
Abstract
Executive Summary
This article explores how undocumented border crosser (UBC) deaths are counted as well as mis- and under-counted across the US southwest, and proposes a suite of policy remediations to standardize this process. An accurate count of UBC recovered remains is vital to understanding the scope of fatalities associated with border crossing, providing evidence accounting for the reciprocal relationship between US border enforcement and the incidence of migration-related death. To meaningfully intervene, it is insufficient to advocate only for more robust individual death investigations, though this is pivotal to forensically identify UBC decedents and unite them with their loved ones. Though identification and reunification of UBCs are the elements of forensic care most commonly attributed as humanitarian, the relationship between forensic investigation and international humanitarian principles is equally about accumulating primary evidence for policy intervention and justice claims on behalf of those who wrongfully die. Even if existing counting mechanisms do not provide the means for establishing this attribution between border-crossing deaths and border enforcement policy, this article lays out an argument for why they must do so and it makes recommendations for how this can take place.
Necessarily, this article begins with a critique of existing mechanisms for counting UBC deaths, from the federal observation of such deaths by Customs and Border Protection, to the bureaucratic mechanisms for the collection of vital statistics authored at the local level. It then suggests means for improving accurate counting using the US Standard Certificate of Death. It particularly explores two aspects of the certificate, Manner of Death reporting and a section that asks death filers to describe how the death occurred, sections 37 and 43 respectively. Finally, it explores historical precedent for altering the standard death form at local and then national levels, positing that select amendments to the existing death certificate would be useful for standardizing how medicolegal death filers across the border and beyond can more accurately enumerate and characterize UBC deaths.
Policy recommendations include the following, in order of immediacy:
● Jurisdictions across the US southwest must adopt standardized criteria for counting fatalities believed to be associated with undocumented border crossing.
● Despite some local formalization of UBC counting, current means of representing UBC status in vital records remains ad hoc across the US southwest and existing mechanisms for counting elude wider scale national recognition in vital statistics. The most straightforward and reliable method of standardization to ensure systematic representation of UBC deaths across the borderlands would be a UBC checkbox on the death certificate. This would require cooperation with state-level public health departments and legislatures. Precedent exists for changing the death form at the state level, facilitating, in some cases, for eventual inclusion of new components of the death certificate to be adopted on the US Standard Certificate of Death. This is recommended as a longer-term goal.
● Finally, there must be a means to characterize the deadly relationship between UBC fatalities and US border enforcement policy and practice in vital records where UBC Manners of Death are most often characterized as “Natural” or “Accidental.” Both are inaccurate. Unilaterally ensuring an accurate count leaves room for a trend already well underway in which agencies associated with border enforcement have cast UBC deaths as simply due to unfortunate heat-related accidents, resulting in legislation aimed to mitigate deaths that fails to address the role of border policy in causing deaths. This paper recommends that a new Manner of Death category could be useful beyond the border to represent non-capital crimes enforced by leveraging bodily harm.
Introduction
This article explores how undocumented border crosser (UBC) deaths are counted as well as mis- and under-counted across the US southwest, proposing a suite of policy remediations to standardize this process. An accurate count of UBC recovered remains is vital to understanding the scope of fatalities associated with border crossing, providing evidence accounting for the reciprocal relationship between US border enforcement and the incidence of migration-related death. To meaningfully intervene, it is insufficient to advocate only for more robust individual death investigations, though this is pivotal to forensically identify UBC decedents and unite them with their loved ones. Though identification and reunification of UBCs are the elements of forensic care most commonly attributed as humanitarian (e.g., Moon 2020), the relationship between forensic investigation and international humanitarian principles is equally about accumulating primary evidence for policy intervention and justice claims on behalf of those who wrongfully die (e.g., United Nations 2017). Even if existing counting mechanisms do not provide the means for establishing this attribution between border-crossing deaths and border enforcement policy, this article lays out an argument for why they must and makes recommendations for how this can take place.
Necessarily, this article begins with a critique of existing mechanisms for counting UBC deaths, from the federal observation of such deaths by Customs and Border Protection (CBP) to the bureaucratic mechanisms for the collection of vital statistics authored at the local level. It then suggests means for improving accurate counting using the US Standard Certificate of Death. It particularly explores two aspects of the certificate, both Manner of Death reporting and a section that asks death filers to describe how the death occurred, sections 37 and 43 respectively. Finally, it explores historical precedent for altering the standard death form at local and then national levels, positing that select amendments to the existing death certificate would be useful for standardizing how medicolegal death filers across the border and beyond can more accurately enumerate and characterize UBC deaths.
Counting UBC Deaths: An Overview of the Status Quo
Papers throughout this edited collection describe the relationship between UBC deaths across the US southwest and policies for enforcing US borders. Most overtly, the strategy of “prevention through deterrence” adopted for the whole of the US southwest from 1994 described an intended relationship between “hostile terrain” and “mortal danger.” The Border Patrol’s (BP) 1994 Strategic Plan document explained that a calculated deployment of infrastructure and personnel would block what were historically safer zones of urban transit to ensure that remaining alternate routes would be more dangerous to undocumented travelers, with the capacity to exact a deterrent “cost” on UBC bodies (USBP 1994, 6–7): “The prediction is that with traditional entry and smuggling routes disrupted, illegal traffic will be deterred, or forced over more hostile terrain, less suited for crossing and more suited for enforcement [. . .] [The goal is] to increase the ‘cost’ to illegal entrants to the point of deterring repeated attempts” (ibid., 6–7).
As this strategy came to deadly fruition in the years to follow, researchers have understood this planning document as an announcement of a policy intent to use the risk of suffering and mortal danger as leverage to deter undocumented journeys. In the early 2000s, this began in Pima County in southern Arizona as personnel from the medical examiner’s office noticed a dramatic increase in excess deaths due to heat-related causes and in wilderness settings (Keim et al. 2006; Rubio-Goldsmith et al. 2006). This occurred in tandem with surges of BP apprehensions of undocumented migrants in the same areas. The association of these deaths to undocumented border crossings paved the way for a wide body of scholarship attributing the rise of prevention through deterrence and a funneling effect of UBCs into increasingly remote and rugged areas to cross the border and evade detection (e.g., Eschbach et al. 2001; Cornelius 2005; Rubio-Goldsmith et al. 2006; Kovic 2013; De León 2015; Boyce et al. 2019; Boyce and Chambers 2021; Martínez et al. 2021; Chambers et al. 2019, 2022).
A sustained observation of UBC deaths prompted the Pima County Office of the Medical Examiner (PCOME) to establish a UBC criteria to capture what was understood as an emerging public health crisis of correlated deaths (Anderson and Parks 2008; Keim et al. 2006). The office now documents when decedents under their care are probable UBCs on a supplemental form filed with these individuals’ vital records (Binational Migration Institute 2014).
PCOME’s systematic documentation effort facilitated for researchers and local humanitarian organizations to work with the office as they sought to understand what was happening (personal communication, June 11, 2021). 1 Among many public products of this relationship, PCOME’s criteria for identifying and counting probable UBCs was publicly circulated to establish the legitimacy and rigor of the office’s death counts (Rubio-Goldsmith et al. 2006). As of 2014, this included the following, for which multiple corresponding indicators were used as conditions to identify probable UBCs for enumeration:
The decedent lacks a US Social Security Number, permanent US residency card, or evidence of lawful US immigration status.
The decedent is of Hispanic ethnicity.
The decedent is foreign-born, of a foreign nationality, foreign residency, foreign next-of-kin, and died while in transit from Mexico to a US destination.
The body was discovered in a well-known migration corridor, or
Was found with or reported by other UBCs.
The decedent possessed personal effects or documents typical of UBCs, water jugs, extra clothing, addresses of contacts in a foreign country, US and foreign currency, phone cards, hygiene products, phone numbers, a backpack. (quoted in BMI 2014, 4)
The forensic anthropologist at PCOME, Bruce Anderson, described
our office practice [. . .] to include anyone who fits [this] pre-established profile that indicates that the decedent was engaged in the undocumented crossing of our southern border. This practice acknowledges that we may be slightly over-reporting the number of border-crossing deaths. Our office considers this potential issue preferable to the vast under-reporting that would result if these unidentified individuals were excluded from the rolls of the unsuccessful migrants. (Anderson 2008, 12)
As their criteria developed, PCOME made efforts to foster cooperative relationships with other border jurisdictions in California and Texas to establish border-wide standards for counting UBC deaths (Anderson and Parks 2008). But as of 2024, counting UBC deaths beyond Pima County takes place on a mostly ad hoc basis in other jurisdictions, even as the deadly funneling effect of migration related to prevention through deterrence shifted or distributed regionally across the US southwest over the years since the strategy’s adoption (Cornelius 2005; Kovic 2013; Leutert et al. 2020; No More Deaths 2024).
For instance, over multiple interviews, the Webb County medical examiner in Laredo, Texas reported enumerating UBC deaths investigated by her office by maintaining an internal log listing individuals she believed to have died under these circumstances (personal communication, January 9, 2023). She explained that her office mainly assigned a UBC status based on a decedent’s clothing and discovery in known migration corridors (personal communication, March 2, 2012), 2 though this criteria was not formalized. She also documented such deaths on the component of the death certificate—section 43—asking filers to describe how the death occurred. She told me that she would always add a note identifying the person as an undocumented migrant and that doing this was “humanitarian” given her awareness that the state of Texas does not compile death statistics related to border crossing (personal communication, January 9, 2023). Webb County’s medical examiner office, like Pima’s, has served multiple counties in its proximity in southeast Texas.
In Brooks County in Texas, the current sheriff—then a deputy—described knowing border crossers on sight: “We do this so often that I just know” (personal communication, February 28, 2012). The county’s criteria for tallying UBC deaths are mainly based on this accumulated experiential knowledge and affirmed based on geography—those who died on private ranchland without any local knowledge of their identities are understood as probable UBCs. More than 90 percent of that county is private ranchland and sheriff’s office personnel reason that non-local people have no other compelling reason to trespass (field notes, September 6, 2023). The same rationale was described in Webb County (personal communication, March 2, 2012). Some of Brooks County’s justices of the peace, their principal medicolegal authority, add a similar note in the “describe how injury occurred” section on death certificates for suspected UBCs as that described by the medical examiner in Webb. I reviewed sheriff’s office incident reports as well as inquest records from one justice of the peace dating from 2019 and 2022 for all individuals in those years identified as probable UBCs in Brooks. Among these records, a description I saw repeated on available abstracts of deaths (short form versions of death certificates) was, “decedent was hiking through ranch illegally.” Internally, the county maintains binders organized by year aggregating all sheriff’s incident reports associated with the recovery of individuals they believe to be UBCs.
Other Texas jurisdictions make no record of individuals whose deaths they believe to be associated with migration, even though many county officials have described informally recognizing probable UBCs based on some of the common traits in the criteria established by PCOME (Soto 2020a). One Texas sheriff insisted that since migration violations are a federal crime, it is simply not his county’s job to make any note of a person’s migration status in their documentation of the death (personal communication, August 8, 2012). El Paso County’s medical examiner explained to reporters in 2023 that “our office does not track migrant deaths, nor is data collected when a consulate is involved” (Villagran 2023). However, a BP El Paso Sector spokeswoman confirmed that despite the county not officially tracking UBC deaths, the El Paso County Office of the Medical Examiner regularly provides the agency with lists of deceased individuals suspected to be UBCs (Ibid.). This indicates that the medical examiner’s office has some informal criteria established for recognizing characteristics they associate with this population, and is also recording them in some way—despite statements to the contrary.
Because most jurisdictions in Texas do not count UBC deaths in any official way, when researchers from the University of Texas Austin’s Strauss Center attempted to compile southeast Texas UBC death records for analysis they were left to create inclusion criteria based on information they could glean from sheriffs’ incidents reports and justice of the peace inquest records (Leutert et al. 2020).
The most fundamental challenge for this report’s dataset was determining who fit into the target population: unauthorized migrants in transit through South Texas. While some deaths appeared to be a clear fit, others did not. To ensure that non-migrants were not included in the count, the researchers designed a four-pronged approach to answering this question: (1) a decedent had to be found along known migration routes; (2) the place of birth and residency was not in the United States; (3) the decedent had to lack a U.S. social security number on their death certificate; and (4) the decedent’s cause of death had to be consistent with transit migration and uncommon for individuals not in transit (such as dehydration, heat stroke, or hypothermia). For unidentified remains, the researchers relied more heavily on meeting the first and fourth criteria. (Ibid., 11)
The Strauss Center research team acknowledged that lacking context for many deaths meant they were likely undercounting incidents that did not conform with common causes of death for UBCs in transit. Further, with knowledge that many Texas counties are not conducting thorough medicolegal investigations for deaths inferred to be migration-related, many cause of death listings that the research team associated with migration were based on assumptions local officials made about how UBCs died absent forensic confirmation (Frey 2015; Gocha et al. 2018; Soto 2022; Chesky and Lozano 2024).
For example, as I conducted ethnographic fieldwork in Brooks County between 2019 and 2023 I learned that Brooks County ended its contract with the Webb County Office of the Medical Examiner (WCOME) in 2021 to perform autopsies for UBC individuals. This means that most individuals believed to be UBCs now do not receive any forensic examination beyond efforts to identify them—where the forensic identification process is the sole and concerted focus. 3 In these conditions, the county’s medicolegal officials instead list causes of death for probable UBCs based on visual estimation in correlation with their knowledge of historic trends associated with UBC deaths. They reason that the vast majority of autopsies performed in prior years—autopsies being scientific determinations of cause of death—listed UBC causes of death overwhelmingly due to dehydration or hyperthermia, or in extreme cold spells, hypothermia. They currently list UBC causes of death accordingly in vital records. In Pima County, by contrast, identifying cause of death for UBCs is premised on thorough forensic investigations (Rubio Goldsmith et al. 2006; Anderson 2008; Reineke 2016). Identifying an individual as a UBC is not to identify how that person died, though this appears to be a common trajectory (Soto 2020a).
It bears acknowledging that jurisdictions outside Pima County have different resources for investigations and may observe UBC deaths occurring in different ways—including the rise of drownings and wall fall deaths that often occur in hospitals as opposed to wilderness settings in the BP El Paso Sector (No More Deaths 2024). Some recent reporting indicates that UBC deaths may also be occurring in greater numbers along the US border with Canada where the BP also recorded a 1,000 percent surge in apprehensions from 2021 to 2024 (Robinson 2024). It is not clear from reporting how these individuals die, but it seems they are mainly due to cold exposure (Staff 2022; Bilefsky 2023). While Pima County’s criteria for identifying UBCs may not apply universally, and indeed bear some updating as migration trends evolve and include more UBCs from outside Latin America, they are formalized in distinction from most other medicolegal jurisdictions in the US southwest—or for that matter, the northern border.
Significantly, observing PCOME’s established investigation-based standards for counting UBC deaths has allowed researchers and investigative journalists to compare their numbers to those aggregated by CBP under which BP operates—the only entity providing an official count of UBC deaths in the United States across all border jurisdictions.
The fact that CBP is responsible for counting UBC deaths is highly concerning, placing the parent entity of the agency whose enforcement practices researchers argue are responsible for surges in UBC deaths in the position of monitoring these deaths. These casualties should be an indictment of agency practices, and so CBP is in the position of essentially providing oversight for itself. But their authority for counting the dead is also problematic in a practical sense as neither CBP nor BP has jurisdiction or capacity for investigating UBC deaths. Investigations and filing of vital records are the mandate of local medicolegal authorities. Jurisdiction shifts upon the death of a UBC, from a federal concern while the person was alive to a local one when the person dies (Soto 2022). Strikingly, in some sectors in Texas, BP agents had once adhered to negotiated union contracts that prohibited them from touching a deceased person, even a presumed UBC, even when they were on scene when remains were recovered and could have assisted local investigators in the recovery (Ibid.).
When researchers from the Binational Migration Institute (BMI) published their first analysis of PCOME’s UBC records in 2006, they observed in comparison that CBP counted such deaths using a narrower set of criteria than PCOME.
CBP’s criteria include the following:
The death occurs during the furtherance of an illegal entry.
The death occurs within the Border Safety Initiative (BSI) “target zone” (which includes 45 counties on or near the US/Mexico border or 9 of the 20 BP sectors).
The death occurred outside of the BSI “target zone,” but the BP was directly involved in the case. (quoted in Rubio Goldsmith et al. 2006, 11).
BMI’s report documented a subsequent undercounting by CBP compared to PCOME in the region of the Tucson Sector of BP operations—a trend that appears to have continued and expanded more recently in Pima County and beyond (O’Dell et al. 2017; Ortega 2018; Leutert et al. 2020; Martínez et al. 2021; Leutert 2024; No More Deaths 2024). PCOME also occupies a smaller area than that of the Tucson Sector, though it fits within its borders. This makes CBP’s undercounting even more striking, observing deaths across a wider geographic area (Rubio-Goldsmith et al. 2006).
Since BP does not have jurisdiction to investigate deaths, it seems that the principal discrepancy in CBP’s counting occurred when local authorities investigated a death without BP present—because BP does not necessarily have any investigative reason to be present. Often agents discover remains because they patrol the remote regions where deaths occur, or otherwise they might be called when someone else finds remains believed to be associated with undocumented migration (BMI 2014; Soto 2022). Other discrepancies seemed to be due to bureaucratic oversight, or deaths that occurred in hospitals north of the “target zone” even when an injury and subsequent medical evacuation occurred in a Border Safety Initiative “target zone” (Rubio Goldsmith et al. 2006; O’Dell et al. 2017; Ortega 2018; Leutert 2024; NMD 2024)
When the Missing Persons and Unidentified Remains Act (MPURA 2020) was passed into federal law in 2020, it required CBP to interface with local jurisdictions to fill in the gaps of their acknowledged undercounting of recovered UBC deaths. It also required CBP to explain in its reporting the limitations of its dataset. After failing to meet the requirement by MPURA’s established deadline for over 3 years, CBP finally began listing deaths documented by its own agents as well as additional numbers recorded by local authorities. These appear on their website as simply a disaggregation based on “discoverer” in CBP records—distinguished between “USBP” and “Other” (US CBP 2023).
However, as of this writing, CBP has still failed to provide any official accounting of its dataset’s limitations or to explain how the local numbers were received (US GAO 2022a, 2022b, 2024a). Places like Webb and Pima Counties were cited in a Government Accountability Office (GAO) investigation of CBP’s undercounting post MPURA as consistently providing their local data to the agency (US GAO 2022b). Brooks County consistently provides these numbers as well (field notes, September 6, 2023). Despite coordinating with many local entities as required, the GAO found that CBP was still not reliably including counts beyond its own agency observations in its enumeration of UBC fatalities (US GAO 2022a, 2024a).
Several dubious explanations were offered to GAO investigators for this discrepancy, including issues of coordinating bureaucratically across multiple sectors where local agents were not consistently aware of their obligation to update numbers based on local medicolegal data (US GAO 2022b, 7–8; US GAO 2024a, 4). The most compelling explanation offered was that CBP could not consistently verify whether local counts of UBC deaths conformed with its own agency criteria for inclusion of “reportable migrant death[s]” (US GAO 2022b, 9; US GAO 2024a, 6). This makes some sense in light of the fact that most local jurisdictions in the US southwest may not disaggregate believed UBCs from other deaths recorded locally, and lack formal criteria for doing so.
It also makes sense in light of counting criteria in Brooks County. Brooks’ criteria may be locally reasonable, but are not easily articulable with CBP’s. However, after several years and an established working relationship with local reporting jurisdictions like Brooks County, CBP’s explanation still begs credibility in the sense that the agency could have notified cooperating local officials of its criteria and asked them to provide information accordingly (cf. Leutert 2024). Yet, the GAO investigation also found that CBP continues to undercount deaths reported by PCOME, which both regularly communicates with the agency and has a clearly defined and public standard for inclusion of UBC cases that overlaps with CBP’s, albeit not directly (US GAO 2022b, 8).
Despite many issues with relying on CBP to monitor border-crossing deaths, CBP’s explanations for its undercounting of local deaths since MPURA should revive efforts by local jurisdictions to standardize how they count UBC deaths. Yet ideally, local jurisdictions should not rely on CBP to monitor UBC deaths at all. Standardizing how UBC deaths are counted in jurisdictions directly responsible for investigating and identifying locally occurring deaths, including those of UBCs, should be a means to scrutinize what is happening when trends appear among how people die—in this case, the trend in UBC deaths represents the deadly results of border security practice. Rigorous and standardized accounting can create a forensic record to hold government agencies responsible for utilizing border enforcement practices that leverage suffering and possible death as deterrence mechanisms.
The status quo presents many roadblocks to standardizing accounting of UBC deaths, as discussed above. However, local jurisdictions that investigate cases of UBC fatalities should count this population. Inclusion in this accounting should be based on a set of agreed upon criteria that overlaps with CBP’s standards for identifying UBC deaths. A longer-term remedy that bypasses reliance on CBP is also urgent. One reliable solution can be found in the death certificate as all local medicolegal officials are responsible and obligated to these vital records. Because death certificates constitute a national and international database of vital statistics accounting for how people die, coordinating and standardizing filing of death certificates observing UBC deaths may provide the best path forward for monitoring these deaths in the border region and beyond.
Considering the death certificate as a solution also necessitates that I review how national vital statistics are collected, as well as collection limitations. In the following sections, I argue that possible pathways for standardizing accounting of UBC deaths in US vital records build on precedent and can also provide means to recognize other deaths resulting from preventable social violence.
The Dead Must be Counted: Limitations and Paths Forward
Why is accurately counting the dead a task for the government? In the United States, the web page for the National Vital Statistics System (NVSS)—operating under the Center for Disease Control and Prevention (CDC)—characterizes its purpose as follows: “National level mortality data help track the characteristics of those who have died, monitor and make decisions about public health challenges, determine life expectancy, and compare death trends with other countries” (NVSS 2022). Death statistics generated through this system are thus legible as policy concerns that can be remediated through political action, regulatory policy, research, and funding. In tracking deaths, NVSS aggregates statistics assembled based on death certificates generated for all people who die in the United States, 4 regardless of their citizenship. The United States also shares its vital statistics with the World Health Organization to facilitate tracking and policy making at a global scale (Schulz 2014). NVSS is thus a critical tool facilitating the US government’s role in protecting public health.
And yet, the fact that NVSS does not include statistics on death trends as prominent as those of UBCs on the border illustrates how established modes of counting the dead fall short. In 2017, Pima County’s chief medical examiner, Gregory Hess, said as much to reporters from USA Today in defense of his office’s efforts to enumerate UBC fatalities: “A hallmark of civilized society is that [. . .] you keep track of [. . .] death statistics [. . .] with the intent to decrease those deaths or take policy measures to help whatever the issue is” (quoted in O’Dell et al. 2017). Hess noted this with a tone of frustration, quoted in an article with a title that captures the concern: “‘Mass disaster’ at the border, little care in Washington, D.C.” Tracking UBC deaths through NVSS could provide the mechanism to achieve the kind of policy remediation Hess proposed, but it currently does not. In fact, the CDC generates periodic reports on mortality trends gleaned from NVSS, some of which align with common causes of death observed among UBCs, like deaths from heat exposure. However, this mortality reporting only observes deaths of US citizens in its population of concern, though including UBC deaths on US soil could have increased the CDC’s observed annual averages of deaths from heat exposure by at least 50 percent (Leutert et al. 2020; Martínez et al. 2021; NMD 2024). It is then necessary to understand why these gaps in NVSS’s tracking exist, because closing them would be the most straightforward means to ensure standardized and reliable accounting of UBC deaths in the US southwest and beyond.
Over the years, many criticisms have been levied against the limitations of vital records collection in the United States (Carter 1985; McGinnis and Foege 1993; Wexelman et al. 2013). As it did with so many other facets of our social and political lives, the COVID-19 pandemic brought many long-existing shortcomings in US death tracking to light. Increased rates of excess deaths that were likely, but not clearly attributed to COVID, raised awareness about the lapses in death recording for the many cases where there seemed to be no medicolegal capacity for follow-up among deaths that occurred outside of medical observation. The CDC’s guidance for listing COVID-19 deaths in vital records acknowledged this: “Getting high quality cause-of-death information can be challenging, especially during emergencies. Certifiers may be faced with heavy workloads, may not have access to complete information about the death, or may not be well-trained in how to prepare quality cause-of-death statements” (CDC 2021). This is a limitation echoed by conditions in the US southwest where high volumes of UBC fatalities in excess of expected local death rates have challenged existing medicolegal infrastructure and left many cases un- or under-investigated (Reineke 2016; Gocha et al. 2018; Kaplan and Spradley 2022; Chesky and Lozano 2024).
Investigative reporting found that “[a]fter overwhelming the nation’s health care system, the coronavirus evaded its antiquated, decentralized system of investigating and recording deaths” (The Documenting COVID-19 project, and USA TODAY Network 2021). The investigation’s authors contested the CDC’s claim that it was only the public health emergency that stood in the way of quality death recording, arguing that the pandemic exposed a pre-existing crisis in national vital records. For instance, the majority of medicolegal officials across the country who both file death forms and determine how suspicious or unattended deaths are investigated may lack any required medical background or training beyond on-boarding for their positions (Berard 2009a; NAS 2009; Young 2022). While medical examiners are medical doctors, usually with a required specialty and certification in forensic pathology (though certification is not required in states like Texas), medicolegal authorities like coroners and justices of the peace in Texas do not consistently possess this education and are not consistently required to (Berard 2009a; NAS 2009; BMI 2014). Given that there are only 14 public medical examiner’s offices across Texas, investigative reporting has found that they—like many forensic pathologists across the United States—experience chronic case overloads, often taking on over 300 percent of recommended annual case maximums (Berard 2009a; NAS 2009; Tracey 2023). This means that they experience sustained emergency-level caseloads, exacerbated in border jurisdictions by excess deaths that occur when UBCs are funneled there.
Research also points to a long history of officials filing specious death records deliberately misidentifying causes that at different times attached to certain kinds of social stigma, especially the incidence of deaths related to drug and alcohol addiction, or that otherwise proved politically inconvenient to come to light—such as deaths at the hands of police (Berard 2009b; The Documenting COVID-19 project, and USA TODAY Network 2021; GBD 2021; Young 2022).
Since the murders of Michael Brown in 2014, then George Floyd in 2020, 5 greater awareness has emerged for lapses in tracking deaths directly due to social violence—especially gun violence and fatal police encounters (McGinnis and Foege 1993; The Counted 2016; Soto 2020b; Fatal Encounters 2024; Gun Violence Archive 2024). For example, when journalists from the Guardian began a project called, “The Counted” (2016), to track deaths at the hands of law enforcement in the United States, they wrote: “The US government has no comprehensive record of the number of people killed by law enforcement. This lack of basic data has been glaring amid the protests, riots and worldwide debate set in motion by the fatal police shooting of Michael Brown, an unarmed 18-year-old, in Ferguson, Missouri, in August 2014” (emphasis original). The George Floyd Justice in Policing Act attempted to legislate a mechanism to track all law enforcement use of deadly force in the United States, though it required the data be collected by law enforcement and not through vital records (George Floyd Justice in Policing Act 2021). If passed, this reporting requirement could fill a wide gap in existing data, but it has stalled in Congress for over 3 years at this time of this writing. As of June 2024, it remains true that the only federal counting of such deaths comes through a voluntary reporting system managed by the Federal Bureau of Investigation that tracks only “justifiable homicides” self-reported by local police jurisdictions. Only a fraction of police forces ever submit data (The Counted 2016).
In 2013, Congress passed the Death in Custody Reporting Act, mandating the US Department of Justice to regulate the recording of all deaths occurring during and after an arrest while subjects remain in custody. In the last several years, studies and Congressional hearings have brought to light how reporting lapses have continuously failed to count such incidents in violation of the law (The Leadership Conference Education Fund and POGO 2023). Similarly, in 2024 the GAO issued a review critiquing this very reporting failure by CBP to account for injuries and deaths among undocumented migrants experienced during encounters with its agents and in its custody (US GAO 2024b).
In these cases, the primary policy responses to lapses in reporting deaths resulting from encounters with law enforcement seems to be legislating mandates for law enforcement entities versus medicolegal death filers to faithfully account for the incidents that could call their own practices into question. As described above, MPURA seems to have created similar flawed expectations for CBP.
Death reporting guidelines offered by the National Association of Medical Examiners (NAME) emphasize a particular need for unbiased reporting accuracy by medicolegal authorities observing deaths related to encounters with law enforcement—necessary to uphold credibility and public trust in their own forensic authority, but also in law enforcement to faithfully manage public safety (Hanzlick et al. 2002, 11–12; Timmermans 2007). A close relationship between medicolegal authorities and law enforcement has been demonstrated to sometimes compromise medicolegal authorities’ ability to hold their colleagues accountable when deadly incidents occur (Young 2002; Timmermans 2007; Berard 2009b). In fact, 22 percent of medicolegal authorities who responded to a 2011 survey about tracking deaths at the hands of the police “reported having been pressured by an elected official or appointee to change cause or manner of death on a certificate” (GBD 2021, 1250)
A 2021 study published in the Lancet medical journal compared NVSS data to non-governmental databases independently tracking police violence through crowd-sourcing data. Using regression modeling, the researchers attempted to quantify the extent of NVSS’s undercounted deaths at the hands of the police between 1980 and 2019, estimating at least 17,000 more deaths in these circumstances than could be traced through NVSS. If accurate, this would mean half of all such incidents were uncounted in US vital records, with most incidents likely applying to people of color (Ibid.). The lapse seems to stem from the level of the death certificate, particularly listings of Manner of Death and components that ask filers to describe the context of fatal incidents.
There is considerable evidence that omission of police involvement from the description of how the injury occurred is responsible for the misclassification of police violence as homicides. A police violence death might be misclassified as another cause because the certifier fails to mention the police in the “describe how the injury occurred” section, or because the certificate is incorrectly coded after the fact. (Ibid., 1250)
Observing this problem, the study authors recommended better training for medicolegal death filers (Ibid., 1251), though this seems insufficient alone to resolve the issues. Alternatively, the California legislature passed a bill in 2022 requiring medicolegal authorities in the state to use the “describe how injury occurred” section of the death certificate (section 43) to explicitly note when a given death was in law enforcement custody and/or at the hands of a law enforcement official (Moscufo 2022). As of this writing, the results of this new requirement are yet to be seen, but it appears to be a stronger remediation than that offered by the Lancet authors.
In his ethnographic study of one medical examiner’s office, Stefan Timmermans (2007) theorized the implications of sustained undercounting of police-related fatalities for the public’s ability to fully comprehend what it means to support tough-on-crime politics. “Inevitably, when deaths that appear to be forensic homicides are not counted as such, one can question whether a reduction in crime has actually occurred” (Timmermans 2007, 192). Do tough-on-crime political measures simply create a perception of falling crime rates? If legally-tolerated homicides (deaths at the hands of police) are substituted for extra-legal homicides, then the aggregate violence might never have changed despite public perception to the contrary. This is a question with particular relevance for the border where preventable wilderness deaths of UBCs are not reliably recognized as results of border enforcement strategy.
Medicolegal capacity to inform public health should transcend the recognition of disease and apply to social causes—from deaths due to police violence to those resulting from undocumented border crossings. Through a wider historical lens beyond the border region, the ability of the medicolegal system to identify and record deaths associated with social causes has been central to establishing the capacity and legitimacy of forensic death investigation in the United States. Historically, social causes of death identified by medicolegal authorities have ranged from insufficient industrial safety standards, the deadly effects of inebriated driving, recreational tobacco use, and lethal police tactics like chokeholds and hog-tying. Establishing an evidentiary pattern of these deaths through forensic record keeping paved the way to the creation of regulations directed at these social causes and designed to save lives (Zevallos et al. 2004; Timmermans 2007; Jentzen 2009).
In recognition of shortcomings for observing certain social causes of death, the last update to the US Standard Certificate of Death adopted in 2003 included new mechanisms for tracking a limited array of social data (Siri and Cork 2009). The new form allowed for visualization of racial health disparities by including sections to record decedents’ race and ethnicity (recognizing Hispanic identity as an ethnic versus racial identity for the first time), included questions regarding the role of pregnancy in mortality, and added legitimacy to efforts to prove a connection between tobacco use and mortality by adding a checkbox querying whether tobacco use played a role in the death (Ibid., 51, 98–99).
My takeaway from this overview of limitations within vital statistics recording is to look toward two immediate reforms to standardize the counting of UBC deaths on the US Standard Certificate of Death. First, the California law requiring specific language on the “describe how injury occurred” section of a death certificate appears promising to ensure standardization for recording a trend in social deaths of concern (Moscufo 2022). A similar mandate could be proposed for recording decedents’ possible UBC status on their death certificates. As noted in the previous section, this use of the death form is already in practice in some jurisdictions, though it is not regulated.
Second, the addition of the tobacco checkbox to the US Standard Certificate of Death also appears promising, standardizing the listing of a common factor in American deaths that might otherwise be lost. A UBC checkbox could standardize the otherwise complex circumstances that local authorities have observed informally, but not otherwise noted in decedents’ associated death records, given that there is no straightforward mechanism to record this data currently. It is notable that the move toward adding a tobacco checkbox to the death certificate began at the state level.
The Tobacco Checkbox
The 2003 adoption of a tobacco checkbox on the US Standard Certificate of Death was the result of a process over a decade in the making. It began with state-initiated public health campaigns, spearheaded by five states—first Oregon and Utah by 1989, then Washington and Colorado, then Texas by 1993 (Gross 1989; Zevallos et al. 2004). The eventual national adoption of a tobacco checkbox was the result of lobbying efforts on the part of the American Medical Association (AMA) to bring awareness to the potentially lethal risk of tobacco use and what the AMA understood as systemic underreporting of tobacco’s impact in death records (Zevallos et al. 2004).
Oregon was among the first states to adopt a checkbox in 1989, but doing so was the culmination of a process that began 2 years earlier when state health officials noticed a potential lapse in their vital statistics collection. Based on the latest medical research they worried that fatal pulmonary conditions were being caused by tobacco use, but that there was no means to represent this causal element on death forms.
These officials contacted every doctor who filed death certificates on behalf of individuals who died the previous year due to conditions that might reasonably have been sequelae of tobacco use—conditions ranging from chronic lung disease to lung cancer. Of the over 3,000 state deaths attributed to such conditions in that period, 80 percent of doctors who responded confirmed their belief that the deaths were directly related to their patients’ tobacco use. But, they had only formally indicated the correlation of a death to tobacco use on 2 percent of death certificates (Gross 1989).
In response to this lapse, health officials decided to add a checkbox to their state death certificate, on which death filers could easily indicate whether the death was related to tobacco use. This started a domino effect that continued in other states, and finally the country as a whole (Gross 1989; Zevallos et al. 2004).
The statements that came in support of this measure are telling:
“It sends a very strong message,” said John M. Pinney, executive director of Harvard University’s Institute for the Study of Smoking Behavior and Policy. “This is another institutional recognition of the role of tobacco in deaths. For people on the borderline, who still don’t believe that the evidence is all in, this is a signal that we’re not kidding.” (Gross 1989)
A lawyer for the Tobacco Products Liability Project supporting the measure spoke to a New York Times reporter in 1989 to note that “a death certificate citing tobacco would be impressive trial testimony [against tobacco companies], although not conclusive. Moreover, he said, ‘this will be useful in recruiting plaintiffs’” (Ibid.).
Leading up to the modification of the US standard certificate, a review committee consisting of state-level public health officials recommended the addition, which was then reviewed and verified once more by panel of national experts. These results were published in 2000, updated in 2001, and resulted in implementation of the updated federal form by 2003—all a part of a scheduled review of the national death form. Its previous update was in 1989. According to the panel’s report, review of standard forms should take place every 10–15 years (Siri and Cork 2009). As no substantive updates to these standard forms have occurred since 2003, as of this writing in 2024, it is germane to note that the next review is long overdue. This presents a tremendous opportunity for change.
The death certificate has the potential to drive public understanding of social perils, validating research indicating the deleterious health consequences of recreational tobacco use that to that point had been met with skepticism—precisely because it lacked the substantiating scale of national-level mortality data as evidence for what doctors and researchers considered a meaningful factor in the deaths of a significant number of Americans. The collection served as proof to better inform consumer decisions, as well as a basis for consumers to seek remunerative legal action against tobacco companies that had failed to adequately represent their products’ entailed risks. These are all lessons that can directly apply on the border. There must be a way to systematically recognize a UBC death toll, and to highlight the connection of these deaths to policy to pave the way for remunerative action.
Manner of Death Categories
Simply standardizing counting is not enough. UBC deaths seem to be the result of policies that leverage possible corporeal harm or de facto death penalties for the act of unauthorized migration (De León 2015; Chambers et al. 2022). Though criminal liability for migration violations has been enhanced over the years, undocumented migration is hardly an act that the public would concede warrants a death sentence (though see McCann Ramirez 2024; Planas 2024). The problem is that, to a certain extent, BP acknowledges the deadly nature of border crossing, but casts itself as the humanitarian savior of border crossers (Tuiasosopo 2024; Williams 2016). This role was codified in MPURA’s recognition of both UBC deaths and simultaneously the role of BP’s humanitarian efforts to mitigate these deaths, absent any acknowledgement of the intended risk imposed by the agency’s deterrence policies.
A survey of incident reports and inquests dating from 2019 to 2022 in Brooks County, Texas, as well as conversations with the medical examiner in Webb County (personal communication, January 9, 2023) found that the majority of associated death certificates characterize UBCs’ Manners of Death as “Accident,” “Natural,” or “Undetermined.” The latter designation applies mainly to individuals recovered in states of advanced decomposition or skeletonization, although these indeterminable deaths are presumed on the whole to also have resulted from similar conditions as the classifiable deaths (Martínez et al. 2021). Death filers in these cases select from six available Manner of Death options standardized on the death form: “Natural,” “Accident,” “Suicide,” “Homicide,” “Undetermined,” or “Pending Investigation.”
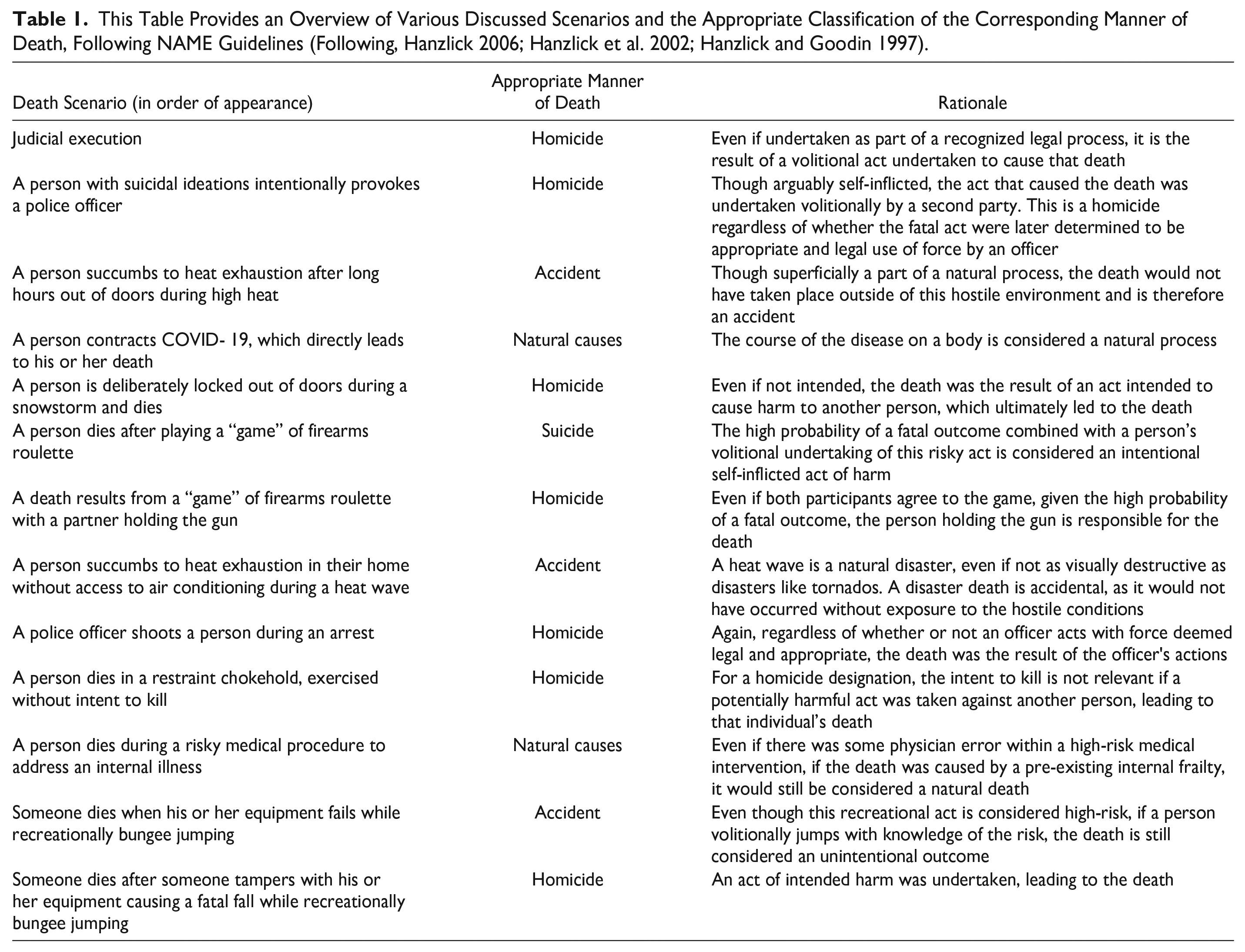
Here, I will briefly review the Manner of Death portion of the US Standard Certificate of Death and explain why characterizing deaths as “Accident” or “Natural” are both inaccurate. To illustrate this, I quote from NAME Manner of Death guidance at length as it outlines general principles for each kind of unnatural death:
Accident applies when an injury or poisoning causes death and there is little or no evidence that the injury or poisoning occurred with intent to harm or cause death. In essence, the fatal outcome was unintentional.
Suicide results from an injury or poisoning as a result of an intentional, self-inflicted act committed to do self harm or cause the death of one’s self.
Homicide occurs when death results from a volitional act committed by another person to cause fear, harm, or death. Intent to cause death is a common element but is not required for classification as [H]omicide [. . .]. It is to be emphasized that the classification of Homicide for the purposes of death certification is a “neutral” term and neither indicates nor implies criminal intent, which remains a determination within the province of legal processes. (Hanzlick et al. 2002, 6, bold emphasis added).
I propose that standardized counting of UBC deaths must be associated with an accurate characterization of their Manners of Death to ensure that official recognition of UBC deaths does not occur without co-recognition of their policy cause—as occurred with MPURA. Though MPURA recognized UBC deaths, its endorsement of BP’s humanitarian practice arguably undermined its value to meaningfully mitigate future deaths. If the goal of NVSS, in turn, is to instigate policy change to mitigate preventable deaths, then the role of policy in causing deaths must also be a part of the conversation.
Though some border death filers characterize UBC deaths as “Natural,” the role of the environment in what are predominantly heat-related deaths is a disqualifier for a “Natural” characterization. Per NAME, deaths due directly to extreme heat are appropriately “Accidental” because they are due to circumstances external to any individual maladies that may have caused a death. When extreme temperatures directly cause a person to die earlier than the individual would have otherwise, these external circumstances should supersede any underlying natural or internal conditions in Manner of Death filing, necessitating the filer to look to unnatural characterizations for most UBC deaths (Hanzlick et al. 2002). Crucially, an “Accident” designation applies for these conditions unless there is “intent to kill or harm the victim via the act of placing or leaving a person in such environment with apparent intent to do harm” (Hanzlick et al. 2002, 14). This is exactly what I identify as decisive for cases of UBC deaths.
If an individual corrals another person into a hostile environment with the intent to cause harm, and the second individual dies, this is a “Homicide.” As Boyce and Chambers (2021) explain, a corral effect is precisely what happens on the border, but there are policies and agencies at work instead of individual perpetrators. This role of policies versus individuals as actors complicates the element of necessary interpersonal action that qualifies a “Homicide” designation for UBC deaths. And yet, these deaths are not “Accidents” either. As I have written elsewhere:
The claim that border crossers are most responsible for the risks they undertake is categorically disingenuous (Boyce and Chambers 2021; Chambers et al. 2022). What overwhelms any claim that migrants choose the risks involved in border crossings, and by extent, that they are most responsible for harms that come to them, is that there is harm intended in border enforcement. Even if someone chooses a high risk activity, if another party, especially one with greater power and available resources, simultaneously works to extend that risk, it is bad faith to blame the first party for any resulting harm. (Soto n.d., under review)
UBCs may be undertaking a volitional risk in border crossings (Tuiasosopo 2024) as might qualify for characterizing their deaths as “Accidental,” but the risks involved are intended and enhanced by tactical infrastructure and paramilitary strategy underlying US border security policy and practice (De León 2015; Chambers et al. 2019, 2022; Boyce and Chambers 2021). In this sense, UBC deaths do not exactly fall under the necessary conditions for an “Accidental” death. Intent to cause harm, even if not death, is fundamental to prevention through deterrence.
Importantly, there is some precedent for states adding new Manner of Death categories to their death forms to navigate certain complex scenarios. For instance, there is ambiguity in characterizing deaths in the context of very ill patients under medical care. A death due to medical negligence—if an individual would not have died absent this negligence—is appropriately “Accidental.” The death was unintended, and the risk was initiated with a reasonable medical interest. Deaths resulting from high-risk medical procedures are “Natural” given that they resulted from patients’ internal health conditions that the medical procedures in question sought to mitigate (Hanzlick et al. 2002, 12). However, if the severity of the risk is not necessary—with some gray area over what constitutes necessity, or what kind of medical consensus would decide—the death would appropriately be an “Accident” if the decedent knowingly consented to the care (Ibid.). Given the gray area in characterizing these deaths, some states have adopted an additional Manner of Death, “therapeutic complication,” to standardize the otherwise mixed filings associated with these scenarios (Hanzlick and Goodin 1997; Gill et al. 2006). The addition of this category provides a potential path forward for navigating the parallel complexity of UBC cases—not appropriately “Natural,” “Accidental,” or “Homicides,” but indicating elements of each (Figure 1 and Table 1).
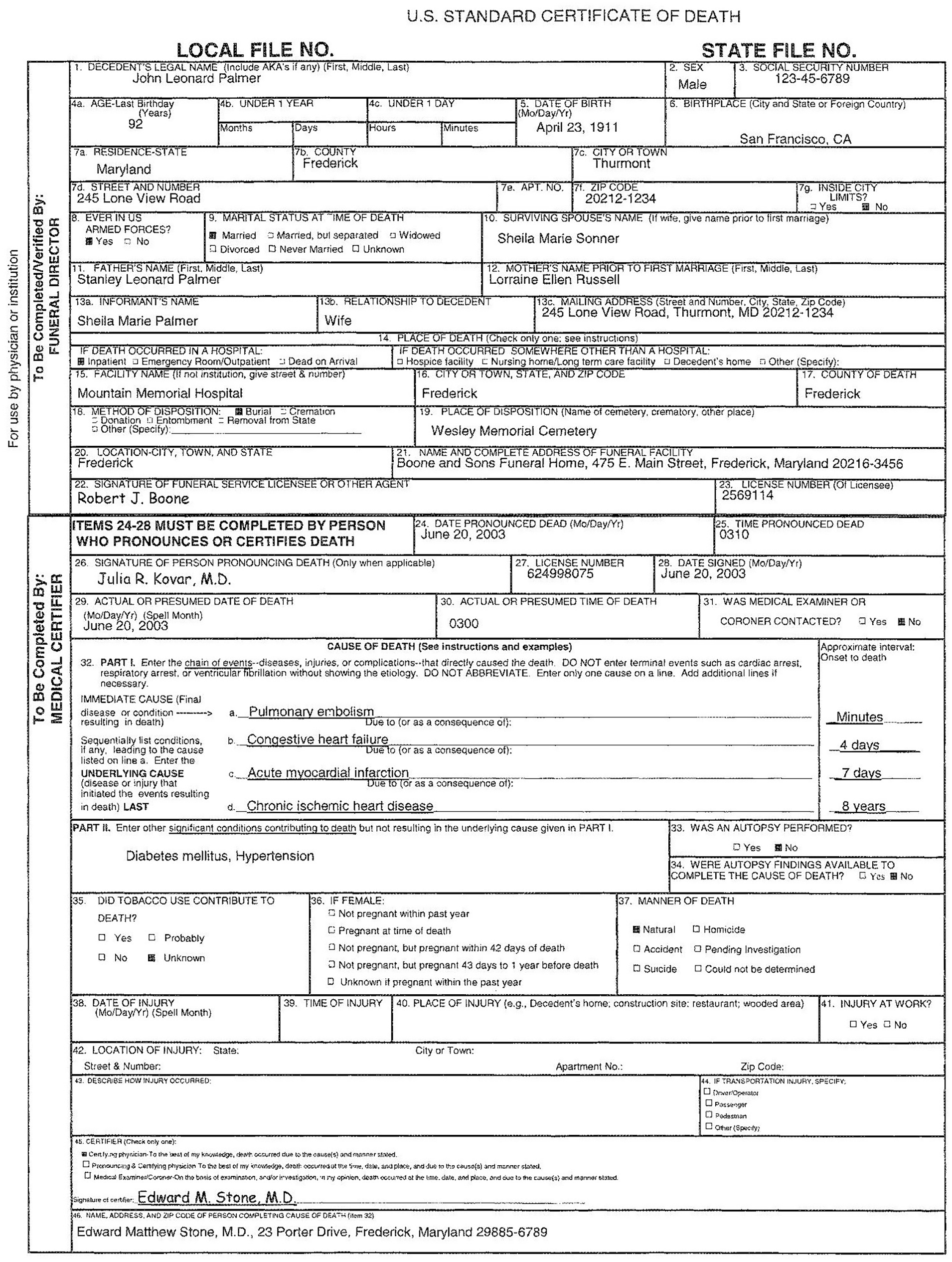
The US Standard Certificate of Death from the National Center for Health Statistics in the US Centers for Disease Control and Prevention (CDC). Parts 32 and 37 Represent the Cause and Manner of Death, Respectively. As a Work of the Federal Government, this Image is in the Public Domain. (CDC 2003: 107)
This Table Provides an Overview of Various Discussed Scenarios and the Appropriate Classification of the Corresponding Manner of Death, Following NAME Guidelines (Following, Hanzlick 2006; Hanzlick et al. 2002; Hanzlick and Goodin 1997).
Discussion and Recommendations
Standardized criteria for observing UBC deaths are necessary for several interrelated reasons. Most immediately, there is a necessity to observe UBC deaths across border jurisdictions in a way that is quite difficult and sometimes impossible to do now given not only a lack of standardization, but often a lack of awareness on the part of local officials of the need to observe migration-related deaths (BMI 2014; Gocha et al. 2018; Leutert et al. 2020; Soto 2020, 2022).
Current standards in the United States do not provide a reliable formal mechanism to count these deaths, so the jurisdictions that fail to do so are not in violation in any way per se. However, as frontline public servants with singular capacity to officially raise awareness for trends in how the population under their care dies, they are arguably in violation of the public obligations inherent in their role as medicolegal authorities (Timmermans 2007; Jentzen 2009). And yet there is a need to acknowledge too, that some jurisdictions may only observe small numbers of UBC deaths relative to others, such that they may not detect any trend. A lack of documentation might give the false impression that no deaths are occurring there and otherwise exacerbate what is estimated to be wide-scale undercounting of these deaths border-wide—because not all who die are found, and because they are systematically under-counted even when they are (Soto 2020a, 2020b).
Therefore the addition of a “UBC” checkbox, parallel to the tobacco checkbox added to the US Standard Certificate of Death in 2003, could ensure standardized accounting of this population. As with the tobacco checkbox, this could be adopted in coordination with state level public health authorities in the US southwest. This could facilitate eventual national adoption, which could capture fatalities related to human smuggling that may well be occurring outside of border states and zones where UBC deaths are concentrated.
In tandem, following California’s mandate for medicolegal authorities to explicitly describe when deaths take place at the hands of the police or in custody within the “describe how injury occurred” portion of its death forms (section 43), similar measures could be passed in border states to add context in documenting UBC deaths on death certificates (Moscufo 2022).
Finally, following precedent from states that have added “therapeutic complication” as an available Manner of Death on their death certificates, border states could adopt their own tailored Manner of Death category designed to characterize UBC deaths. As argued, available categories are inaccurate or misleading. Explicit language to leverage “cost” in “hostile terrain” as a deterrent for unauthorized migration (USBP 1994) means that when deaths result from this imposed cost, they are not “Natural” or “Accidents.”
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article is the result of research support from Arizona State University’s Sol and Esther Drescher Faculty Research Grant and its writing was undertaken as a 2023-2024 fellow of the American Council of Learned Societies.
1
This was an interview with members of the Binational Migration Institute who first formalized research in partnership with the PCOME.
2
69 officials involved in investigations of UBC deaths at the county, state, and federal levels were interviewed by a team from the Binational Migration Institute (BMI) between 2009 and 2014 in an effort to discern what protocols existed for this population of decedents. Interviews took place with a human subjects waiver from the University of Arizona Institutional Review Board given that the study concerned the official responsibilities of public officials. Subsequent studies were undertaken by the author in southeast Texas between 2019 and 2023, principally Brooks County, to determine how protocols for UBC death investigations since the county’s medicolegal officials were interviewed by the BMI team in 2012. Ethnographic research from 2019 to 2020 took place with IRB approval from Trinity College, IRB application #1312; from 2021, the research was IRB approved through Arizona State University, #STUDY00012233.
3
This shift came as the county developed a relationship with the BP’s Missing Migrant Program (MMP). As of 2021, MMP developed cooperative agreements with several Texas counties to compare fingerprints of probable UBCs they recover against a Homeland Security database including all individuals that have had any prior encounters with any branches of migration regulation or enforcement, as well as biometric records of relevant foreign consulates. MMP’s services have also included local trainings for local law enforcement to rehydrate fingers of partially decomposed individuals. In the past, without these databases available, fingerprint comparisons for decedents were run through crime databases compiled by the states and the Federal Bureau of Investigation. These were not very successful for identifying UBCs, leaving mainly DNA as an alternative mode of forensic identification—a process that notoriously takes months or years (Gocha et al. 2018). In contrast, after MMP began its relationship with Brooks County in 2021, records reviewed through 2022 found a 76 percent match rate for recovered and still fleshed remains of believed UBCs, most of which took place in under two weeks via MMP’s fingerprinting. Given limited available resources in WCOME, autopsy services contracted by Brooks County also commonly took several months and had historically not been as successful in deriving identifications (based on review of relevant inquest records before and after the end of Brooks’ contract with WCOME). 4. 4. This information is based on extended participant observation with a Brooks County justice of the peace in 2022, as well as interviews with a Brooks County sheriff’s commander (12/14/2022) and with MMP personnel (7/8/2021), also covered by LA Times reporting (![]() ).
).
4
Deaths of US citizens occurring abroad are recorded by a Consular Report of Death that accompanies a foreign death certificate.