and telephonic (n = 51) and physical platforms (n = 84). The results of this study suggest that mental health issues, such as depression, anxiety, and low body appreciation, have a significant impact on suicidal thoughts, attempts, and risk for the future. In particular, the participants’ mental stability was significantly impacted by anxiety, which contributed to persistent distress. The severity of suicidal ideation was significantly increased when depression was linked to an increase in feelings of hopelessness. Additionally, lower body appreciation scores were associated with elevated levels of self-doubt as well as a significant increase in the frequency and likelihood of suicidal thoughts and actions.
The study used four psychological scales, which are mentioned in Table 1, showing a summary of the scales, their measurements, and reliability. The CES-D scale produced an average score of 42.6 ± 16.5, indicating different degrees of depressive symptoms among the individuals. In the same direction, the mean score on the GAD-7 scale was 15.6 ± 4.6, suggesting a significant manifestation of anxiety. The BAS-2 data indicated an average score of 37.2 ± 10.5, which signifies the considerable diversity of viewpoints regarding body image. Furthermore, an average score of 11.3 ± 4.7 on the SBQ-R was obtained, suggesting that the participants exhibited suicidal tendencies and were exposed to associated risks. With Cronbach’s alpha values ranging from 0.80 to 0.88, the measures utilized in this research exhibited good to excellent internal consistency.
Descriptive of CES-D, GAD-7, BAS-2, and SBQ-R Scale
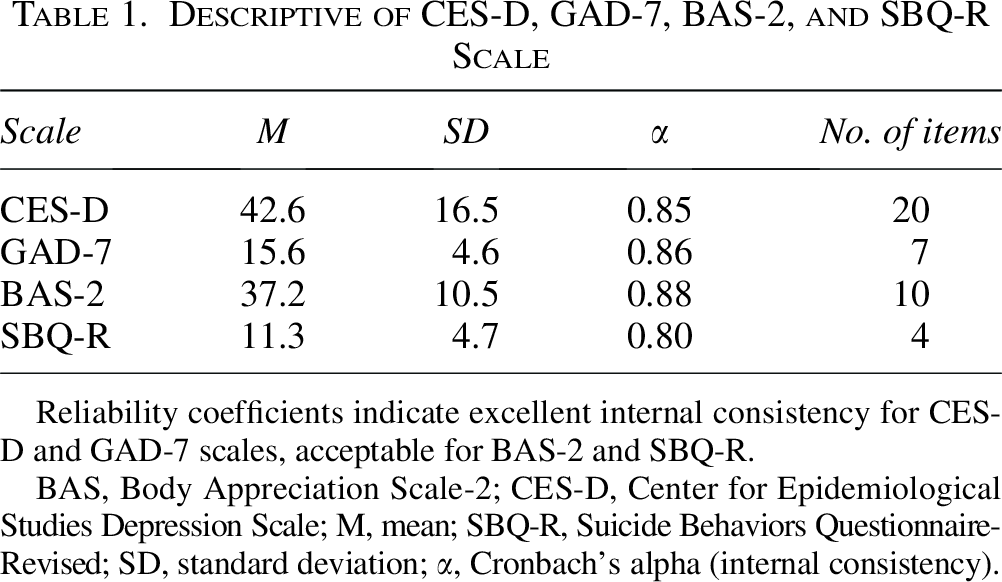
Reliability coefficients indicate excellent internal consistency for CES-D and GAD-7 scales, acceptable for BAS-2 and SBQ-R.
BAS, Body Appreciation Scale-2; CES-D, Center for Epidemiological Studies Depression Scale; M, mean; SBQ-R, Suicide Behaviors Questionnaire-Revised; SD, standard deviation; α, Cronbach’s alpha (internal consistency).
An analysis of suicidal ideation, suicide attempts, and suicidal risks in relation to diverse demographic factors within the transgender community is presented in Table 2. Each row represents several demographic categories, including information on the number of participants (n) and their proportion (%) within each category, as well as the average scores for suicidal ideation (SBQR-1), attempts (SBQR-3), and risks (SBQR-4). In addition, the table presents the mean, mean differences, and statistical significance (p ≤ 0.05) among different demographic groups.
Analysis of Suicidal Ideation, Attempts, and Risks Across Demographic Variables
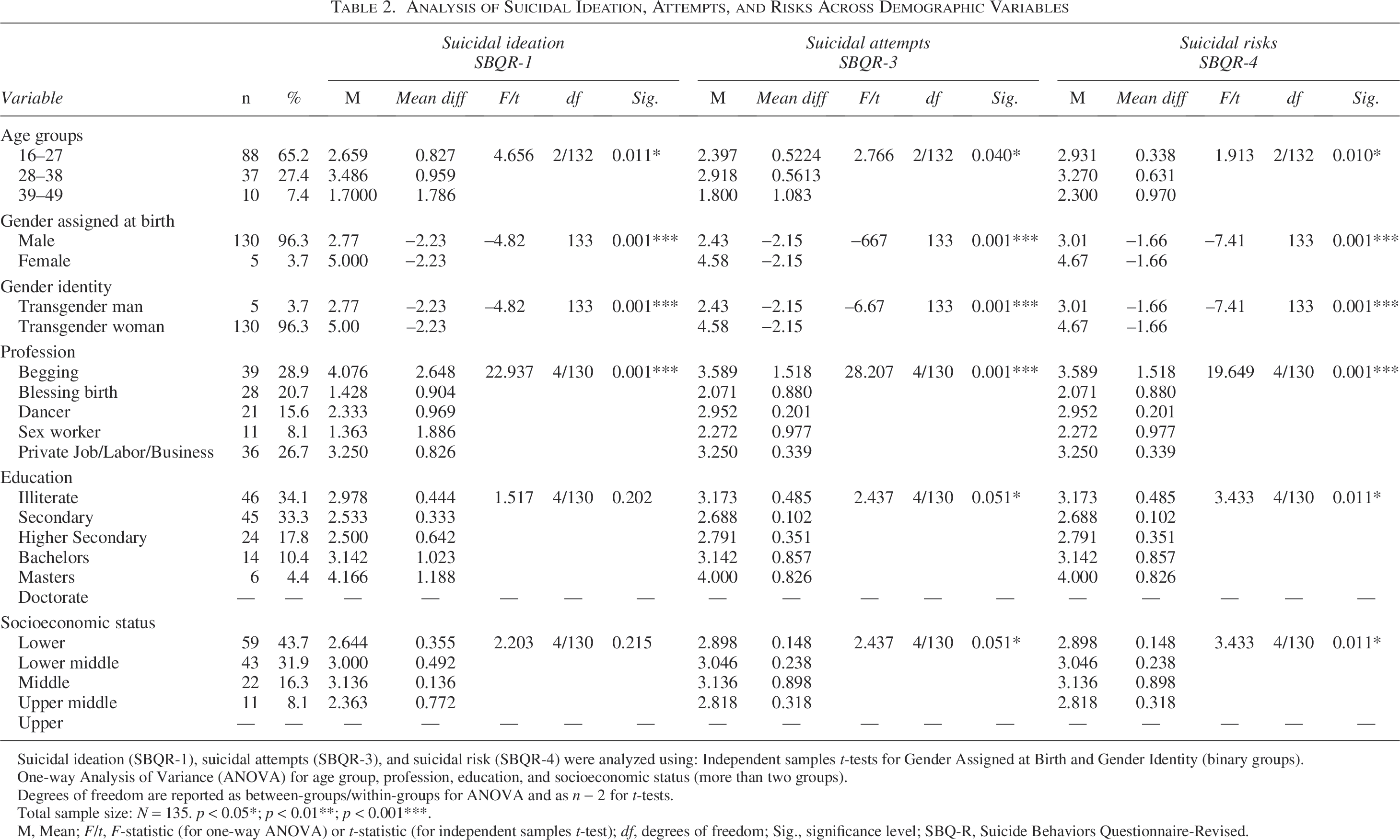
Suicidal ideation (SBQR-1), suicidal attempts (SBQR-3), and suicidal risk (SBQR-4) were analyzed using: Independent samples t-tests for Gender Assigned at Birth and Gender Identity (binary groups).
One-way Analysis of Variance (ANOVA) for age group, profession, education, and socioeconomic status (more than two groups).
Degrees of freedom are reported as between-groups/within-groups for ANOVA and as n − 2 for t-tests.
Total sample size: N = 135. p < 0.05*; p < 0.01**; p < 0.001***.
M, Mean; F/t, F-statistic (for one-way ANOVA) or t-statistic (for independent samples t-test); df, degrees of freedom; Sig., significance level; SBQ-R, Suicide Behaviors Questionnaire-Revised.
The mean scores for suicidal behaviors vary significantly between age groups, specifically within the categories of 17–27, 28–38, and 39–49. Younger individuals typically display lower average scores in comparison to older groups, suggesting variable levels of suicidal inclinations during various phases of maturity (p = 0.011, p = 0.040, p = 0.010 for ideation, attempts, and risks respectively).
The gender differences, based on an individual’s assigned birth category of Male or Female and self-identified as a Transgender man or Transgender woman, demonstrate important differences about suicidal ideation, attempted suicide, and the risks involved. These findings highlight the differences that are influenced by both a person’s gender identification and the gender they were assigned at birth ( p = 0.001 across all comparisons).
Occupational characteristics significantly influence suicide behaviors, as professions such as begging and sex work have higher average scores compared with occupations such as Dancer or Private Job/Labor/Business (p = 0.001). These variations indicate the possible effects of work on mental health outcomes associated with suicide.
There are also significant variations in suicidal behavior measures among individuals with different educational levels, ranging from illiterate to those with a master’s degree. There is a negative correlation between higher levels of education and the average scores for suicidal thoughts, suicide attempts, and suicide risks. This indicates that education has a protective impact on suicidal tendencies. For instance, the suicidal risk difference across education levels was significant (p = 0.011), with marginal significance for suicide attempts (p = 0.051).
Furthermore, different levels of suicide behaviors can be observed among socioeconomic status categories, showing a positive correlation between having a lower socioeconomic status and higher average scores for suicidal thoughts, attempts, and risks. These findings suggest that economic variables may play a role in increasing sensitivity to engaging in suicide behaviors. Again, the statistical significance for suicidal risk was observed at p = 0.011.
The statistical tests, such as ANOVA and t-tests, validated the significance of mean disparities among demographic groups, highlighting the characteristics, such as age, gender, profession, education, and socioeconomic position that significantly influence suicidal behaviors among participants.
The age distribution is shown descriptively in Table 3, which displays a range of 17–45 years, with a mean age of 26.99 years and a standard deviation of 6.43.
Descriptive Statistics of the Age
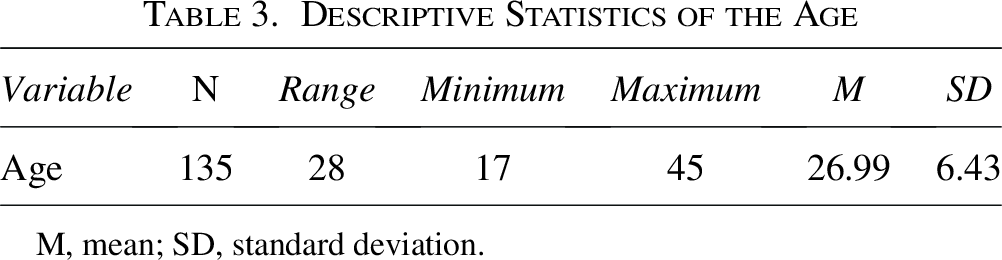
M, mean; SD, standard deviation.
Table 4 shows bivariate correlations between age, depression, anxiety, body shame, and suicide. Significant positive correlations were observed between depression and anxiety (r = 0.366, p < 0.01), depression and body shame (r = 0.344, p < 0.01), anxiety and body shame (r = 0.536, p < 0.01), anxiety and suicide (r = 0.362, p < 0.01), and body shame and suicide (r = 0.486, p < 0.01)—pointing out possible connections between these constructs. The results suggest that there is a proportional rise in the connected variable for every increase in one variable.
Bivariate Correlations Between Study Variables
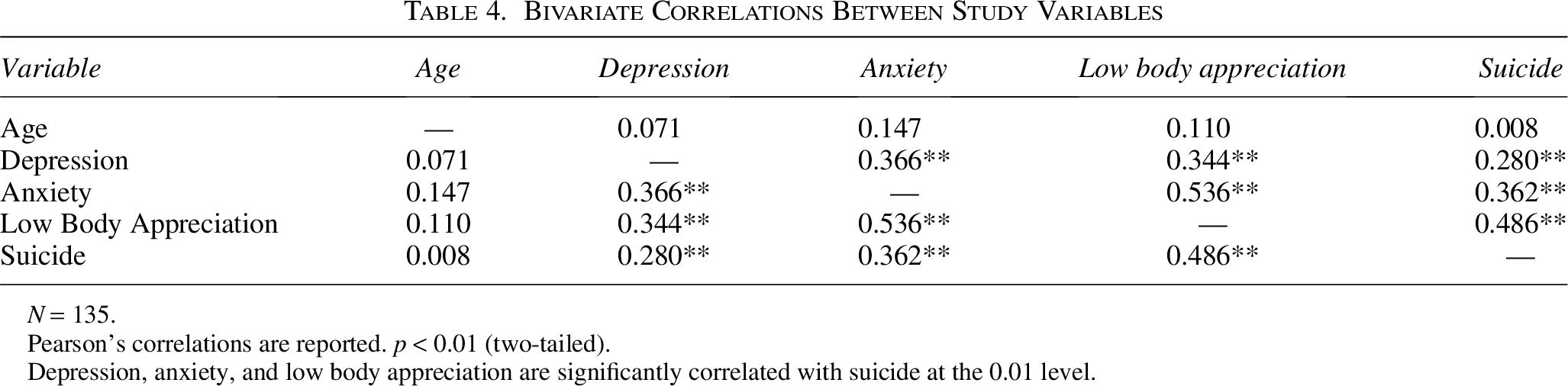
N = 135.
Pearson’s correlations are reported. p < 0.01 (two-tailed).
Depression, anxiety, and low body appreciation are significantly correlated with suicide at the 0.01 level.
Table 5 shows the relationship between depression, anxiety, body shame, and outcomes related to suicide: suicidal ideation (past), suicide attempts (past), and suicide risks (future). The reported regression coefficients (Nagelkerke R2 values) indicate the strength and direction of these relationships. Considerable R2 values (e.g., R2 = 0.395 for ideation, R2 = 0.376 for attempts, R2 = 0.415 for risks) suggest that the model including low body appreciation, depression, and anxiety may explain a considerable portion of the variation in previous and future suicide thoughts and attempts. The higher R2 values in the full model demonstrate how effectively the model explains variation. The Hosmer–Lemeshow tests confirmed good model fit for all three models (p > 0.05).
Suicide Ideation, Suicide Attempts, Suicide Risks, and Nagelkarke R2 Values
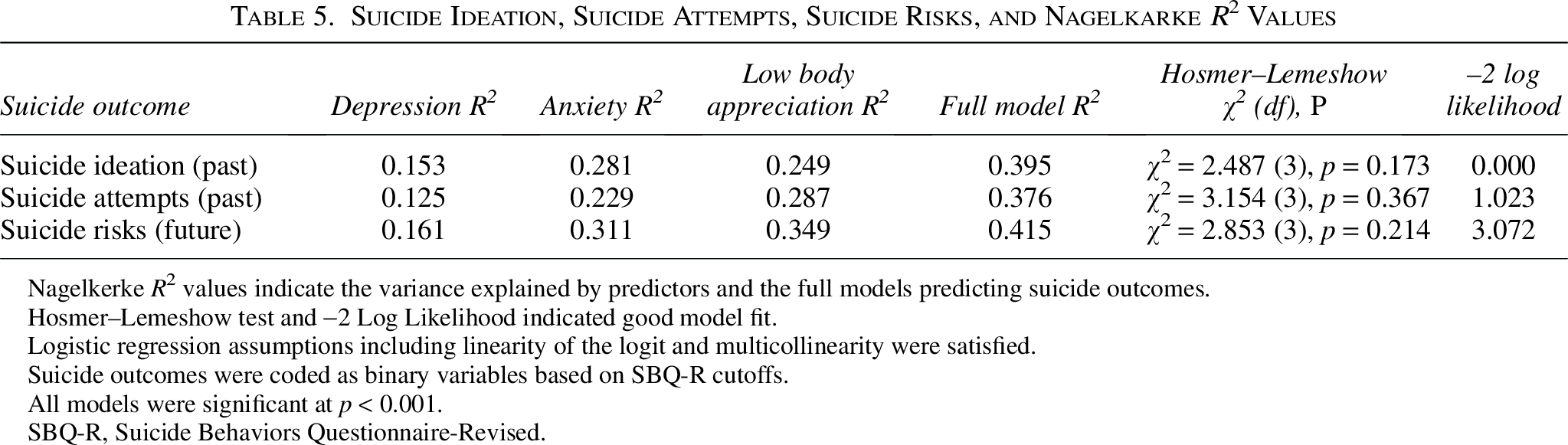
Nagelkerke R2 values indicate the variance explained by predictors and the full models predicting suicide outcomes.
Hosmer–Lemeshow test and −2 Log Likelihood indicated good model fit.
Logistic regression assumptions including linearity of the logit and multicollinearity were satisfied.
Suicide outcomes were coded as binary variables based on SBQ-R cutoffs.
All models were significant at p < 0.001.
SBQ-R, Suicide Behaviors Questionnaire-Revised.
In Table 6, the outcomes of suicide ideation, suicide attempts, and suicide risks are correlated with low body appreciation, anxiety, and depression. The findings show a strong correlation between low body appreciation and past suicidal thoughts (AOR = 1.071, p = 0.044) and future suicide risks (AOR = 1.013, p = 0.045). The results also show that anxiety has a significant inverse association with future suicide risks (AOR = 0.913, p = 0.039), while depression is significantly associated with previous suicide attempts (AOR = 1.024, p = 0.001) and future suicide risks (AOR = 1.017, p = 0.028).
Bivariate Logistic Regression Analysis Associating Suicide Ideation, Suicide Attempts, and Suicide Risks
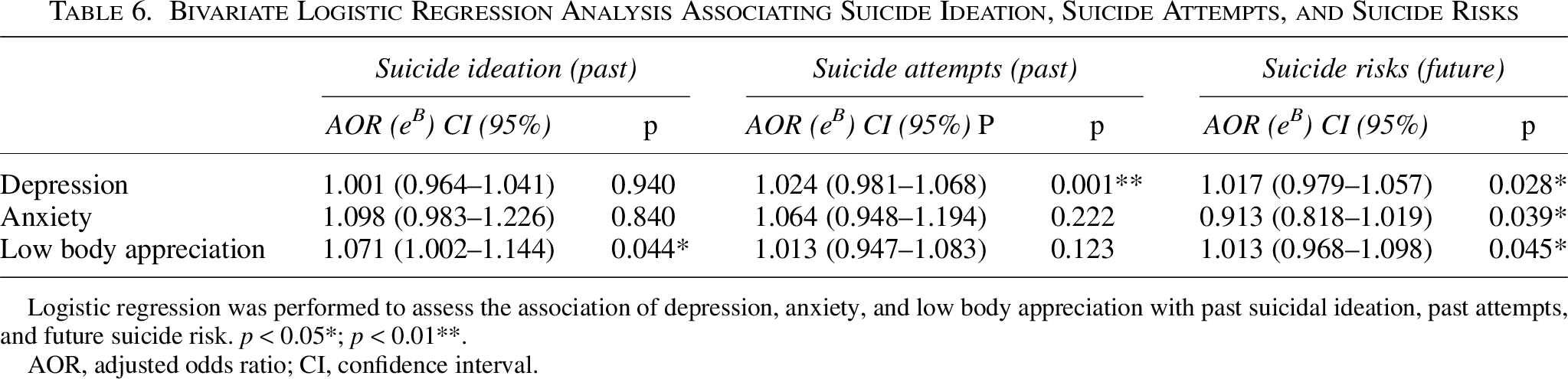
Logistic regression was performed to assess the association of depression, anxiety, and low body appreciation with past suicidal ideation, past attempts, and future suicide risk. p < 0.05*; p < 0.01**.
AOR, adjusted odds ratio; CI, confidence interval.
These results highlight the complex relationship between mental health characteristics and the likelihood of suicidal thoughts and actions, offering important new information for focused intervention and preventative approaches.
Discussion
The study represents the largest and most geographically diverse investigation of suicide-related outcomes among the transgender population of Pakistan. It is the first study in the region to examine associations between suicide and depression, anxiety, and low body appreciation. The findings indicate that suicidal ideation among transgender people is significantly associated with demographic factors such as age, gender assigned at birth, identified gender, profession, education, and socioeconomic status. The results suggest that suicidal behavior varies by age, with different patterns observed across age groups, possibly indicating that younger individuals experience different mental health concerns than older ones. Furthermore, gender differences were related to variations in suicidal thoughts and attempts, underscoring the need to consider the distinct experiences of transgender men and women. Occupational stability and higher education appeared to serve as protective factors, whereas lower socioeconomic status and involvement in stigmatized professions were associated with greater vulnerability.
Depression and anxiety were found to be prevalent among participants and were significantly associated with suicidal ideation and attempts. Low body appreciation also emerged as an important psychological factor, showing a relationship with higher self-doubt and increased suicidal behaviors. These findings suggest that transgender individuals may be more likely to experience mental distress and suicidal thoughts in the context of social rejection and negative body image.
These associations are supported by Thomas Joiner’s Interpersonal-Psychological Theory of Suicide, which explains that suicidal behavior tends to arise when three psychological conditions are present: thwarted belongingness, perceived burdensomeness, and acquired capability for suicide (Ploskonka, 2016). Transgender individuals in Pakistan often face severe social rejection and family exclusion, which may reflect a deep sense of thwarted belongingness. Additionally, the stigma, economic marginalization, and societal discrimination they encounter may contribute to feelings of burdensomeness. Repeated exposure to trauma, violence, and exclusion may desensitize individuals to pain and fear, which could play a role in the development of acquired capability for suicide (Jobbins, 2021). Together, these elements provide a relevant theoretical lens for understanding vulnerability to suicide-related outcomes among transgender people in Pakistan.
Moreover, the inverse association between anxiety and future suicide risk highlights a complex relationship between anxiety symptoms and suicidal impulses. The findings expand understanding of the psychosocial variables related to suicide within transgender communities, emphasizing the need for targeted interventions that address low body appreciation, along with depression and anxiety. Previous research has shown that factors such as age, identified gender, education, profession, and socioeconomic status are related to mental health outcomes that may contribute to suicide risk. A study by Mustanski et al. (2010) found that among Lesbians, Gay, Bisexual and Transgender (LGBT) youth aged 16–20, one-third met the criteria for any mental disorder, with few statistically significant racial/ethnic and gender differences (Mustanski et al., 2010). In the current study, participants engaged in professions such as begging and sex work reported higher average scores related to suicide than those working in dancing, private jobs, labor, or business.
This study also found that higher levels of education were negatively associated with suicidal thoughts, suicide attempts, and suicide risk. This supports the role of education as a possible protective factor. Most participants belonged to lower socioeconomic groups, and no individuals were from upper-income backgrounds, indicating socioeconomic disparities within the sample. A case study by Shahzad et al. (2020) also reported that transgender individuals may be at increased risk of suicide due to the influence of demographic stressors (Shahzad et al., 2020). Similarly, Toomey et al. (2018) found high suicide rates among female-to-male and nonbinary transgender persons, emphasizing the importance of recognizing distinct vulnerabilities within the gender minority population (Toomey et al., 2018). A study from China by Chen et al. (2020) reported alarming rates of abuse, mental illness, stigma, and suicide-related deaths among transgender women (Chen et al., 2020).
The study also sheds light on the relationship between gender identity and mental health among transgender individuals. Trujillo et al. (2017) emphasized how prejudice may influence both psychological distress and suicide risk and underscored the value of social support in mitigating such outcomes among marginalized groups (Trujillo et al., 2017). The demographic analysis in the current study similarly highlights the need for targeted and culturally appropriate mental health services.
The literature review by Pinna et al. (2022) and the current findings both reflect a high prevalence of depression in transgender populations. This supports the call for more inclusive and accessible mental healthcare in Pakistan (Pinna et al., 2022). The associations between depression, anxiety, and suicide risk in the current study are consistent with those reported by Budge et al. (2013) and Bouman et al. (2017). Likewise, Virupaksha et al. (2016) outlined that mental health issues, along with gender-based discrimination, bullying, and exclusion, are major factors related to suicidal behaviors (Bouman et al., 2017; Budge et al., 2013; Virupaksha et al., 2016). Rao Azeem et al. (2019), in a study of 156 transgender individuals, reported a high prevalence of suicidal ideation (42.9%) and found significant associations with depression and drug use, further emphasizing the importance of early screening and intervention to reduce suicidal vulnerability (Rao Azeem et al., 2019).
This study also clarified the complex interrelations among depression, anxiety, and low body appreciation, and how each of these is associated with suicidal ideation, attempts, and perceived risk in the transgender population. The findings reflect the multifaceted nature of mental health struggles in this group, indicating the need for integrated treatment approaches. The use of standardized psychological assessment tools allowed for reliable evaluation of mental health indicators, contributing to a comprehensive understanding of the challenges faced by transgender individuals in Pakistan’s sociocultural environment. This multidimensional perspective helps contextualize the link between mental health and societal attitudes, particularly in regard to body image.
However, the sample may not fully reflect the diverse regional and cultural contexts of the transgender community across Pakistan. A study by (Wolford-Clevenger et al., 2017) also highlighted the risks of suicide in transgender populations and pointed to the lack of sufficient empirical data and theoretical models in this area. Although the literature remains limited, the rates of suicide ideation and attempts reported here align with previous findings and reinforce the urgency of further research into mental health among gender minorities.
Despite these limitations, the study provides a culturally grounded analysis of the psychosocial factors influencing mental health and suicide risk among transgender individuals. These insights may guide the development of prevention strategies and mental health services that are sensitive to the needs of this group. Closing the healthcare gap and designing context-specific interventions is essential to promoting mental well-being in Pakistan’s transgender population.
This study explains the mental health challenges experienced by transgender individuals in Pakistan, but it has several limitations. The use of online data collection methods and interviews may introduce some response bias, as participants might be hesitant to fully disclose sensitive issues related to suicide. Furthermore, the study restricted the sample to a specific group, and potential cultural and regional disparities within Pakistan could impact the generalizability of findings. Additionally, the cross-sectional nature of the study limits the ability to assess causality and accurately predict future suicide risk, as self-reported intentions may not translate into actual future behavior. It is suggested that future studies should address these limitations through meta-analyses, longitudinal study designs, more inclusive sampling, and incorporating both qualitative and quantitative approaches to provide a more comprehensive understanding of the mental health challenges faced by transgender individuals in Pakistan.
Conclusions
In conclusion, this research explains the mental health issues and the likelihood of suicide among transgender individuals in Pakistan. The correlations found that depression, anxiety, and low body appreciation are associated with suicide-related outcomes. The bivariate correlations revealed that low body appreciation is strongly correlated with suicidal risks. The regression analysis shows that depression, anxiety, and low body appreciation were significantly associated with suicidal behaviors. Depression was strongly associated with suicide attempts and risks, while anxiety and low body appreciation were related to ideation and risks.
Demographic variables such as age, gender identity, education level, and socioeconomic status all had an impact on vulnerability. While younger individuals showed higher suicidal ideation in group comparisons, lower education and low socioeconomic status were consistently associated with greater suicide risk. Additionally, professions such as begging and sex work were linked to elevated suicidal behaviors, likely due to social exclusion, stigma, and economic hardship.
These findings underscore the need for targeted mental health interventions, especially those addressing body image concerns and stigma. Enhancing access to psychological services, promoting mental health literacy, and creating inclusive educational and economic opportunities are crucial to reducing suicide vulnerability among gender minorities in Pakistan.
Authors’ Contributions
A.J. did the conceptualization and design of the article and original draft writing. D.D. provided supervision and validation. W.M.D. provided resources, software, and formal data analysis. A.H. conducted surveys and translated interviews. T.A.F. helped graphical representations and software. A.J. reviewed, edited, and prepared the article for submission.
Footnotes
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
The authors declare that they received no funding for this study.
Data Availability
The datasets generated during the current study are available from the corresponding author on reasonable request.