
Abstract

KEY POINTS
In a longitudinal cohort of 71 patients treated with teprotumumab, 52.1% experienced clinically significant worsening of glycemic control, a notable contrast to the lower incidence rates reported in initial clinical trials.
The temporal onset and severity of dysglycemia were heavily stratified by baseline metabolic status. Patients with diabetes showed a peak at a median of 4.8 months, whereas normoglycemic individuals exhibited a delayed metabolic drift peaking at 13.2 months.
The chronicity of this metabolic disruption requires attention, as only 33.3% of the diabetes cohort and 35.3% of the normoglycemic cohort who experienced glycemic worsening spontaneously recovered to their baseline metabolic status.
SUMMARY
Background
Thyroid eye disease (TED) is an autoimmune condition driven by the activation of orbital fibroblasts via a receptor complex involving the thyrotropin receptor and insulin-like growth factor 1 receptor (IGF-1R). 1 The use of teprotumumab, a monoclonal IGF-1R inhibitor, transitioned TED management from broad immunosuppression to targeted therapy.2,3 However, because IGF-1R is ubiquitously expressed, systemic inhibition disrupts physiological endocrine feedback loops. 4 Specifically, the blockade of IGF-1R reduces the feedback inhibition of growth hormone (GH) secretion, leading to elevated GH levels that promote glucose production and peripheral insulin resistance. Furthermore, teprotumumab impairs insulin receptor (IR) signaling by binding to IGF-1R/IR hybrid receptors. This inhibits downstream IR activation and triggers internalization and degradation of the entire hybrid complex, thereby removing functional insulin receptors from the cell surface and compounding the insulin resistance. Although early clinical trials reported treatment-emergent hyperglycemia in roughly 10% of participants, 5 subsequent real-world observations demonstrated a higher incidence, 6 particularly among patients with preexisting glucose intolerance. Results from prior reports were often restricted by brief follow-up periods, leaving it unclear whether these metabolic disruptions resolve after therapy cessation. The study by Ha et al. addresses this clinical gap by evaluating an extended longitudinal cohort to quantify the severity, trajectory, and durability of teprotumumab-induced dysglycemia. 7
Methods
This retrospective, single-institution study was conducted at the Massachusetts Eye and Ear Infirmary, capturing clinical data from January 1, 2020, to March 31, 2025. Inclusion required adult patients initiating teprotumumab for TED to have documented hemoglobin A1c (HbA1c) measurements both prior to and after starting treatment. To isolate the effects of IGF-1R inhibition, individuals with oral or intravenous corticosteroid use within 3 months prior to or during therapy were strictly excluded.
Baseline metabolic stratification used American Diabetes Association (ADA) diagnostic criteria: normoglycemia (HbA1c, ≤5.6%), prediabetes (HbA1c, 5.7%–6.4%), and diabetes (HbA1c, ≥6.5% or prior clinical diagnosis). The primary outcomes assessed absolute quantitative shifts in HbA1c from baseline to peak and immediate posttreatment values. Additionally, the investigators evaluated the incidence of clinically significant worsening glycemic control, defined as formal progression to a higher ADA category or an absolute intracategory HbA1c increase of ≥0.5%, a threshold aligned with elevated risk of microvascular complications. Recovery was strictly defined as a return to baseline metabolic status without the requirement for supplementary glucose-lowering pharmacotherapy beyond the pretreatment regimen. Data were analyzed using nonparametric statistical methods.
Results
The final cohort comprised 71 patients (median age, 58 years; 71.8% female) with a median follow-up of 28.0 months. Baseline stratification identified normoglycemia in 57.7%, prediabetes in 28.2%, and diabetes in 14.1%. Overall, 92% of patients completed the eight-infusion protocol, with three discontinuing prematurely due to severe hyperglycemia.
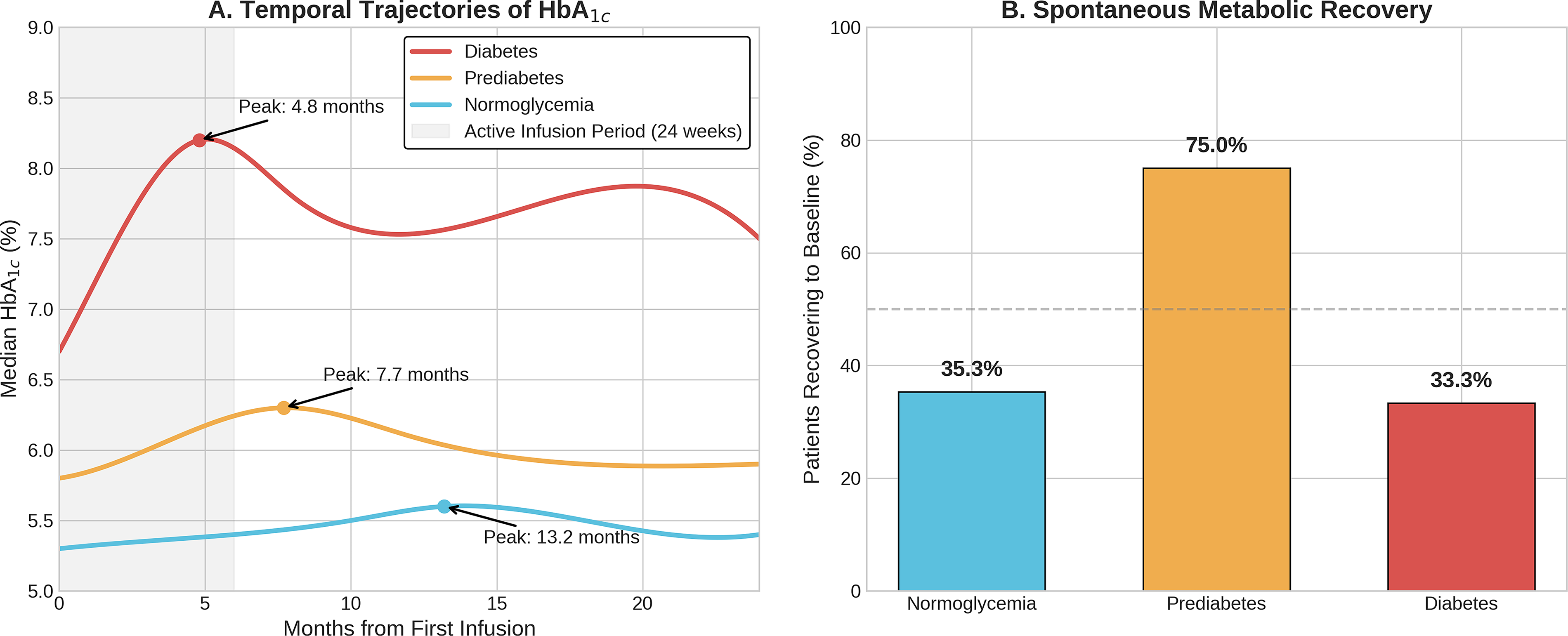
Teprotumumab initiation was associated with a statistically significant overall elevation in median HbA1c (from 5.5% to 5.9%, p<0.001), but the magnitude and timing were highly stratified by baseline metabolic risk. Patients with baseline diabetes endured the most dramatic decompensation, experiencing a median HbA1c increase of 1.4%, peaking rapidly at 4.8 months (Figure 1A). Prediabetic patients experienced a 0.5% increase, peaking at 7.7 months. Conversely, normoglycemic individuals exhibited an insidious trajectory, with a median 0.3% increase, peaking at 13.2 months, typically after treatment completion. Subgroup analysis revealed these HbA1c elevations occurred uniformly across normal, overweight, and obese body-mass index categories.
The Impact of Teprotumumab on Glycemic Management.
Clinically significant worsening of glycemic control was seen in 90.0% of patients with diabetes, 50.0% of patients with prediabetes, and 44.0% of normoglycemic patients. Consequently, initiation or escalation of glucose-lowering pharmacotherapy was required by 60.0%, 30.0%, and 2.4% of individuals in these groups, respectively. Regarding long-term recovery, spontaneous return to baseline metabolic status without sustained, escalated pharmacotherapy occurred in only 33.3% of patients with preexisting diabetes and 35.3% of normoglycemic patients, whereas patients in the prediabetes cohort demonstrated greater resilience (75.0% recovery) (Figure 1B).
Conclusions
Teprotumumab frequently induces persistent glycemic deterioration, strongly modulated by baseline metabolic reserve. The rapid decompensation in patients with diabetes at baseline and delayed onset in normoglycemic individuals highlight the importance of systematic risk assessment and extended posttreatment surveillance to prevent permanent metabolic complications.
COMMENTARY
Teprotumumab is now a well-established medical therapy for moderate-to-severe thyroid eye disease (TED). 2 Although its efficacy in reducing proptosis and overall disease activity is well documented, integrating this biologic into routine clinical practice has brought into sharper focus its systemic side effects, most notably hyperglycemia, hearing impairment, and the potential exacerbation of inflammatory bowel disease. 3 From a stewardship perspective, the longitudinal investigation by Ha et al. characterizes this metabolic dysregulation in the largest reported cohort so far with the longest duration of follow-up, and thus provides practical data on how to monitor the risks of insulin-like growth factor 1 receptor (IGF-1R) inhibition over time.
The 52.1% incidence of clinically significant dysglycemia is notably higher than the roughly 10% seen in initial clinical trials, 5 likely reflecting the inclusion of metabolically fragile patients. However, significant surveillance bias exists. Of 198 patients initiating teprotumumab, only 71 met inclusion criteria with paired HbA1c measurements. This suggests that we may be underestimating dysglycemia in unmonitored “low-risk” individuals, while simultaneously missing the true upper limit of metabolic toxicity due to the likely exclusion of patients with severely uncontrolled baseline diabetes.
Despite these missing variables, the data suggest that in everyday practice, the metabolic impact of IGF-1R inhibition is frequent and often chronic. For patients with baseline diabetes, the rapid glycemic decompensation (peaking at a median of 4.8 months) indicates sustained beta-cell exhaustion rather than a brief, transient spike. A particularly important finding is the delayed glycemic trajectory in normoglycemic individuals. In this group, HbA1c peaked at a median of 13.2 months, well after the standard 24-week infusion cycle concluded. This observation indicates that ending metabolic surveillance immediately after the last infusion is premature and risks missing late-onset dysglycemia. Additionally, the authors noted that these HbA1c elevations occurred uniformly across normal, overweight, and obese body-mass index categories, suggesting that this metabolic disruption may be a direct pharmacodynamic consequence of the drug rather than simply an exacerbation of baseline adiposity-driven resistance.
Furthermore, although HbA1c serves as a practical surrogate for glycemic control, questions remain regarding whether these metabolic excursions confer a lasting vascular penalty or what compounded risks exist for patients requiring repeated courses of teprotumumab. To mitigate these uncertainties in current practice, we must implement structured metabolic stewardship. A safe protocol begins with universal baseline screening using HbA1c and fasting blood glucose, deferring therapy in diabetic patients with poor glycemic control (baseline HbA1c, >8%) until improved control is achieved. 4 During treatment, close surveillance using routine capillary glucose testing or targeted continuous glucose monitoring is essential to manage acute excursions. Crucially, completing the 24-week infusion cycle must not mark the end of metabolic oversight; ongoing routine monitoring is required well into the posttreatment phase to capture the delayed drift observed in this cohort. Ultimately, navigating this targeted therapy requires a coordinated, long-term multidisciplinary approach in which endocrinologists and ophthalmologists manage TED collaboratively, safely preserving orbital health without precipitating permanent metabolic complications.