
Abstract
The neurological symptoms of pediatric mild encephalopathy/encephalitis with a reversible splenial lesion (MERS) are mild and have a good prognosis. However, some aspects of neonatal MERS are unclear due to a lack of clinical knowledge. We present a neonatal case of MERS with features of poor activity and prolonged poor oxygenation after birth without asphyxia. He was diagnosed with MERS by brain magnetic resonance imaging (MRI) on day10, because the diffusion restriction of the splenium of the corpus callosum (SCC) seen on diffusion-weighted MRI on day 5 was attenuating. He was discharged due to good progress on day 26, but growth issues and developmental delay were observed in the follow up from 1-10 months. In rare neonatal cases, many aspects of the clinical course and prognosis are thus unclear. MERS should be considered in newborns who show unexplained non-neural or other encephalopathic symptoms.
Introduction
Mild encephalopathy/encephalitis with a reversible splenial lesion (MERS) is the second-most common childhood acute encephalopathy (16%) in Japan, after acute encephalopathy with biphasic seizures and late reduced diffusion (29%). 1 The rate does not differ markedly by gender, and the average age of onset is 5.6 years, making it common in adolescents. 1 The onset factors are often viral infection, including influenza virus (34%), rota virus (12%), mumps virus (4%), and bacterial infectious diseases (3%). 1 Although five newborn cases have been reported in China and a similar case considered to be MERS in Japan,2,3 no other reports of newborn cases are available. The findings and pathology of this clinical imaging syndrome thus seem relatively rare, or perhaps cases cannot be diagnosed during the neonatal period. While the neurological symptoms of pediatric MERS are mild and have good prognosis,4,5 clinical knowledge of neonatal MERS is lacking.
Case Presentation
A 10-day-old boy was born by normal vaginal delivery at 40 weeks’ gestation at 3056 g. His Apgar score was 8 points (5 min), and umbilical cord blood gas showed a pH of 7.299. Just before the delivery phase, fetal tachycardia and a low-grade fever were observed.
With a diagnosis of transient tachypnea, since oxygen saturation was 80% range on room air, oxygen administration (FiO2: 28%) was started in an incubator. Blood tests showed elevated creatinine kinase (CK 4825 IU/L) and hepatobiliary enzymes (AST 158 IU/L, ALT 71 IU/L, ɤ-GTP 190 IU/L) and mixed respiratory-metabolic acidosis. His oxygen demand had deteriorated by 16 h after birth, so blood tests, a blood gas test, head ultrasonography, and chest x-ray were performed, revealing no abnormalities.
His little interest in feeding, poor activity continued at DOL (day of life) 5, so brain magnetic resonance imaging (MRI) was performed. Diffusion-weighted imaging (DWI) showed a decrease in diffusivity in the splenium of the corpus callosum (SCC) and the white matter around the dorsal horn of the lateral ventricle and a slight decrease in the bilateral frontal lobes, suggesting hypoxic ischemic encephalopathy (HIE) (Figure 1, panel A). A routine electroencephalogram (EEG) at DOL 8 showed no obvious abnormal waves except for an overall small amplitude.
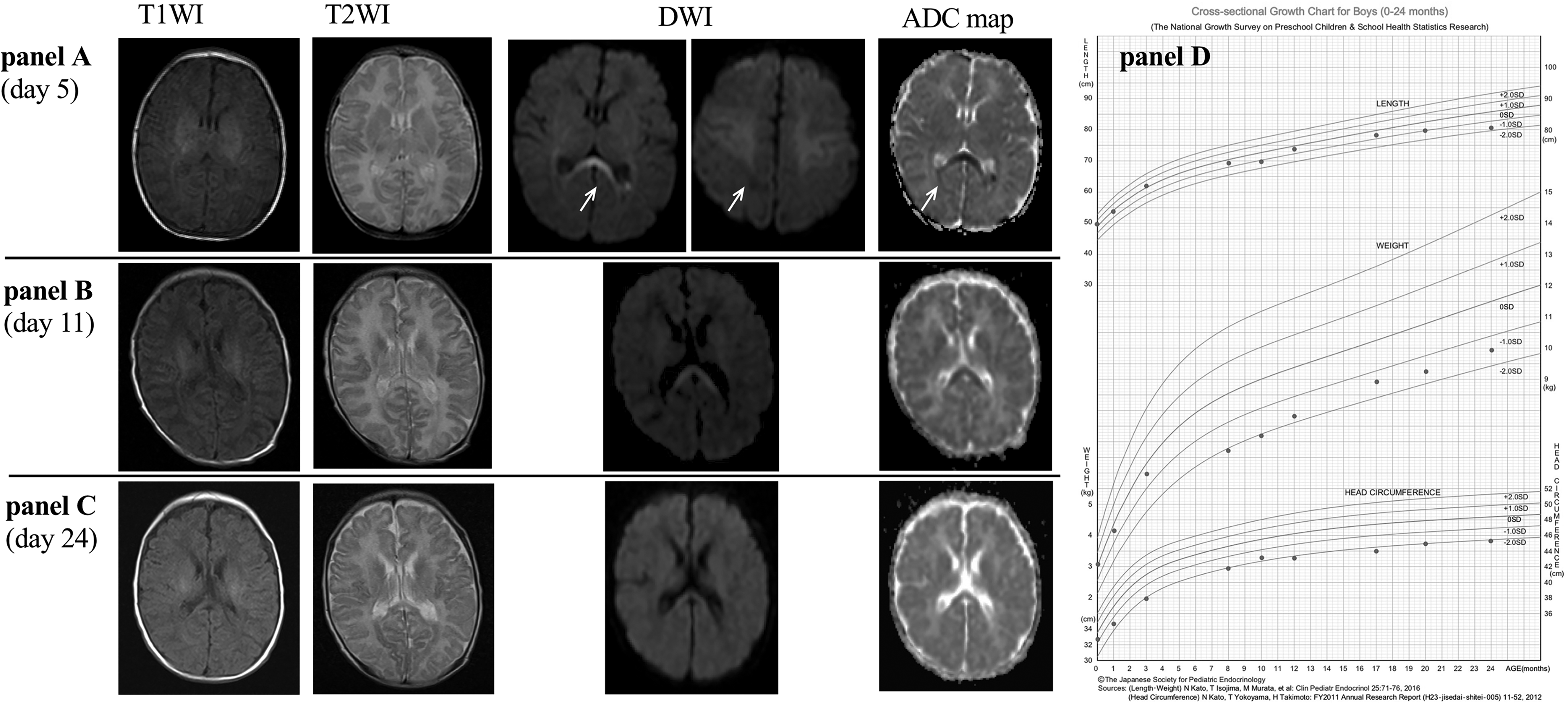
Sequential changes in the brain MRI findings from 5 days old (panel A) to 11 days old (panel B). The white matter around the lateral ventricle and the lesion in the splenium of the corpus callosum (SCC) showed hyper-intensity on T2WI and DWI and hypo-intensity on an ADC map (white arrow). The diffusion restriction of the SCC had disappeared by 24 days old (panel C). A comparison of the age- and sex-specific height and weight growth charts with mean, ± 1SD, and ± 2SD lines (z-score lines) for male Japanese children (Panel D).
Since his oxygen demand still was not improving, he was transferred to our neonatal intensive-care unit at DOL 10. Based on brain MRI at DOL 11, he was diagnosed with neonatal MERS, as the restricted diffusion at the SCC was slightly obscured (Figure 1, panel B). His oxygen demand improved until DOL 19, and he was discharged at DOL 26 because his activity and his blood test data improved. The brain MRI at DOL 24 showed that the diffusion restriction of the retro-splenial cortex had disappeared (Figure 1, panel C). We found that the serum IgM levels of Toxoplasma, Varicella-zoster virus, Rubella virus, Herpes simplex virus were negative, and comprehensive PCR virus study including Adeno viruses, Corona viruses, Parainfluenza virus, Boca viruses, Rhino viruses, Respiratory Syncytial Virus, Influenza A and B viruses, Human metapneumo virus, Entero viruses (by using Pharyngeal swab), Cytomegalo virus (by using urine) were negative. Newborn mass screening tests for metabolic disorders were normal.
In the observation of his development, head control and rolling over were observed at 4 months age, but by 10 months age, he was still unable to sit up alone. From around 6 months age, poor weight gain of approximately −2.0 standard deviations was observed (Figure 1, Panel D). No obvious abnormal findings were found on head MRI at one year old.
At one and a half years old, he was able to sit alone and stand up, and at two years old, he was able to walk but still could not speak words.
Discussion
We encountered a neonate who developed MERS after birth with symptoms of poor oxygenation and poor activity.
To our knowledge, this is the seventh case, preceded by reports of five newborn cases from China 2 and a similar case considered to be MERS in Japan, 3 so we speculate that neonatal MERS is relatively rare or unrecognized in clinical settings.
MERS is a clinical imaging syndrome based on MRI findings of the brain, especially DWI. Imaging changes are transient and disappear within 2 months (72% within 1 week). 4 A typical case with lesions only in the SCC is called MERS type 1, and cases with lesions in the symmetric white matter in addition to the SCC are categorized as MERS type 2.3,4,6 The characteristics of the imaging findings in newborns were similar to those in older children. 6 Case 1 was MERS type 2 and case 2-6 were MERS type 1 (Table 1). In the present case, a decrease in diffusivity in the SCC and white matter was noted initially, so the previous doctor provisionally diagnosed the patient with HIE. But a follow-up study revealed an isolated SCC lesion with no reduced diffusion in the white matter, so our case was considered to indicate MERS type 2.
Summary of clinical findings in the six previously reported cases and our own case.

Abbreviations: GW, gestational age; CSF, cerebrospinal fluid; EEG, electro-encephalogram; NA, not available; ND, not done.
Four of the five cases in China 2 were born without asphyxia, and our case also had no neonatal asphyxia. In case 1 with asphyxia, the onset of MERS was at DOL 2, and involuntary spasms of the lower limb muscles were observed, but the patient was discharged without any neurological abnormalities. In the previous Japanese case, 3 DWI of a neonate with mild asphyxia at DOL 12 revealed a high-signal-intensity lesions in the central portion of the SCC with a decreased ADC value. The condition gradually improved, and the patient was discharged at DOL 18 and MRI findings at six months old were normal. The relationship between neonatal asphyxia and the onset of MERS is considered unclear at present.
A study of 54 pediatric MERS cases revealed a fever (94%), vomiting (24%), and diarrhea (15%) as prior symptoms and abnormal behavior (54%), convulsions (33%), impaired consciousness (30%), headache (24%), and meningism (6%) as neurological symptoms. 4 Among the five newborns in China, 2 there were three cases of convulsions, and instances of poor activity, poor feeding, and moaning were also observed. In our case, no convulsions or obvious EEG abnormalities were noted, but indefinite complaints including poor feeding and poor activity with unexplained oxygen demand may be important indicators of neonatal MERS.
Viral and bacterial infectious diseases have been reported as pathogens of MERS. 1 In the five cases from China, TORCH-IgM and culture tests were negative, except for in case 5 (details unclear). In our case, all comprehensive examinations for viruses were negative. On the other hands, blood test findings of MERS in children show hyponatremia (Na 131.8 ± 4.1 mEq/L) more frequently than in other cases of encephalopathy. 7 However, no obvious serum sodium abnormality was observed in our case. Multiple factors, including hyponatremic encephalopathy, are thus thought to be involved in the development of neonatal MERS.
The growth and developmental delays seen in our case can occur in patients diagnosed with MERS during the infantile period.8 In addition, in the previous Japanese neonate case, at 1 year old, he had mild hypotonia without paralysis, mild psychomotor retardation, and no epileptic seizures. 3 The further accumulation of cases may reveal that the prognosis of MERS with a neonatal onset is not always good.
Conclusion
The prognosis of neonatal-onset MERS may not always be good. However, many cases may not be able to be diagnosed during the neonatal period. In newborns lacking activity or with unexplained oxygen demand, we should consider MERS as a differential diagnosis.
Footnotes
Acknowledgments
We thank the faculty and staff of the Maternal and Child Care Hospital of the University of Ryukyus and all participants in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series. Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.