
Abstract

KEY POINTS
Metabolic dysfunction–associated steatotic liver disease (MASLD) affects approximately 30% of people worldwide and has emerged as the most common cause of chronic liver disease. Hypothyroidism contributes to hepatic steatosis through impaired lipid metabolism and worsened insulin resistance. Cross-sectional and case–control studies have reported an association between hypothyroidism and cirrhosis or hepatocellular carcinoma (HCC).
This study examines the association between hypothyroidism and the risk of HCC and cirrhotic complications in a retrospective, territory-wide cohort of patients with MASLD.
A significant association between time-varying hypothyroidism and the risk of liver-related events was observed, whereas baseline thyroid function was less predictive.
SUMMARY
Background
Excess or dysfunctional adipose tissue leads to fat deposition in the liver, known as steatosis, which can potentiate inflammation, oxidative stress, insulin resistance, and vascular dysfunction. This pathophysiological process underlies the cardiovascular-kidney-metabolic syndrome and the development of cardiovascular diseases. 1
Thyroid hormones play a central role in metabolism, and both hypothyroidism and hyperthyroidism can affect lipoprotein and carbohydrate metabolism, thereby contributing to the development of metabolic dysfunction–associated steatotic liver disease (MASLD). 2 There is a strong association between MASLD and primary hypothyroidism. In a large meta-analysis of 764,244,399 adults, hypothyroidism was associated with higher prevalence and severity of MASLD. 3 In a prospective cohort of 387,142 patients in the UK Biobank, those with hypothyroidism had an increased risk of developing MASLD. 4
Although these studies have demonstrated an association between hypothyroidism and MASLD, controversy remains about the clinical outcomes of patients who have both diseases. In the study by Jin et al., 5 the impact of thyroid dysfunction on liver-related events (LREs) was evaluated over time.
Methods
This retrospective cohort study used Clinical Data Analysis and Reporting System data from all public hospitals and clinics in Hong Kong, China, which together represent 80% of the local population. All patients with an ICD-9-CM code for MASLD diagnosed between 2000 and 2024 were identified. Thyroid dysfunction was defined by exposure to levothyroxine replacement therapy, thyroid function test results, or ICD-9-CM diagnosis codes. Thyroid status was assessed at baseline and during follow-up. The outcome was LREs, defined by ICD codes as the diagnosis of hepatocellular carcinoma, cirrhotic complications, or liver-related death during follow-up.
The association between baseline thyroid status and baseline cirrhosis was estimated using logistic regression, while the cumulative incidence function for LREs was estimated using the Aalen–Johansen method. Time-dependent analyses were conducted to further explore the dynamic relationship between thyroid function and LRE risk over the follow-up period.
Results
Among 20,478 eligible patients, 1.9% had cirrhosis, 8.3% had hypothyroidism, and 2.9% had hyperthyroidism at baseline. Thyroid dysfunction was associated with a higher risk of cirrhosis than euthyroidism. When hypothyroidism was stratified by severity, overt hypothyroidism remained significantly associated with cirrhosis (adjusted Odds Ratio [OR], 1.52; 95% Confidence interval [CI], 1.04–2.21; p = 0.029), whereas subclinical hypothyroidism was not (adjusted OR, 1.29; 95% CI, 0.71–2.35; p = 0.401). The incidence of LREs, with a median follow-up of 4.8 years, did not differ significantly across baseline thyroid status after adjustment.
During follow-up, 0.9% of the population developed LREs. Higher thyrotropin (TSH) levels, treated as a time-varying covariate, were significantly associated with a higher risk of LREs.
Compared with patients with normal TSH levels, those with high TSH levels had a 2.49-fold increased risk of developing LREs (adjusted cause-specific hazard ratio [CSHR], 2.49; 95% CI, 1.51–4.13; p < 0.001). Those with very high TSH levels (>10 mIU/L) had an even greater risk (adjusted CSHR, 4.91; 95% CI, 1.56–15.47; p = 0.006).
Relative to euthyroidism, time-varying hypothyroidism was significantly associated with an increased risk of LREs (adjusted CSHR, 3.19; 95% CI, 2.06–4.94; p < 0.001). Both subclinical (adjusted CSHR, 2.58; 95% CI, 1.56–4.29; p < 0.001) and overt (adjusted CSHR, 6.41; 95% CI, 2.96–13.85; p < 0.001) hypothyroidism independently conferred elevated risk.
Conclusions
In this study, time-varying hypothyroidism was significantly associated with a higher risk of LREs in patients with MASLD. Baseline thyroid function was less predictive, supporting dynamic thyroid function testing as a potential strategy to reduce the risk of liver-related complications.
COMMENTARY
Thyroid hormones are central to metabolic regulation, and the liver is a key organ in thyroid-metabolic crosstalk. As MASLD has emerged as an important risk factor for cardiovascular and kidney disease, interest in thyroid actions on the liver has grown, particularly following the development of thyroid hormone receptor β agonists that can reverse early-stage liver fibrosis. 6
Hypothyroidism impairs lipophagy and fatty acid catabolism, leading to excess free fatty acids that trigger oxidative and endoplasmic reticulum stress, contributing to hepatocellular injury and steatosis. In response to liver injury, altered deiodinase activity further reduces intrahepatic thyroid hormone signaling, a phenomenon termed the “intrahepatic hypothyroidism” phenotype in metabolic dysfunction–associated steatohepatitis (MASH). These disturbances exacerbate oxidative stress, inflammation, and progressive liver damage in MASLD. Furthermore, the direct effect of elevated serum TSH levels on hepatic TSH receptors, as observed in preclinical studies, may also contribute to increased hepatic triglyceride content. 3
However, the role of hypothyroidism in MASLD and its clinical consequences is not fully explored. In this large cohort study, time-varying TSH levels were associated with MASLD progression, and hypothyroidism may be an accelerator of LREs. Compared with previous longitudinal studies assessing this association, this study uses time-varying models that capture whether thyroid dysfunction persists, worsens, or resolves over time, thereby highlighting the limitations of a single baseline assessment used in prior studies.
Some limitations of this study include the use of ICD-9-CM diagnosis codes to define variables such as MASLD, cirrhosis, or thyroid dysfunction, rather than direct clinical assessment, which may introduce misclassification bias. Furthermore, several clinical parameters, including BMI, waist circumference, and Fibrosis-4, were missing in more than 60% of patients. Although multiple imputation by chained equations was used to account for these missing covariates, residual uncertainty may remain.
The slogan “When you see obesity, think liver” has become increasingly relevant in the era of MASLD. The findings discussed here suggest that the thyroid may be another key piece of the metabolic puzzle. Perhaps the next iteration of this message should be: “When you see obesity, think liver—and remember the thyroid” (Figure).
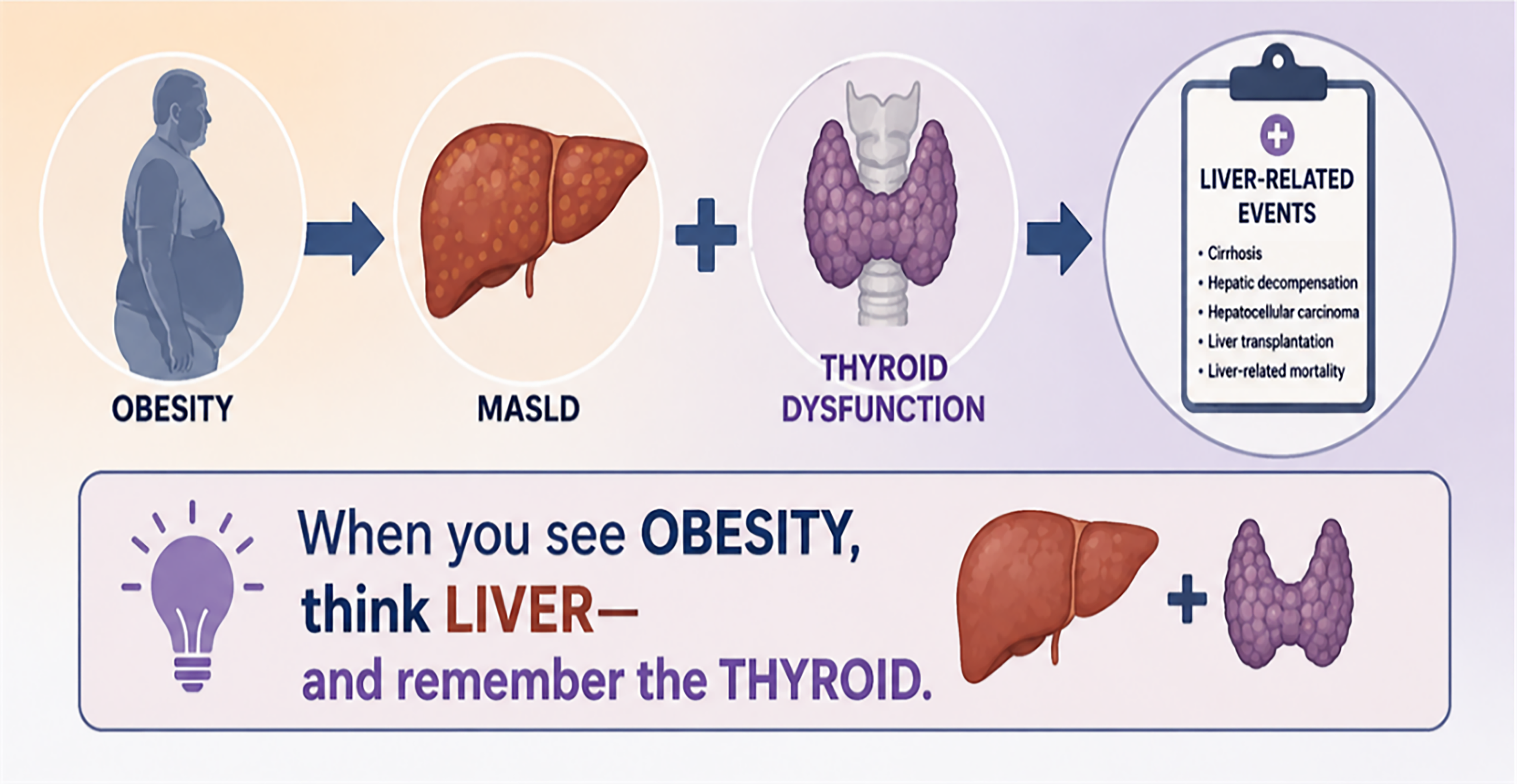
Obesity Contributes to MASLD, While Thyroid Dysfunction Increases the Risk of Liver-Related Events. Dynamic thyroid function assessment may improve risk prediction. Visual representation was generated with the assistance of ChatGPT (OpenAI) based on author-provided concepts and content. The author reviewed, edited, and approved the final figure and assumes full responsibility for its accuracy and interpretation.