
Abstract
Executive Summary
Venezuela’s economic crisis has triggered mass migration; more than 3.4 million Venezuelans have fled to other countries in the region and beyond. An assessment mission to Cúcuta, in the Colombian border state of North Santander, was undertaken from July 26 to August 1, 2018, and to Bôa Vista and Pacaraima, in the state of Roraima, Brazil, between August 24 and 28, 2018. Interviews were conducted with key informants, including health providers and organizations engaged in the humanitarian response. Secondary analysis of gray literature and data shared by key informants was also undertaken. Surveillance data demonstrate increases in infectious diseases, as well as adverse maternal and neonatal health outcomes, among Venezuelans in North Santander and Roraima.
Summary of Findings for North Santander
Reportable public health surveillance events among Venezuelans increased from 182 in 2015 to 865 in the first half of 2018.
In 2018, the most common reported events included gender-based and intrafamiliar violence (17 percent), malaria (15 percent), and acute malnutrition in children <5 years (9 percent).
There were 14 measles cases reported between January and June 2018 (compared to none in the previous years), the majority associated with migration from Venezuela.
Thirty-six cases of maternal morbidity and two cases of maternal mortality among Venezuelans were observed in the first half of 2018 (compared to three cases of maternal morbidity and no maternal deaths in 2015). Low-birth-weight Venezuelan births rose from three in 2015 to 34 in 2017.
Between January 2017 and June 2018, emergency medical attention was provided to 19,108 Venezuelans in government health facilities.
Summary of Findings for Roraima
In 2018, there were 355 cases of measles in Roraima (compared to none in previous years) — all cases had the genotype lineage originating in the 2017 Venezuelan measles outbreak.
Children younger than one year old (812.1/100,000) had the highest measles incident rate in Roraima, followed by children 1–4 years old (245.7/100,000).
Malaria cases among Venezuelans increased 3.5-fold from 2015 to 2018 (1,260 vs. 4,402 cases).
As of August 2018, 171 HIV-infected Venezuelans were receiving HIV care at the Coronel Motta Clinic in Bôa Vista, Roraima.
In 2018, 1,603 Venezuelan women gave birth at the Hospital Materno-Infantil in Bôa Vista, and by mid-2018, 10,040 Venezuelans had received outpatient care and 666 had been hospitalized at the Hospital General Roraima.
In Colombia, primary healthcare is not available to Venezuelans, and provision of emergency care is perceived as unsustainable given current funding mechanisms. In Brazil, primary care is available to Venezuelans, but the healthcare system is under severe strain to meet the increased demand for care and is facing unprecedented shortages in medications and supplies. There is an urgent need to expand the humanitarian health response in Colombia and Brazil, both to ensure health among Venezuelans and to protect public health in border areas.
Introduction
The Venezuelan economic, political, and health crisis has triggered an exodus of Venezuelans to countries throughout the region. Hyperinflation in Venezuela is the highest in the world, at 1.37 million percent in 2018, with projections for 2019 in excess of 10 million percent (Reuters 2018). Hyperinflation, coupled with shortages of food, medicine, and healthcare, have contributed to increased humanitarian needs that are not being adequately addressed due to the government’s lack of acknowledgment of the crisis and refusal to accept humanitarian aid (Fraser and Willer 2016; Bello et al. 2017). The deteriorating public health infrastructure has resulted in rising infant and maternal mortality; increased transmission of vector-borne illnesses, HIV, and tuberculosis; and outbreaks of vaccine-preventable diseases (García, Correa, and Rousset 2019; Grillet et al. 2019; Page et al. 2019; Torres and Castro 2019). The number of Venezuelans fleeing the country has dramatically increased in recent years. As of late 2018, the International Organization for Migration (IOM) estimated that 3.4 million Venezuelans had fled the country, and the United Nations High Commissioner for Refugees (UNHCR) reports a 2000 percent increase in Venezuelan asylum applications in 2018 (UNHCR 2018a; UNCHR/IOM 2019).
Colombia is the primary destination of most Venezuelan “migrants,” a generic term used in this article to connote the unclear status of Venezuelans ranging from economic migrants to refugees. Many Venezuelans, however, pass through Colombia en route to other countries — primarily Peru and Ecuador. As of mid-2018, there were an estimated 1.1 million Venezuelans and Colombian returnees from Venezuela residing in Colombia, of which 909,000 needed health assistance (USAID 2018). UNHCR reported there were 4,170 Venezuelan asylum seekers in Colombia in 2018, and 657,732 Venezuelans with other forms of legal stay, meaning the vast majority of migrants do not have legal status in Colombia (UNHCR 2018b). Of the 442,462 Venezuelans registered by the Colombian government in 2018, the majority were adults aged 18–59 years (70.6 percent), followed by children (26.8 percent) and older adults (2.6 percent). Nearly 20 percent were from groups that traditionally have high health needs, including 50,729 children younger than five years (11.5 percent), 16,812 with chronic health conditions (3.8 percent), 15,705 pregnant and lactating women (3.5 percent), and 468 with infectious diseases (0.1 percent). Of the latter, 202 had tuberculosis and 21 HIV/AIDS. The departments in the border areas had the highest concentration of Venezuelans, with the largest number in North Santander (n = 82,286, 18.6 percent) followed by La Guajira (n = 74,874, 16.9 percent) (RAMV 2018).
Brazil has also received a significant number of Venezuelans, and hosts the sixth largest overall migrant population in South America after Colombia, Peru, Ecuador, Argentina, and Chile. As of December 2018, 83,893 Venezuelans had applied for refugee status in Brazil. They represent almost 10 percent of the population in the receiving state of Roraima, a geographically isolated region that borders southern Venezuela with low population density and limited economic opportunities (UNHCR 2018a). In 2018, in response to increased migration, the governor of Roraima attempted to temporarily shut the border with Venezuela, citing “the social and economic imbalance brought about by this strong migration wave.” Although the motion was rejected by Brazil’s supreme court, it illustrates the tensions arising from mass outmigration (Rodrigues 2018).
The growing number of migrants is contributing to regional public health concerns, in particular with respect to spread of infectious disease and increased burden on the Colombian and Brazilian health systems (USAID 2018). We undertook this analysis to better characterize the migrant health situation and needs in Colombia’s and Brazil’s most affected provinces, North Santander and Roraima, respectively, with the aim of describing the extent of the crisis and informing health sector response planning.
Methods
A joint team of public health researchers and physicians (authors SD, KRP, and FH) from Johns Hopkins School of Public Health and the National University of Colombia, and Human Rights Watch, conducted an assessment mission of North Santander State, Colombia, from July 26 to August 1, 2018, and in Roraima State, Brazil, between August 24 and 28, 2018. The missions included visits to humanitarian organizations, border crossings, service provision sites, and other community locations of interest with a focus on the Colombian city of Cúcuta and the Brazilian cities of Bôa Vista and Pacaraima. A total of 30 individual and group informant interviews were conducted with approximately 58 key informants from organizations engaged in the humanitarian response (Table 1). Key informants were asked to describe their organization’s response to the increase in migrants, list challenges and lessons learned, and share relevant data when available. While the guiding themes and general content of information were similar in key informant interviews, a standardized interview guide was not used because each organization had a different role in the response, making a more iterative approach to interviews preferable.
Key Informant Characteristics by Country.
All interviews were conducted in Spanish or Portuguese; detailed notes were taken, but interviews were not audio recorded. In addition to information provided orally, and in some cases via PowerPoint presentations, organizations were asked to share relevant statistics that could aid in the characterization of the health and nutrition situation of Venezuelans at the borders. This included hospital statistics and public health events, such as infectious diseases, infant and maternal deaths, and vaccine-preventable illnesses that are reported to authorities via surveillance systems.
In addition, a gray literature search was conducted of key websites (government websites and ReliefWeb, which catalogs documents by organizations engaged in humanitarian response), as well as a structured search of peer-reviewed articles indexed in PubMed. These activities were reviewed by the Johns Hopkins Bloomberg School of Public Health Institutional Review Board. They were determined to be public health practice and not human subjects research.
Results
Migrant Flows
Colombia
Migration in North Santander is complex: the border is open, many people cross without documentation, and no registry is maintained, all of which present a challenge regarding the characterization of the scale and type of population flow. Key informant interviews indicate the majority are “day crossings,” in which Venezuelans cross to take advantage of income-generating opportunities, markets, and services such as community kitchens and primary healthcare. These populations have access to legal stay in Colombia through border mobility cards — of which 834,954 had been approved at the end of 2018 (GIFMM 2018a). A second group are Venezuelans seeking to migrate to Colombia or other destinations such as Peru and Ecuador. In December 2018, the Colombian government introduced temporary transit permits allowing foreigners with and without passports 15 days to travel through Colombia to a third destination country. The third category are Colombians who are returning on a more permanent basis back to Colombia; there were an estimated 250,000 returnees in 2018, and, with Colombian returnees, they comprised 40 percent of arrivals from Venezuela (GIFMM 2018b; IOM 2018). The mix of these groups varies at the different border crossings and throughout time. The distinction between Colombians and Venezuelans is often unclear due to dual-nationality households and documentation issues. Surveillance and health service provision statistics described in the following sections are reported by nationality, and thus underrepresent the full scale of the migration crisis because they do not include Colombian returnees.
Brazil
Roraima is a geographically isolated area with the lowest population levels in Brazil and limited economic opportunities. According to immigration records, 114,974 Venezuelans crossed the Pacaraima border in the first eight months of 2018; among them, 29,771 returned to Venezuela and 85,203 stayed in Brazil. Net entries more than quadrupled from 2016 to 2017, and net entries in 2018 were more than double the entries in 2017. Most Venezuelan migrants settle in the border town Pacaraima, with a population of around 15,580, or travel 200 km south to Bôa Vista, with a population of approximately 375,000 inhabitants (Instituto Brasileiro de Geografia e Estatística 2018). Few travel to other Brazilian cities due to prohibitive transportation costs. The Brazilian government has deployed its armed forces to coordinate the migrant crisis response. In collaboration with UNHCR, the armed forces opened 12 migrant shelters in Pacaraima and Roraima as part of a program called Operação Acolhida (Welcome Operation; Casa Civil 2018). Relocation of Venezuelans to other areas of the country with increased economic opportunities is ongoing, but the process has been slow; as of late September 2018, only 1,976 Venezuelans had been resettled (Gonçalves 2018). In September 2018, more than 6,000 Venezuelans were living in shelters in Roraima, which were at capacity, and many were still in the streets (Casa Civil 2018).
Infectious Diseases
Colombia
There has been a sharp increase in recent years in reportable public health surveillance events among Venezuelans in North Santander: 182 events were reported in 2015 compared to 865 in the first half of 2018 (through July 15). The most frequently reported events in 2018 were suspected cases of gender-based and intrafamiliar violence (17 percent), malaria (15 percent), and acute malnutrition in children <5 years (9 percent). 1 Infectious diseases accounted for only 19 percent of events in the first half of 2018 (n = 165). The most frequent infectious diseases were acute respiratory tract infections (ARIs) or flu-like symptoms from sentinel site surveillance (24 percent), tuberculosis (20 percent), HIV/AIDS (18 percent), varicella (15 percent), and hepatitis A (15 percent) (Figure 1a; North Santander Health Institute 2018a). It is unclear if the increasing number of infectious disease cases among Venezuelans is having an impact on incidence in North Santander more generally. A recent analysis of HIV/AIDS cases in the Colombia–Venezuela border region suggests that the gradual rise in HIV/AIDS cases preceded the recent influx of Venezuelans (Gomez Ochoa 2018); access to antiretroviral therapy for HIV-infected Venezuelan migrants arriving in Colombia is limited to those with health insurance.
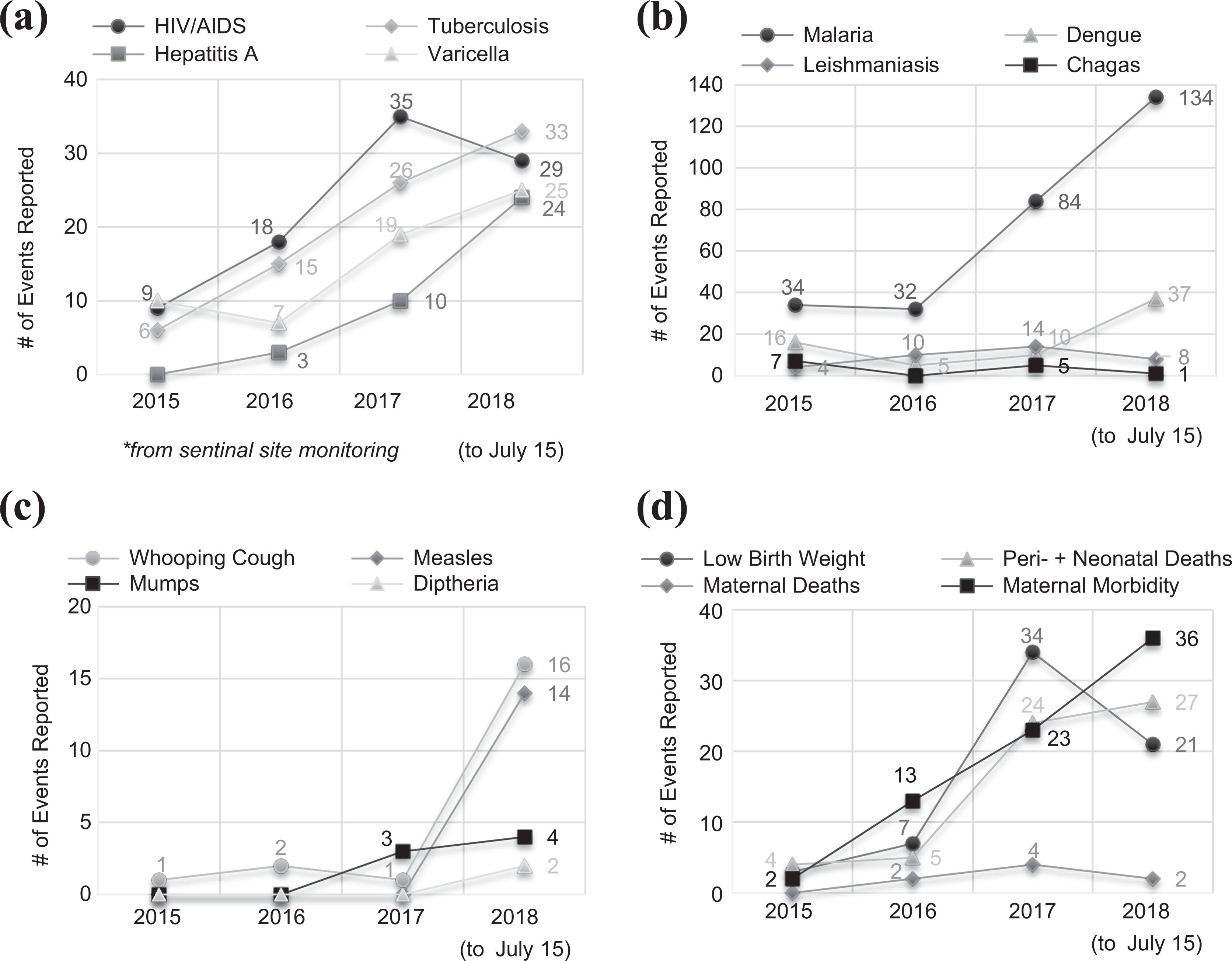
Public health surveillance events among Venezuelans in North Santander, Colombia, 2015–2018. (a) Infectious diseases. (b) Vector-borne diseases. (c) Vaccine-preventable diseases. (d) Maternal and neonatal health.
Vector-borne diseases comprised 21 percent (n = 181) of 2018 surveillance events among Venezuelans; the most common were malaria (74 percent), dengue (20 percent), and leishmaniasis (6 percent) (Figure 1b). The rise in malaria cases is a likely reflection of the regional increase in cases, with an especially strong resurgence in Venezuela (PAHO/WHO 2018a). From 2013 to 2014, malaria incidence in Venezuela increased 69 percent; a total of 406,000 cases were reported in 2017, a fivefold increase compared to 2013 figures. Vaccine-preventable diseases accounted for only 4 percent of 2018 events (n = 36) among Venezuelans in North Santander and primarily consisted of whooping cough (44 percent) and measles (39 percent); the 2018 figure represents a significant increase from one–four events annually in 2015–2017 (Figure 1c).
The increase in measles cases is likely attributable to an ongoing outbreak in Venezuela with 7,233 cases reported from 2017 to mid-2018. Emergence of measles in Colombia began in March 2018. In the early stages of the outbreak, through July 2018, 58 percent of cases were imported and 40 percent were imported-related (PAHO/WHO 2018b). Of the 212 measles cases reported in Colombia in 2018, 103 required hospitalization, and none resulted in deaths. In early 2019, the outbreak was still ongoing with cases under investigation in North Santander and other areas of the country (PAHO/WHO 2019). One of the efforts to combat the border health crisis is provision of vaccinations; in 2017 and the first half of 2018, respectively, 58,580 and 86,536 vaccinations were provided at three North Santander border crossings (in addition to lower numbers elsewhere) to vulnerable groups, the majority of which are Venezuelan (Colombian MoH 2017).
Brazil
In Roraima, a measles outbreak following the Venezuelan outbreak that began in 2017 and endemic malaria are the principal health concerns among the Venezuelan population. In 2018, there were 10,274 confirmed cases of measles and 14 deaths attributed to measles in Brazil (PAHO/WHO 2019) (Figure 2a). The majority of cases occurred in the state of Amazonas (9,778), followed by Roraima (355 cases) (PAHO/WHO 2019). The genotype lineage in all confirmed cases is identical to the lineage of the 2017 measles outbreak in Venezuela (D8). In Roraima, Venezuelans accounted for 61.1 percent of confirmed cases and indigenous people (not exclusively Venezuelan) for 41.1 percent of cases (Ministério da Saúde 2019a). Half (50.1 percent) of confirmed cases occurred in Bôa Vista, which has the largest migrant population in the state but the lowest measles vaccination coverage (Ministério da Saúde 2019a). The cumulative incidence rate of confirmed cases in Roraima is 80.0 per 100,000 inhabitants, with the highest incidence in children younger than one year old (812.1/100,000), followed by children one–four years old (245.7/100,000) (PAHO/WHO 2019). During a three-day vaccination campaign, 33,403 doses of measles vaccine were administered among children younger than five years old in Roraima, improving measles vaccination coverage in Bôa Vista from 66.8 percent to 87.7 percent (Ministério da Saúde 2018a). Since mid-2018, weekly cases have been decreasing in the state. Although there is an ongoing outbreak of diphtheria in Venezuela and Brazil, cases in the Brazil outbreak have predominantly occurred outside Roraima (PAHO/WHO 2018c). In 2017, there was one confirmed case of diphtheria in Roraima in a 10-year-old Venezuelan child; no diphtheria cases were reported in Brazil in 2018 (Ministério da Saúde 2018b).
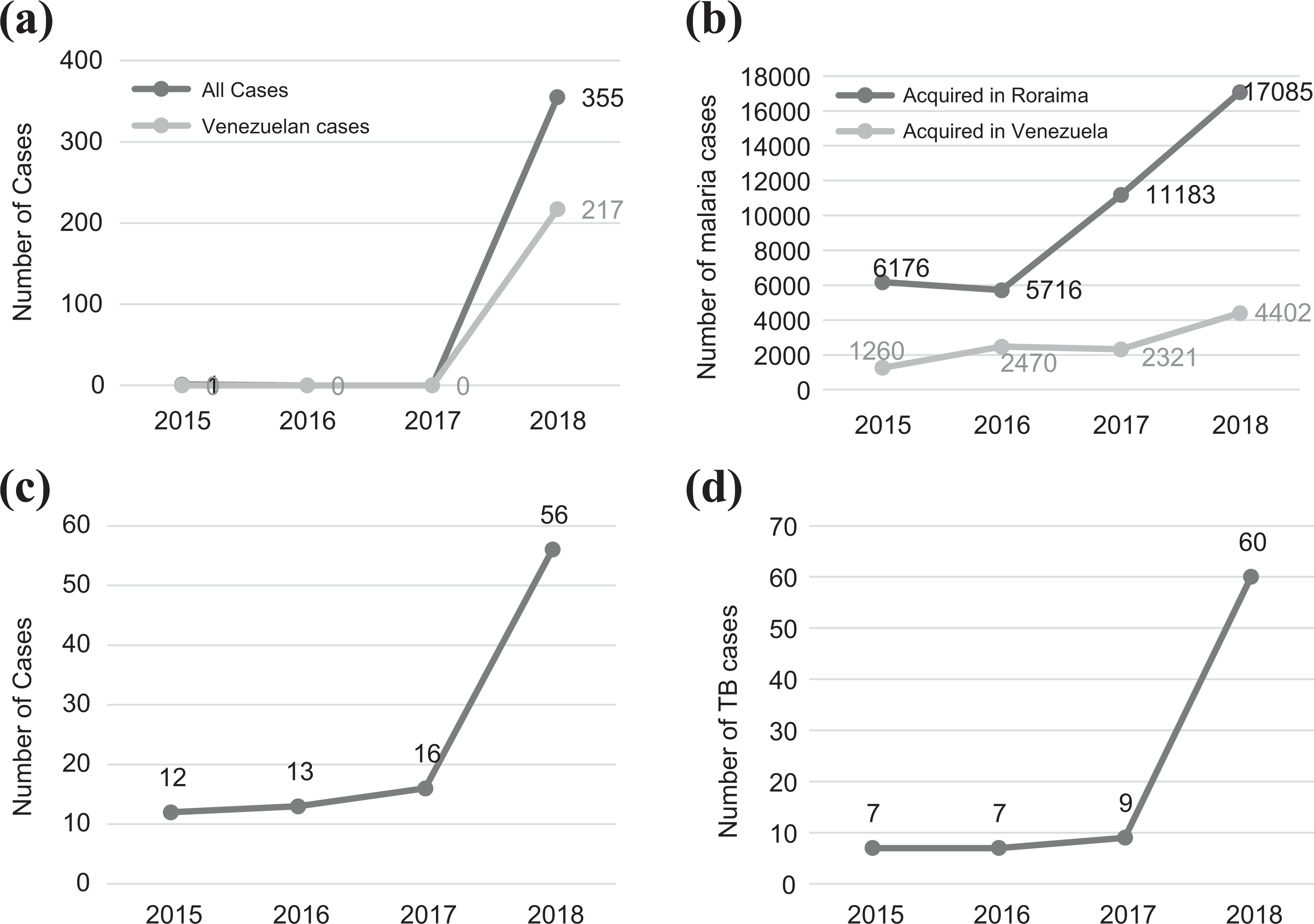
Public health surveillance events among Venezuelans in Roraima, Brazil, 2015–2018. (a) Measles. (b) Malaria. (c) New HIV diagnoses (Ministério da Saúde 2018c). (d) Tuberculosis.
Vector-borne diseases present a significant health problem in Roraima, where malaria is endemic; the annual parasite index (API) ranged from 15.4 to 17.7 per 1,000 inhabitants between 2013 and 2016. In 2017, there was a marked increase in malaria cases, evident in a 54.8 percent rise in the API from the prior year (17.7/1,000 vs. 27.4/1,000). Malaria among Venezuelans began increasing in 2015, and it increased 3.5-fold from 1,260 in 2015 to 4,402 in 2018 (Figure 2b). Among Venezuelans, 67.8 percent of 2018 cases were attributed to Plasmodium vivax, 28.8 percent to Plasmodium falciparum, and 3.3 percent to mixed infections. Venezuelans accounted for 28.3 percent of all confirmed cases and 55.6 percent of all malaria-related deaths in 2018 (Ministério da Saúde 2018a).
In contrast to Colombia, where access to antiretroviral therapy is cost-prohibitive for most Venezuelans, migrants with HIV have access to free antiretroviral therapy in Brazil, regardless of immigration status. Given drug shortages in Venezuela — where an estimated 58,000 people with HIV do not have access to antiretroviral therapy (PAHO/WHO/UNAIDS 2018) — some Venezuelans seek care in Brazil. Physicians at the Roraima Hospital and at the Coronel Mota Specialty Clinic reported that HIV-infected Venezuelan patients were much more likely than Brazilian patients to present with serious AIDS-defining conditions, often requiring prolonged hospitalization. Treatment interruptions or inadequate therapy (i.e., dual instead of triple therapy, or every-other-day therapy) was common due to drug shortages in Venezuela, placing patients at risk for acquired drug resistance. According to 2018 surveillance data, 56 Venezuelan patients were diagnosed with HIV in Roraima (Figure 2c) (Ministério da Saúde 2019b), and as of August 2018, 171 HIV-infected Venezuelans, who accounted for 8.3 percent of the total population, were receiving continuous HIV care at the Coronel Mota Clinic (most were diagnosed prior to 2018).
Tuberculosis (TB) cases among Venezuelans living in Roraima had remained stable between 2013 and 2017, with 32 cases of active TB reported during this period. In 2018, however, 60 cases were reported, including one case of multidrug-resistant (MDR) TB in an indigenous patient housed in a shelter (Figure 2d) (Ministério da Saúde 2018b).
Maternal and Child Health
Colombia
Maternal and peri-/neonatal health events comprised 10 percent of reportable events among Venezuelans in North Santander in the first half of 2018, with all indicators following an increasing trend since 2015 (Figure 1d) (North Santander Health Institute 2018a). Low birth weight and peri-/neonatal mortality among Venezuelan infants rose drastically; there were four peri-/neonatal deaths in 2015 compared to 27 in early 2018. Similarly, 36 cases of maternal morbidity and two cases of maternal mortality were observed in the first half of 2018, whereas in 2015, only three cases of maternal morbidity and no maternal deaths were reported. Greater frequency of adverse maternal and neonatal health outcomes among Venezuelans in North Santander mirrors the most recent available Venezuelan statistics, which indicated increases in infant and maternal mortality of 33 percent and 66 percent, respectively, from 2015 to 2016 (Umer 2017). The tertiary hospital in Cúcuta, Erasmo Meoz University Hospital, delivered 1,204 Venezuelan infants in the first five months of 2018, and by mid-2018 more than half of births were to Venezuelans (Hospital Universitario 2018). Hospital staff report the increased caseload has translated to longer wait times and capacity concerns. Key informant interviews with health providers indicated that perceived inaccessibility of safe delivery in Venezuela was a driver of migration to Colombia among pregnant women, and that inadequate prenatal care in Venezuela contributed to high levels of complications observed among Venezuelan women delivering in Colombia.
Brazil
Likewise, the director of the 266-bed Hospital Materno-Infantil in Bôa Vista also reported a dramatic increase in Venezuelan use of obstetric services. In 2018, 1,603 Venezuelan women had given birth at the hospital, compared to 556 in 2017 and 288 in 2016 (Figure 3a). Care of Venezuelan women is complicated by low rates of prenatal care and high rates of maternal anemia and malnutrition. Compared to Brazilian women, Venezuelan women were 20 percent more likely to have a C-section (43.6 percent vs. 36.0 percent), and in 2017, 33.4 percent of all deliveries and 63.2 percent of C-sections among Venezuelan women were considered high risk (Hospital Materno-Infantil 2018). At the time of our visit, the 42-bed neonatal intensive care unit was at capacity, and a housing complex for mothers with newborns in the neonatal intensive care unit was primarily occupied by Venezuelans. The director reported shortages of intravenous fluids, glucose strips, ceftriaxone, gentamycin, and surfactant, and had received a three-month emergency supply of medications through an emergency petition to the state.
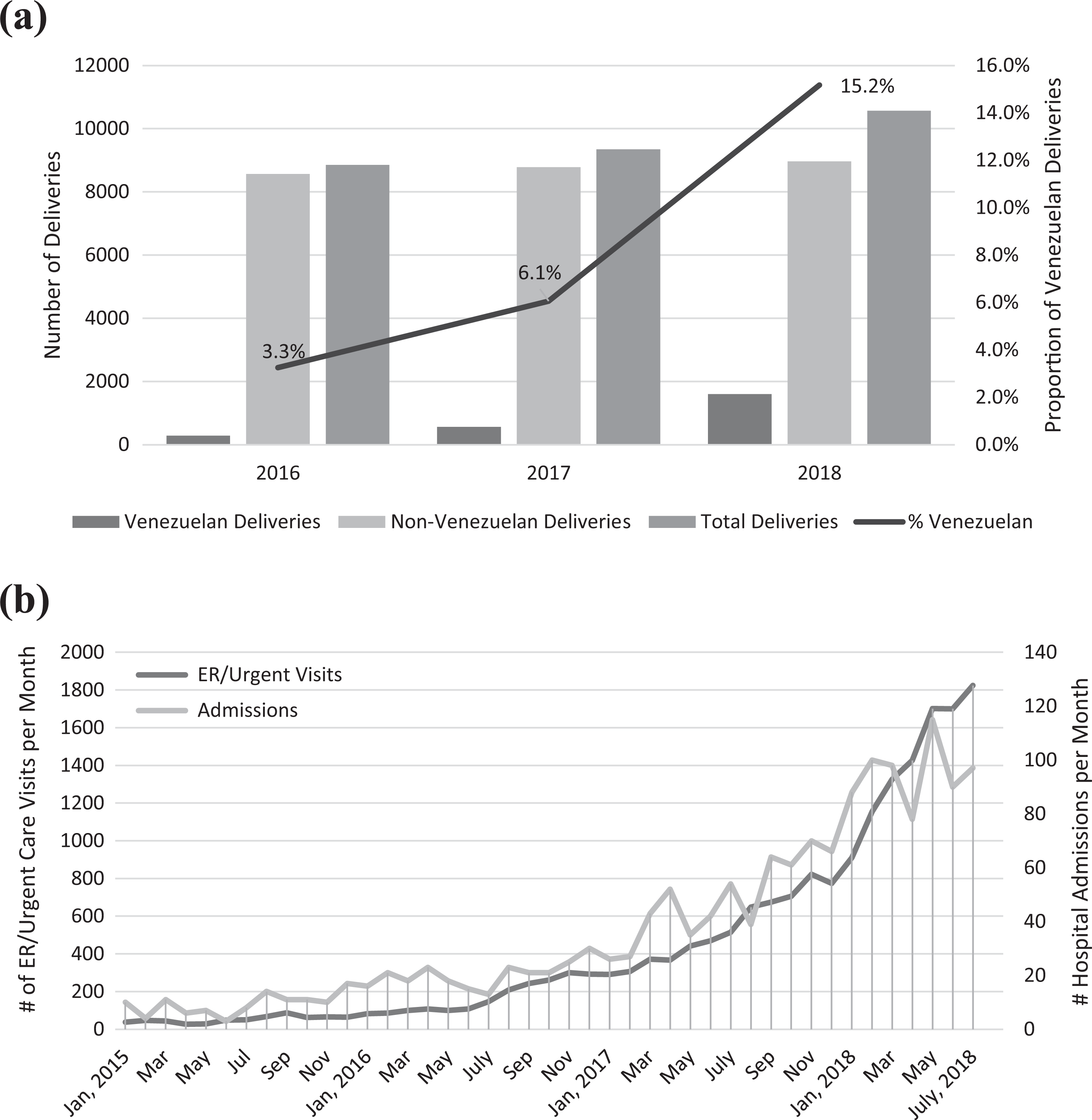
Health services provided to Venezuelans in Roraima, Brazil. (a) Trends at the Hospital Materno-Infantil, Roraima, 2016–2018. (b) Trends at Roraima General Hospital, 2015 to mid-2018.
Health Service Provision
Colombia
Colombia provides emergency medical care to Venezuelans at no cost in government health facilities (Colombian MoH 2017). In most cases, however, Venezuelans are denied access to non-emergency health services (i.e., primary, secondary, and tertiary care) at public facilities. Despite these restrictions, the burden of Venezuelans on health services in North Santander is considerable. Between January 2017 and the end of June 2018, emergency medical attention was provided to 19,108 Venezuelans in government health facilities in North Santander, and there were an additional 5,877 mobile clinic visits (Figure 4a) (North Santander Health Institute 2018b). The Colombian Red Cross is the main provider of primary care, and in 2018 mobile health units were scaled up to reduce the burden at health facilities; by the end of 2018, 17 Red Cross migrant assistance posts had been established in North Santander (GIFMM 2018b). Several other international organizations also began scaling up health sector response activities in 2018 (GIFMM 2018b).
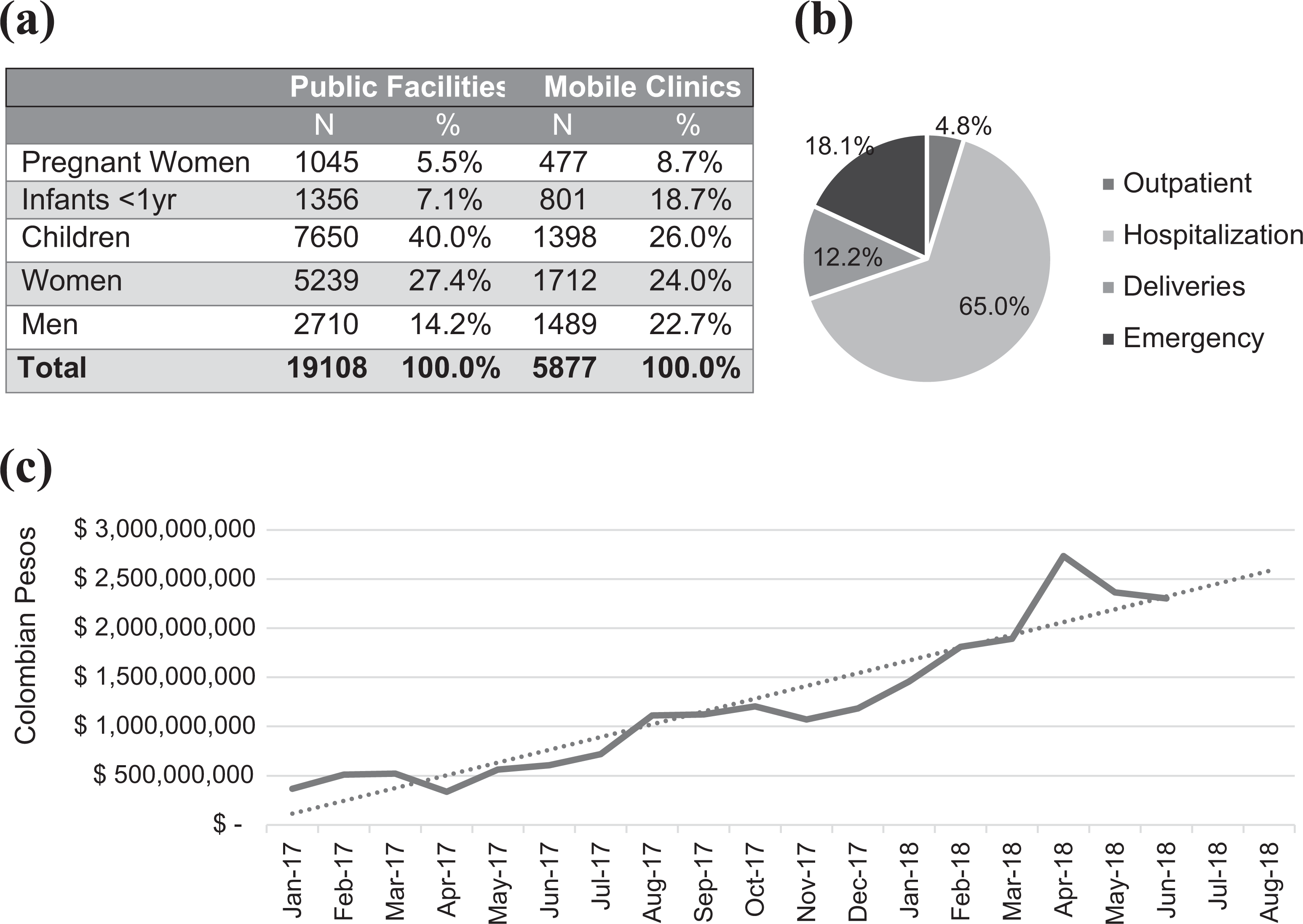
Health services provided to Venezuelans in North Santander, Colombia. (a) Venezuelans attended in North Santander, 2017 to mid-2018. (b) Venezuelans attended at Erasmo Meoz University Hospital, January to May 2018. (c) Billing trends for Venezuelans at Erasmo Meoz University Hospital, 2017 to mid-2018.
Erasmo Meoz University Hospital in Cúcuta is the only tertiary hospital in North Santander, and it receives most Venezuelan patients. The Venezuelan case load increased by 248 percent from the first quarter of 2017 to the first quarter of 2018. The hospital treated 9,875 Venezuelan patients in the first five months of 2018, which accounts for approximately 60 percent of Venezuelan cases seen at all public facilities in North Santander. Of Venezuelans who attended in the first five months of 2018, 65 percent were categorized as hospitalizations, 18 percent as emergency care, 12 percent as deliveries, and 5 percent as outpatient consultations (Figure 4b) (Hospital Universitario 2018).
Public hospitals are authorized to provide only basic emergency care, which limits the extent of treatment they can provide — for example, they may be authorized to manage symptoms but are not authorized to treat the underlying condition. There are no referral pathways for Venezuelans because they lack insurance, which prevents transfers to private hospitals and public specialty hospitals located in major cities. In addition, these hospitals are unreachable for most Venezuelan patients due to distance, cost, migration status, and government travel restrictions. Venezuelans sometimes succeed in obtaining official rulings by judges known as tutelas that entitle them to receive life-saving non-emergency care. The process is complex, however, and often too slow for urgent cases. Access to non-emergency care remains a critical gap when neither government nor nonprofit clinics are able to attend to more complex cases such as HIV/AIDS, diabetes, cancer, and other noncommunicable conditions. Similarly, access to medicines remains financially out of reach for most Venezuelans, although medications for a small number of infectious diseases (e.g., malaria and TB) and immunizations are provided free of charge via government-supported public health programs.
While the government has the capacity to address Venezuelan emergency health needs, sustainability is a concern. The World Health Organization and UNHCR provide support to public facilities. The Colombian government, however, bears most of the expenses. Costs of vaccinations, emergency care, and rapidly accruing expenses for non-emergency care as a result of tutelas were a significant concern among Colombian health officials in key informant interviews. Overall expenses for Venezuelans treated at Erasmo Meoz University Hospital, which attends to the majority of complicated Venezuelan cases, were more than US$720,000 in 2018 (Figure 4c). The government is also supporting select humanitarian cases, to the extent that resources allow; for example, this is being done with some childhood cancers.
Brazil
In accordance with the Brazilian Constitution, universal healthcare is available to all residents of Brazil, including foreign-born individuals. The Sistema Único de Saúde (Unified Health System), established in 1988, ensures provision of primary and specialty care, emergency care, public health services, and medications. Healthcare is administered through the states, which apply for federal funding based on their need. Venezuelan immigrants must obtain a national health card (Cartão do SUS) to access services. Those with residency or refugee status are eligible, but key informants reported that Venezuelans sometimes faced challenges obtaining the card due to language barriers and discrimination. Venezuelans in Brazil have significant health needs on arrival, due to poor food security and nutrition in Venezuela and a high prevalence of chronic medical conditions.
Basic healthcare is also provided as part of the Welcome Operation, a collaboration between the Brazilian government, more than 20 nongovernmental organizations (NGOs), and five UN agencies to manage the migratory movement (Casa Civil 2018). Brazil’s armed forces have deployed 10 physicians in Bôa Vista to provide care to Venezuelans, in addition to two nurses, a pharmacist, and five public health officials. The healthcare teams visit each shelter two to three times a week and provide basic care. The most common conditions treated include diarrheal illnesses, intestinal parasites, respiratory infections, skin infections, and malnutrition. In addition, six physicians (three civilian and three military) have been deployed to the border town of Pacaraima, where they staff a screening and vaccination post at the immigration point of entry; 4,455 Venezuelans (26.8 percent children) have received services at this site since March 2018. Beginning in April 2018, all Venezuelans who apply for asylum or residency in Pacaraima (but not in Bôa Vista) receive the measles-mumps-rubella (MMR); tetanus, diphtheria, and pertussis (Tdap); and yellow fever vaccines unless they refuse or produce documentation of adequate vaccination. In addition, a military-style healthcare facility was inaugurated in Pacaraima in June 2018 with private rooms for clinical examination and phlebotomy, a pharmacy stocked with commonly used medications, and a room with hospital beds for observation and capacity for simple procedures (e.g., intravenous fluid resuscitation, nebulizations, first aid, and electrocardiogram [EKG]). Rapid tests are available for common infections, including malaria, HIV, syphilis, hepatitis C, dengue, chikungunya, and Zika.
The largest hospital in the state, Hospital General Roraima, has 306 beds and is located in Bôa Vista. During the first half of 2018, admissions of Venezuelan patients increased by 253 percent compared to the first half of 2017, and urgent and emergency room visits by 366 percent (Figure 3b) (Hospital General Roraima 2018). Similar to Colombia, the strain on the system was evident. Hospital administrators reported significant challenges in projecting budgetary needs and logistics in the context of the Venezuelan migrant flow. At the time of our visit, the Roraima General Hospital was facing shortages in antibiotics, syringes, and EKG leads. The director of Pacaraima Hospital, a smaller hospital at the border, reported that 70 percent of patients were Venezuelan and that the hospital also was facing antibiotic shortages (amoxicillin, azithromycin, furosemide, and omeprazole). Hospital staff indicated that the system was stressed not only by the increased number of patients but also by the severity of illnesses at presentation. For example, more than half the patients admitted to the oncology ward in Roraima General Hospital were Venezuelans with metastatic malignancies, many without option for cure. Venezuelans had longer hospitalizations than Brazilian patients, not only because of the severity of disease but also because of their precarious living conditions, which made discharge from hospital difficult.
Discussion
More than 1 million Venezuelans were residing in Colombia in early 2019, a dramatic increase from 2017, and most were in need of humanitarian assistance (USAID 2018). Although Venezuelan migration to Brazil is much lower, it is complicated by geographic isolation at the border, which creates a bottleneck in a poor and remote region of the country. We found that the scale of Venezuelan arrivals had overwhelmed local response capacities, particularly in border states where the migrant population was concentrated, and the humanitarian response was limited. The healthcare system is particularly strained in both countries. Migrants in Colombia do not have universal access to primary care, but the scale of migration has overwhelmed facilities providing urgent and emergency care. A large measles outbreak and rising malaria rates in Brazil have placed significant stress on the public health system.
Lack of availability of medicines and medical treatment has been reported on a widespread basis in Venezuela (Fraser and Willer 2016; Bello et al. 2017; Tran 2017; Umer 2017; Amnesty International 2018), and consensus among key informants was that access to health, economic opportunity, and food security were the primary drivers of migration out of Venezuela. Recent estimates suggest that more than 900,000 Venezuelans in Colombia need health assistance (USAID 2018). These needs, however, remain largely unmet. A 2018 assessment by the International Rescue Committee (IRC) reported 60 percent of respondents faced barriers to accessing healthcare in Colombia, and, other than food, the greatest unmet need was for medicines (71 percent) (IRC 2018). In North Santander, we observed that health facilities were overburdened by the increased number of patients from Venezuela in terms of lack of funds, materials, and human resources. The inability of the Colombian government to assume the cost of providing free non-emergency care to Venezuelans has had negative consequences for Venezuelans who cannot afford medical care, but also for the Colombian population in terms of the spread of infectious diseases. Furthermore, certain medications are either unavailable or too expensive for Venezuelans to purchase; this may exacerbate both infectious and non-infectious diseases. Besides poor patient outcomes, emergency care is expensive compared to preventative and primary healthcare, because emergency care is generally provided when diseases become more serious. Funding free non-emergency care for Venezuelans is controversial, however, because this is not universally available for Colombians. In addition, it could become a pull factor, leading to greater migration from Venezuela. There are, however, no obvious sources of funding to cover the costs of expanding free or subsidized health services for Venezuelans in Colombia.
Although the Brazilian Constitution guarantees access to healthcare for migrants, increasing demand on the healthcare system threatens to compromise services for everyone. The influx of Venezuelans, who have had little or no access to care and medications at home, has resulted in a pent-up demand for care, especially among patients with chronic and severe conditions that were previously unattended and that are complicated by malnutrition and social factors such as housing instability. As a result, the largest tertiary hospital in Roraima is facing unprecedented shortages because the number of patients more than doubled in a year. Although basic healthcare provided at the shelters is helping to decompress the system, additional personnel, medications, and supplies are needed at health facilities. As the flow of Venezuelans entering Brazil increases and the healthcare system reaches a saturation point, the need for technical assistance and monetary support from the federal government and international community will become more urgent.
Failures of the public health system in Venezuela also threaten transnational health in the region. Vaccine shortages have led to a resurgence of measles and diphtheria in Venezuela (PAHO/WHO 2018a, 2019; Page et al. 2019; Torres and Castro 2019). There have been a few cases of imported diphtheria in Colombia and none in Brazil, but there is an ongoing and rapidly expanding measles outbreak in Brazil. In response, the Colombian and Brazilian governments are providing free vaccinations in border areas, and strengthening epidemiologic surveillance. Brazil also provides universal access to healthcare, including non-emergent care, regardless of immigration status. In Colombia, migrants have access to free emergency care in government health facilities, but access to non-emergency health services (i.e., primary, secondary, and tertiary care) is not available to most Venezuelans (Colombian MoH 2017). Brazil has also conducted large vaccination campaigns in Roraima and Amazonas, where the measles outbreak has highlighted low vaccination rates, especially among Venezuelans and indigenous populations. In addition, the interruption of vector-control activities and the propagation of illegal mining activities in Venezuela, where standing water from mining operations promotes mosquito breeding (Daniels 2018; Tuite et al. 2018; Grillet et al. 2019), have contributed to a dramatic rise in malaria in Venezuela (PAHO/WHO 2018b; Grillet et al. 2019), particularly in the state of Bolívar, which borders Roraima, where malaria rates have also soared. The Venezuelan crisis threatens to set back years of progress in malaria and measles control in Latin America.
Our programmatic assessment had several limitations. Key informant interviews were not audio recorded or systematically coded, making it possible that not all information relayed by key informants was adequately captured. In addition, health statistics provided by hospitals and public health entities at each country were obtained using different methodologies, limiting our ability to make direct comparisons of each dataset. Although public health surveillance data are more likely to capture reportable health outcomes (as compared to hospital data), limited access to healthcare among migrants may lead to underestimation of the true burden of disease. In addition, incident rates cannot be calculated without accurate denominators. In the case of Colombia, the burden of the migration crisis is more likely to be underestimated because Colombian returnees, many of whom face similar challenges as Venezuelan migrants, are not included in the analysis. Because most data are reported by nationality, it is impossible to distinguish returnees from other Colombians. Despite these limitations, the data show the strain on the healthcare systems in receiving countries and concerning increases in infectious diseases that have transnational public health implications.
The international humanitarian response to the Venezuela crisis has been limited thus far. In Colombia, the majority of health costs for Venezuelan migrants are borne by the Colombian government. The growth of arrivals in 2017 and 2018 triggered an increased response from UN agencies and bilateral donors. Appeals to date are not fully funded, however, and relatively minimal funding is dedicated to the health sector response (Table 2). In Brazil, the federal government, in collaboration with NGOs and UN agencies, has established 12 migrant shelters in the area (at a cost of US$47 million), and allocated an additional US$56 million to cover social and health services in Roraima (Casa Civil 2018). Despite these efforts, many challenges pose a risk to migrant and transnational public health. Many Venezuelans in both Colombia and Brazil remain homeless and live in precarious tent encampments, vulnerable to hygiene-related diseases and crime. Employment opportunities are scarce, and xenophobia is on the rise.
Response to the Venezuelan Migrant Crisis: Roles and Funding Commitments.
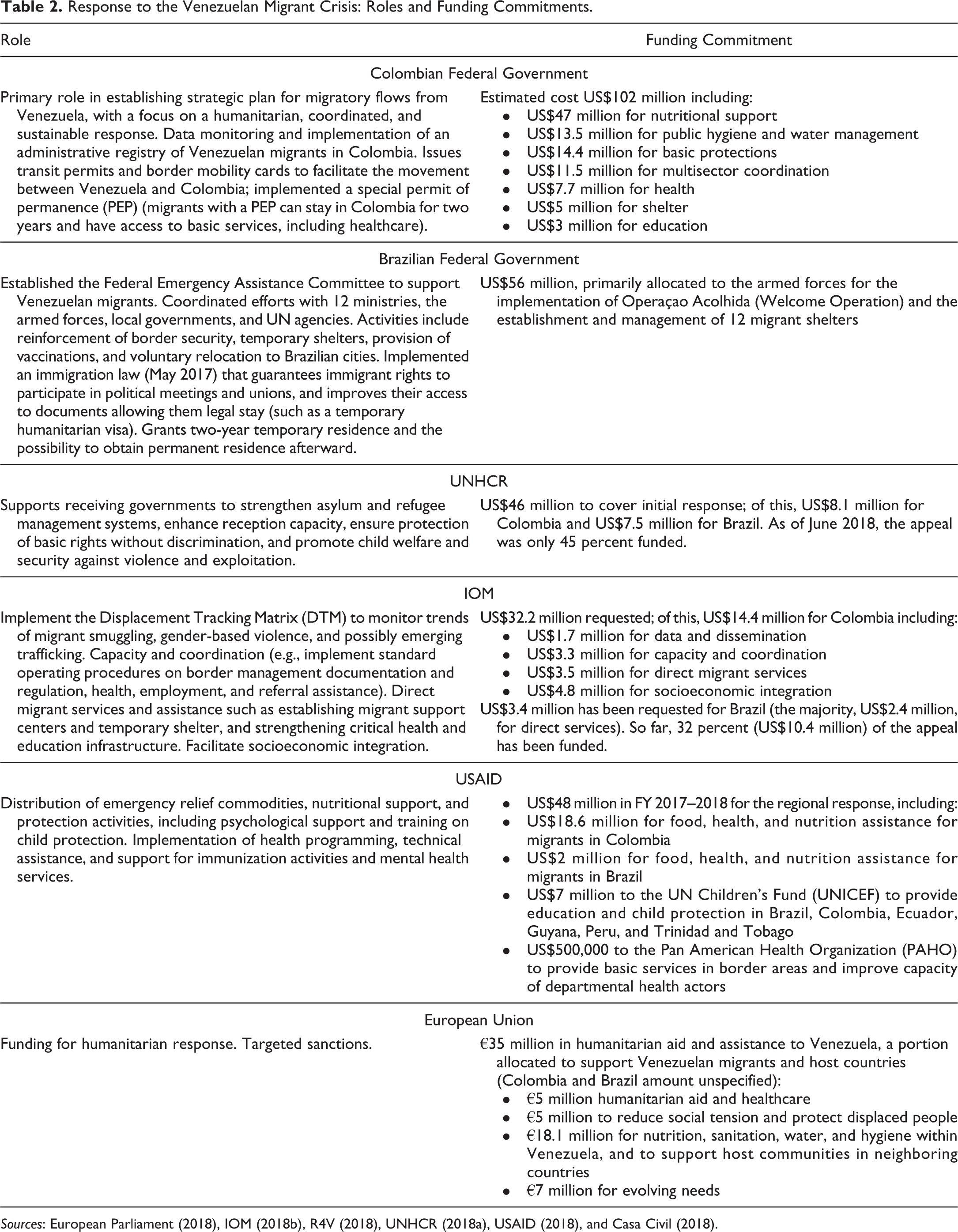
Sources: European Parliament (2018), IOM (2018b), R4V (2018), UNHCR (2018a), USAID (2018), and Casa Civil (2018).
While the Colombian and Brazilian government responses to the immediate needs of Venezuelans have been admirable, they are not sustainable. There is an urgent need for an expanded humanitarian response to the Venezuelan migrant crisis in the region, particularly to address health needs, for which surveillance data show recent and rapid rises in infectious diseases, acute malnutrition, and poor maternal and neonatal health outcomes. Lack of access to preventative and primary care and inadequate funding of life-saving emergency care portend a health crisis for Venezuelans in Colombia, which has the potential to affect public health more broadly if not addressed through a more comprehensive and adequately funded humanitarian response. In Brazil, there is a need to invest in integration programs to improve the health and well-being of Venezuelans who have fled their country, with sensitivity to the needs of receiving communities, especially those who are underserved, to minimize resentment among the local population. This complex and costly process will require political will and financial support from other neighboring countries and the international community at large. In the longer term, only a resolution of the complex health and humanitarian crisis within Venezuela itself will address these transnational threats to health in the region.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received the following financial support for the research, authorship, and/or publication of this article: This work was made possible by the generous support of the Desmond Tutu Professorship in Public Health and Human Rights at the Johns Hopkins Bloomberg School of Public Health, and Human Rights Watch.