
Abstract

KEY POINTS
In a retrospective validation study using surgical histopathology as the reference standard, the deployment of a deep-learning artificial intelligence (AI) adapter demonstrated an area under the curve of 0.794, establishing diagnostic equivalence with expert operators and significantly outperforming novice clinicians in risk-stratifying thyroid nodules.
Functioning as a diagnostic filter, the algorithm safely reclassified 55.7% of benign nodules into lower-risk categories, effectively neutralizing human defensive medicine bias and theoretically reducing the unnecessary fine-needle aspiration biopsy recommendation rate to 37.1%.
Economic modeling over a 1-year horizon from a third-party payer perspective yielded an incremental cost-effectiveness ratio of −€8085.56 per optimal clinical decision, confirming AI integration as cost-effective and cost-saving, driven by the reduction of avoidable surgical interventions.
SUMMARY
Background
The contemporary clinical approach to thyroid nodule management is defined by an escalating crisis of overdiagnosis. Driven by the widespread availability of high-resolution ultrasonography, the detection of nonpalpable, sonographically ambiguous thyroid nodules has surged, creating a vast pipeline of patients subjected to serial imaging, fine-needle aspiration biopsy (FNAB), and frequent surgical intervention. 1 Despite this aggressive detection, mortality rates for differentiated thyroid cancer remain static, exposing the systemic overtreatment of low-risk, subclinical disease. 2 This diagnostic cascade imposes an immense economic burden, costing the United States an estimated $25 billion annually. 3 Although risk-stratification systems such as the American College of Radiology Thyroid Imaging Reporting and Data System (ACR-TIRADS) were developed to standardize morphologic assessment and improve specificity, their reliance on subjective visual interpretation is accompanied by high interobserver variability. 4 Consequently, deploying highly specific, reproducible methods to accurately triage benign nodules and curb the cascade of unnecessary interventions is an essential priority for health care resource optimization and clinical stewardship.
Methods
A retrospective cohort analysis was conducted at the Verge de la Cinta Hospital in Spain to evaluate the clinical accuracy and economic utility of the Koios artificial intelligence (AI) system, an artificial intelligence tool for the risk stratification of thyroid nodules. 5 The investigation analyzed 394 high-quality orthogonal ultrasound images extracted from 176 dominant thyroid nodules in adult patients who underwent surgical resection between May 2022 and November 2024. By restricting the cohort to surgically treated patients, the study established definitive histopathology as the reference standard. The sonographic images were independently evaluated using standard ACR-TIRADS criteria by a novice operator (1 year of experience) and an expert operator (6 years of experience). A blinded third expert subsequently evaluated the images using the KOIOS software. This evaluation involved two distinct components: First, the system identified the standard features of the ACR-TIRADS to provide a baseline score and recommendation; second, it used a deep-learning AI adapter to provide a modified risk assessment that algorithmically adjusted the initial classification. Diagnostic performance was quantified by calculating the area under the curve (AUC) of the receiver operating characteristic curves. Concurrently, a decision-tree economic model assessed direct health care costs within a public health system over a 1-year horizon to calculate the incremental cost-effectiveness ratio (ICER), supported by deterministic and probabilistic sensitivity analyses.
Results
Histologic evaluation confirmed malignancy in 36 nodules (20.45%), predominantly papillary thyroid carcinoma, and benign pathology in 140 nodules (79.55%). Diagnostic accuracy demonstrated that the KOIOS AI system integrated with the deep-learning adapter achieved an AUC of 0.794 (95% confidence interval [CI], 0.718–0.871), establishing statistical equivalence with the expert operator (AUC, 0.784; 95% CI, 0.706–0.861; p = 0.754). Both the algorithm and the expert significantly outperformed the novice operator, whose diagnostic capacity was notably inferior (AUC, 0.619, 95% CI, 0.526–0.711; p < 0.001). Although the novice operator achieved elevated sensitivity (94.4%) at the severe expense of specificity (29.3%), the AI system delivered an optimized equilibrium, yielding a sensitivity of 88.9% and a specificity of 70.9%. Economically, the standard-care pathway amassed a per-patient cost of €6036.57, compared to €3463.89 under the AI-assisted paradigm. The resulting ICER was −€8085.56, indicating that the AI approach is a cost-saving strategy, optimizing the rate of correct clinical decisions while simultaneously producing substantial net cost savings. Deterministic modeling isolated surgical expenditures as the primary variable dictating these savings, and probabilistic simulations consistently maintained the AI system as the optimal strategy across all willingness-to-pay thresholds.
Conclusions
The KOIOS AI decision-support system could function as a highly specific, cost-effective adjunct in the clinical management of thyroid nodules. By reliably replicating subspecialty-level sonographic interpretation, the deep-learning algorithm safely reclassifies benign lesions, systematically mitigating overdiagnosis and the financial burden of unwarranted diagnostic thyroidectomies. Large-scale, prospective validation is required to confirm these health-economic efficiencies in broader populations.
COMMENTARY
The integration of artificial intelligence into clinical thyroidology continues to move from computational theory to practical health care application. 6 The investigation by Bodoque-Cubas et al. goes beyond standard validation of algorithmic accuracy, contextualizing deep-learning probability models within health economics and resource utilization.
A central challenge in endocrinology is the subjective nature of ultrasound interpretation. 4 The diagnostic metrics in this cohort quantify defensive medicine bias. The novice operator achieved 94.4% sensitivity, driven by a low specificity of 29.3%. Inexperienced clinicians routinely lower their biopsy threshold, upgrading benign-appearing nodules to ensure tissue sampling. The KOIOS AI system acts as a rationalizing force. Achieving 70.9% specificity without sacrificing sensitivity, the algorithm functions as an effective clinical filter, preventing 55.7% of benign nodules from advancing to biopsy (Figure).
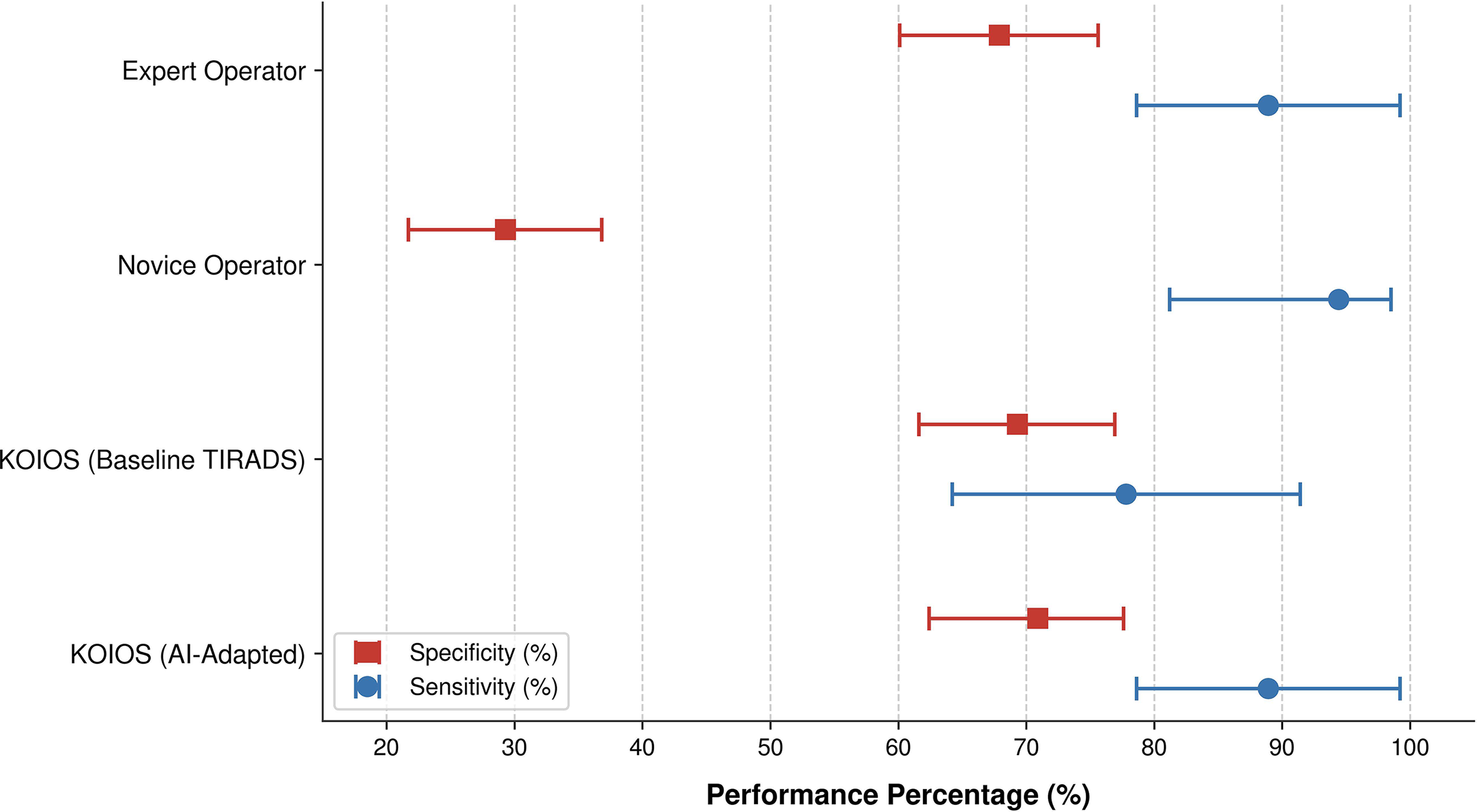
Diagnostic trade-offs in thyroid nodule risk stratification.
Although human operators use the additive ACR-TIRADS lexicon, KOIOS evaluates these foundational characteristics and uses an AI adapter to refine the score using multidimensional, pixel-level feature extraction. This dual approach explains the drop in interobserver agreement between the expert and the AI. By downgrading nodules and shifting low-risk categorizations from 4.6% to 25.6%, the algorithm recognizes benign patterns beyond human visual limitations.
Economically, the negative ICER (–€8085.56) favors implementation, representing a highly attractive strategy for regions lacking specialized endocrine sonographers. While this absolute cost savings reduction is roughly €2572 per patient, the ICER highlights the concentrated financial impact of every additional optimal clinical decision made possible by the AI tool. This cost-saving advantage is driven by avoiding downstream interventions. Indeterminate cytology predictably directs patients toward diagnostic lobectomies, commercial molecular testing, or long-term surveillance. 7 Deploying the AI upstream to classify these nodules as sonographically benign prior to biopsy avoids these expenditures. Notably, the authors amortized the software’s fixed annual cost (€18,500) strictly across the subset of patients requiring FNAB (€105 per patient). Distributing this cost across the entire annual thyroid ultrasound volume (∼1000 cases) would reduce the per-patient burden to roughly €18.50. This methodological choice penalized the software; because it still emerged as the dominant strategy, its true financial benefit is likely underestimated.
Translating these findings into practice requires acknowledging cohort limitations. Dichotomizing the ACR-TIRADS scale, grouping categories 1–3 as benign and 4 and 5 as malignant, masks the algorithm's performance in the clinical gray zone, as categories 3 and 4 represent the primary sources of diagnostic friction. Additionally, reliance on a surgical population acts as a double-edged sword. Although it provides histopathologic truth, it introduces selection bias, creating a filtered subset with a 20.45% malignancy prevalence. In an unselected primary care setting, the positive predictive value will unsurprisingly decrease. The malignant cohort was also overwhelmingly classic papillary thyroid carcinoma, leaving the software's accuracy with rarer malignancies unproven.
Finally, the study assessed human and machine performance in isolation. Previous literature demonstrates that AI provides substantial value as a concurrent decision-support tool, improving the diagnostic confidence and accuracy of novice providers.8,9 Integrating these systems demands coordinated diagnostic stewardship, leveraging the technology as an educational and filtering mechanism to preserve patient health without triggering unnecessary interventions.
The forest plot illustrates sensitivity (blue circles) and specificity (red squares) with 95% confidence intervals for human operators versus the KOIOS artificial intelligence system.