
Abstract
KEY POINTS
Both conventional smear (CS) and liquid-based preparation (LBP) methods demonstrate excellent diagnostic performance in thyroid fine-needle aspiration cytology, with LBP showing modestly higher sensitivity and overall diagnostic accuracy.
CS retains important practical advantages, particularly its compatibility with rapid on-site evaluation, which enhances specimen adequacy, improves procedural efficiency, and supports appropriate triage for ancillary testing and molecular studies.
LBP offers growing advantages in modern cytopathology workflows, including greater standardization, shorter screening time, improved support for ancillary techniques, and better integration with digital pathology and artificial intelligence platforms.
SUMMARY
Background
Fine-needle aspiration (FNA) cytology is the cornerstone of preoperative evaluation for thyroid nodules.1–3 It is also one of the most successful minimally invasive diagnostic techniques in pathology. The implementation of The Bethesda System for Reporting Thyroid Cytopathology (TBSRTC) has improved standardization in reporting, which has strengthened communication among cytopathologists, endocrinologists, surgeons, and radiologists. 2 It has also facilitated more consistent risk stratification and clinical management. 3
Despite these advances, the optimal preparation method for thyroid FNA specimens remains controversial. The two main preparation methods are conventional smear (CS) and liquid-based preparation (LBP). CS involves manually spreading aspirated material onto glass slides. This method has long been the dominant preparation method worldwide. CS preserves many native cytomorphologic features well and supports rapid on-site evaluation (ROSE); however, it can be affected by blood contamination, air-drying artifacts, and variability in smear quality. LBP for cytology was initially developed for gynecologic cytology and later adapted for nongynecologic specimens, including thyroid FNA. LBP offers cleaner backgrounds, more standardized slide preparation, and potentially improved workflow efficiency. However, some concerns remain regarding altered tissue architecture, loss of colloid, and reduced visibility of certain nuclear features.
Studies comparing CS and LBP have shown conflicting results. Many are limited by small sample size, single-center design, or differences in methodology. In practice, some institutions use the two methods together to improve diagnostic yield. However, the true benefit of this combined approach remains uncertain. 4 The study by Chen et al. aimed to address these unresolved questions using a very large multicenter cohort. 5
Methods
Chen et al. conducted a retrospective multicenter study across 16 medical centers in China between June 2010 and November 2025. 5 The investigators analyzed a total of 89,392 thyroid FNA specimens, making this the largest study to date comparing CS, LBP, and combined preparation methods in thyroid cytopathology. Of these, 49,309 were prepared using CS alone, 13,161 using LBP alone, and 26,922 using a combination of the two methods. Cytologic diagnoses were categorized according to the TBSRTC. 2 The authors compared rates of nondiagnostic specimens (Bethesda I) and indeterminate categories (Bethesda III and IV) between preparation methods. For cases with surgical follow-up, histopathology served as the reference standard to calculate sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and overall diagnostic accuracy.
A notable feature of the study is the analysis of a “multi-diagnoses” subgroup. This included cases with separate CS and LBP interpretations alongside a final integrated diagnosis. This design enabled direct, paired comparison between the two preparation methods within the same lesion. It provided a unique opportunity to assess concordance and relative diagnostic performance while minimizing variability between cases.
Results
Overall, LBP showed slightly superior overall diagnostic performance than CS, with higher sensitivity (98.1% vs. 95.0%), higher NPV (82.6% vs. 71.1%), and improved overall diagnostic accuracy (97.0% vs. 93.7%). PPV and specificity were similar between the two methods. The combined use of CS and LBP yielded the lowest nondiagnostic rate at 7.3%, compared with 10.5% for CS alone and 17.9% for LBP alone, suggesting a complementary effect on specimen adequacy. However, this combined approach was associated with a higher rate of indeterminate diagnoses and did not significantly improve overall diagnostic accuracy beyond LBP alone. Specificity was also slightly lower in the combined group, indicating that additional cytomorphologic information may sometimes increase interpretive ambiguity.
In the multi-diagnoses subgroup, concordance between CS and LBP was high at 92.9%, emphasizing that both methods are generally reliable when adequate material is available. In this paired-sample analysis, diagnostic performance between CS and LBP was much closer, with similar sensitivity, PPV, and accuracy. These findings suggest that differences observed in the broader cohort may be influenced more by specimen adequacy and preparation factors than by intrinsic limitations of either method.
Conclusions
The authors conclude that, although LBP offers marginally better diagnostic performance, the routine combined use of CS and LBP may not be justified. It increases cost without providing a meaningful gain in diagnostic accuracy over LBP alone. They advocate selecting a single preparation method based on institutional resources and local practice patterns.
COMMENTARY
The study by Chen et al. provides important contemporary evidence addressing a long-standing debate in thyroid cytopathology. One of the most significant observations is that both CS and LBP perform remarkably well overall. Although LBP demonstrated slightly superior sensitivity and overall diagnostic accuracy, the differences were relatively modest, and the very high concordance rate between paired CS and LBP specimens emphasizes that both techniques remain highly reliable when adequate material is obtained.
CS continues to offer several important practical advantages (Figure 1). Properly prepared smears preserve colloid, highlight cyst contents, maintain tissue fragment architecture (three-dimensional architecture, papillary fragments with fine vasculatures, and crowded follicular patterned groups). Many cytopathologists, including us, also find that diagnostic nuclear features of papillary thyroid carcinoma, particularly grooves and pseudo-inclusions, may be easier to appreciate on CS than on LBP slides, where architectural alteration, cellular fragmentation and loss of nuclear details can occasionally occur.
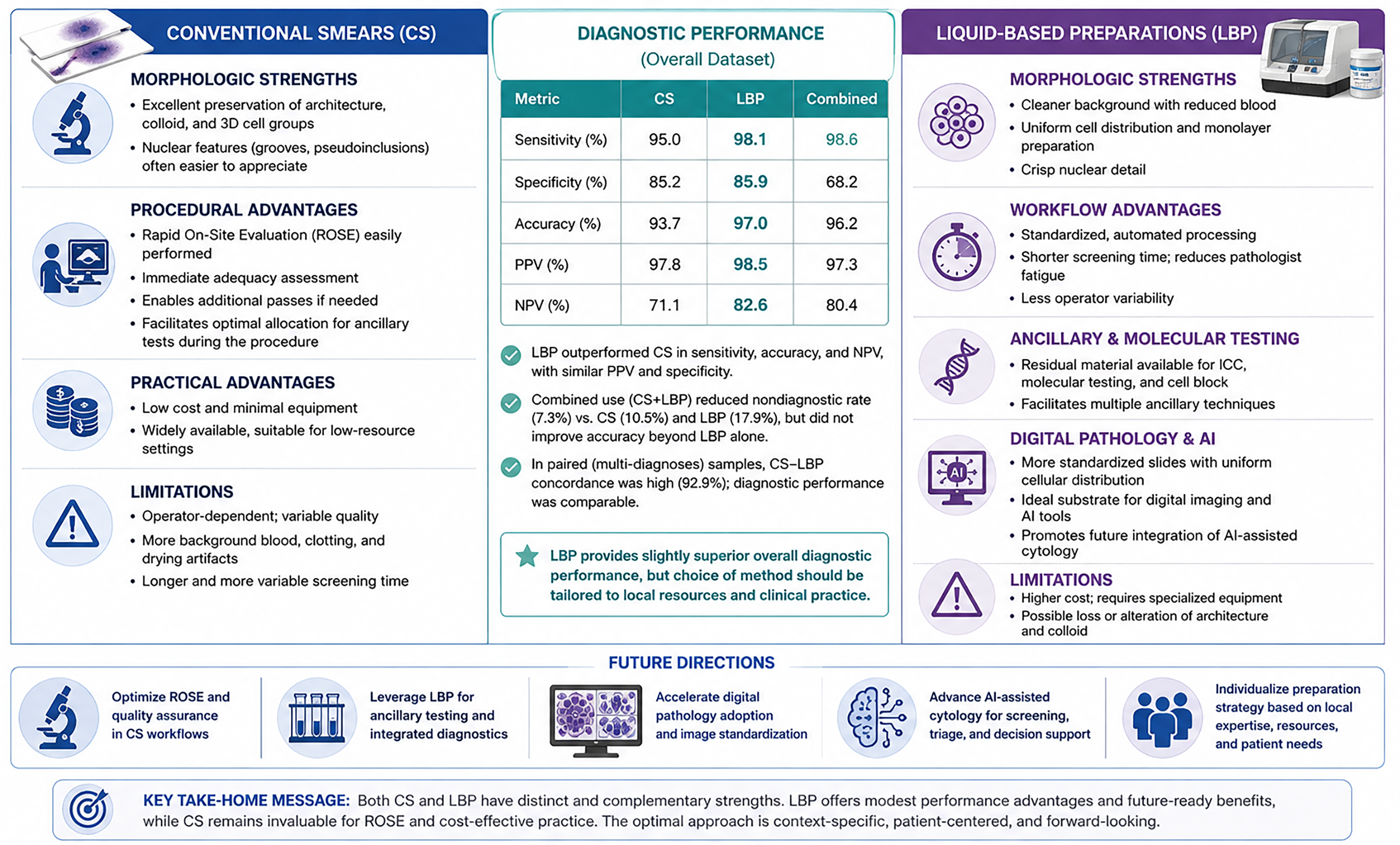
Conventional smears versus liquid-based cytology in thyroid FNA: comparative features, diagnostic performance, and future implications. Generated with the assistance of ChatGPT (OpenAI) based on author-provided concepts and content. The authors reviewed, edited, and approved the final figure and assume full responsibility for its accuracy and interpretation. AI, artificial intelligence; CS, conventional smear; FNA, fine-needle aspiration; ICC, immunocytochemistry; LBP, liquid-based preparation; NPV, negative predictive value; PPV, positive predictive value.
Perhaps the greatest advantage of CS is its compatibility with ROSE. ROSE remains one of the most valuable quality assurance tools in thyroid FNA because it allows immediate assessment of specimen adequacy during the procedure. This reduces nondiagnostic rates, minimizes repeat procedures, and enables optimal triage of material for ancillary testing such as cell-block preparation, immunocytochemistry, flow cytometry, microbiologic studies, and molecular testing. 6 In centers with experienced cytopathologists or cytotechnologists, ROSE substantially improves procedural efficiency and optimal specimen triage.
At the same time, the advantages of LBP are becoming increasingly relevant in modern cytopathology workflows (figure). LBP provides cleaner backgrounds, more uniform cellular distribution, and greater preparation standardization, all of which may significantly reduce screening time and pathologist fatigue. This has been particularly evident in the practice of one of us (M.P.P.) who routinely reviews up to 45 thyroid FNA biopsy cases per day, a workload that would be substantially more difficult to manage efficiently using CS alone. In addition, residual material preserved in collection media can facilitate ancillary studies, including immunocytochemistry, molecular testing, and cell-block preparation, further enhancing the versatility of LBP in contemporary thyroid cytopathology practice.
An especially important future implication relates to digital pathology and artificial intelligence (AI). 7 Emerging AI-assisted cytology platforms such as AIxTHY rely heavily on image standardization and reproducibility. CS slides are inherently variable because of differences in smear thickness, staining quality, air-drying artifact, and cellular overlap, all of which complicate computational image analysis. In contrast, LBP slides provide a more uniform and standardized substrate for digital imaging and machine learning applications. Cleaner backgrounds and monolayer cellular distribution may therefore facilitate algorithm development, automated screening, and AI-assisted cytologic interpretation. As digital pathology adoption accelerates, laboratories may increasingly consider not only the current diagnostic performance of preparation methods but also their compatibility with future computational tools. In this context, LBP may offer strategic advantages that extend beyond traditional morphologic interpretation alone.
Ultimately, the findings by Chen et al. suggest that the choice between CS and LBP should not be viewed as a simple competition between two techniques. Rather, each method possesses complementary strengths that may be better suited to different institutional workflows, laboratory infrastructures, and future technological priorities. Laboratories emphasizing ROSE and low-cost procedural flexibility may continue to favor CS, whereas centers prioritizing standardization, ancillary testing, digital pathology, and AI integration may increasingly adopt LBP-centered workflows.