
Abstract
Reducing race disparities in breastfeeding has become a health objective in the United States, spurring research aimed to identify causes and consequences of disparate rates. This study uses critical discourse analysis to assess how Black women are constructed in 80 quantitative health science research articles on breastfeeding disparities in the United States. Our analysis is grounded in critical race and intersectionality scholarship, which argues that researchers often incorrectly treat race and its intersections as causal mechanisms. Our findings reveal two distinct representations. Most commonly, race, gender, and their intersection are portrayed as essential characteristics of individuals. Black women are portrayed as a fixed category, possessing characteristics that inhibit breastfeeding; policy implications focus on modifying Black women’s characteristics to increase breastfeeding. Less commonly, Black women are portrayed as a diverse group who occupy a social position in society resulting from similar social and material conditions, seeking to identify factors that facilitate or inhibit breastfeeding. Policy implications emphasize mitigating structural barriers that disproportionately impact some Black women. We contribute to existing knowledge by demonstrating how dominant health science approaches provide evidence for health promotion campaigns that are unlikely to reduce health disparities and may do more harm than good to Black women. We also demonstrate the existence of a problematic knowledge set about Black women’s reproductive and infant feeding practices that is both ahistorical and decontextualized.
Health science research indicates that African American 1 mothers have lower rates of breastfeeding than other racial or ethnic groups (Centers for Disease Control and Prevention [CDC] 2020). Efforts to increase breastfeeding initiation and duration and reduce race disparities were U.S. government health priorities throughout the 2010s, as expressed in the Healthy People 2020 objectives and the U.S. Surgeon General’s 2011 Call to Action to Support Breastfeeding (U.S. Breastfeeding Committee 2020; U.S. Department of Health & Human Services 2011). These objectives spurred health science research aimed at understanding the causes and consequences of race disparities in breastfeeding, and breastfeeding promotion initiatives targeting groups identified as having lower breastfeeding rates.
Critical race and feminist theorists have expressed skepticism toward scientific research that focuses on race and gender disparities, arguing that such research often creates racialized and gendered subjects by presenting race and gender as essentialized characteristics rather than as socially constructed subject positions produced by unequal power structures in society. Critical race sociologist Tukufu Zuberi (2001; see also Zuberi and Bonilla-Silva 2008) argues that researchers, particularly those using quantitative statistics, often treat race or socially defined “racial characteristics” as causal mechanisms that create differences in social outcomes. This approach reifies perceptions that people of different socially constructed races are innately different from one another while ignoring systems of oppression. Likewise, feminist scholars such as Donna Haraway (1991), Dorothy Smith (1987), Nancy Hartsock (2004), and others argue that uncritical statistical analyses essentialize gender differences, making statistically observable differences that result from common experiences navigating the social world as gendered beings appear as innate differences stemming from one’s biological sex. These critical race and feminist scholars do not reject quantitative research but argue that how racial and gender statistics have traditionally been constructed, interpreted, and implemented into social policies and programs is problematic.
Black feminist scholars such as Kimberlé Crenshaw (1989) and Patricia Hill Collins ([1990] 2000), and more classically, Anna Julia Cooper (1892), point out that race and gender are not independent, but rather they intersect to create distinct subject positions. African American women are subject to unique forms of discrimination and controlling images not based on race or gender, but on the configuration of race and gender, as well as other significant social statuses, including age, social class, and sexual identity. Researchers have identified numerous examples of how public health messaging has produced gendered racialized subjects (C. Barcelos 2018; C. A. Barcelos and Gubrium 2014; Mann 2013; Waggoner 2015, 2017), but less research has focused on the science behind the campaigns, and none have looked specifically at health science research on breastfeeding. Scholars have advocated for increased attention to structural causes of health inequalities (Geronimus 2000; Krieger 1999; Link and Phelan 1996, 2000) and greater use of intersectionality in public health research (Bauer 2014; Bowleg 2012); however, it is unknown whether these approaches have been implemented in research examining race disparities in breastfeeding. Such research is needed to further academic understanding of how human sciences contribute to or challenge the construction and perpetuation of intersectionally marginalized subjects. Breastfeeding is an ideal site to examine this construction due to the proliferation of race disparities research and its prominence in U.S. national health objectives over the past decade.
In this study, we examine how African American women are constructed as gendered racialized subjects in health science research aimed at understanding race disparities in breastfeeding rates in the United States. We use critical discourse analysis (CDA; Fairclough 1992; van Dijk 1993) to uncover the hidden assumptions about African American women embedded in and perpetuated through a sample of quantitative health science research articles focused on race disparities in breastfeeding. We focus on articles published in the 2010s because reducing race disparities in breastfeeding was particularly highlighted as a national objective during this time period (U.S. Breastfeeding Committee 2020; U.S. Department of Health & Human Services 2011). Our analysis contributes to current literature examining the role of scientific research in perpetuating domination through discursive constructions of racialized and gendered subjects (Haraway 1991; Hartsock 2004; Smith 1987; Zuberi 2001; Zuberi and Bonilla-Silva 2008), and the multiple ways intersectional oppression manifests in the discourses, politics, and medical practices related to Black women’s reproduction (Bridges 2011; Davis 2019; Mann 2013; Prather et al. 2018; Roberts 1997; Waggoner 2015, 2017).
Literature Review
Race, Intersectionality, and Research
To develop a more complete understanding of how African American women are constructed in breastfeeding research, it is important to examine how race and gender are utilized in research. There are two conflicting perspectives on race and research: one claims a biological reality for race, and the other views race as a social construction that fosters social stratification. While the former has held more historical influence, foundational social scientists like W. E. B. Du Bois (1899) empirically demonstrated the latter through examination of the African American experience. Decades of research and activism have not reduced the relevance of Du Bois’s concerns with sociological methods, as problems persist in the categorical use of racialized variables (Zuberi and Bonilla-Silva 2008).
There is also debate between some scholars who push for “race-blind” analysis, which minimizes race as an irrelevant social construction, and others who seek racial justice through “race-conscious” analysis (Zuberi 2001). Proponents of race-blind analysis focus on individuality without historical considerations, which, through its lens of color-blind ideology, actually serves to perpetuate the racial status quo and ignores the adverse social conditions of those who are racially marginalized (Marks 2008), which can be just as harmful as misusing race in statistical reporting (Bonilla-Silva and Baiocchi 2008; Williams 2019; Zuberi and Bonilla-Silva 2008). Conversely, race-conscious researchers intentionally situate race contextually and historically in their analyses. Unfortunately, many social scientists using both race-blind and race-conscious analytical approaches have still consistently utilized racial data without actively considering or challenging existing biases in their conceptualization of race, thus legitimating racial inequalities (Zuberi 2001). As a result, even social scientists who believe both that racial bias persists in U.S. society and that race is a social construct still often fail to recognize that they may be unintentionally perpetuating racial bias in their own research.
In an effort to shift the scientific landscape with regard to the use of race data, some social scientists are challenging researchers to critically examine their own methodological approaches to race, calling for a change in the structure and foundational theory informing the statistics (Marks 2008; Williams 2019; Zuberi and Bonilla-Silva 2008). Standards in social statistics regularly fail to ground racial research in theory and consistently misuse race in their statistical construction, even when researchers understand race as a social construction (James 2008). Zuberi (2001) cautions researchers and data consumers to stop and examine the structure, theory, and methodology employed to draw conclusions. He argues that researchers too often view race as a causal mechanism—which suggests that race causes people to behave in specific ways—and recommends changing the language and structure of quantitative analyses with the acknowledgment that race is a socially constructed concept that is dependent on social conditions as variables. Doing so requires acknowledging the principle of manipulative causation, which holds that in order for a variable to be causal, it must be subject to manipulation—clearly race cannot be manipulated (Zuberi 2001). As Zuberi (2001) highlights, Statistical models that present race as a cause are really statements of association between the racial classification and a predictor or explanatory variable across individuals in a population. To treat these models as causal or inferential is a form of racial reasoning. (P. 129)
Understanding causal assumptions is appropriate for investigating the effects of racial stratification, as behavior that can be manipulated. Furthermore, theory, not statistical method, guides how researchers view and interpret race data. Interpreting statistical analysis must be connected to underlying causal theory.
A separate line of work has assessed the use of intersectionality in research, noting significant challenges for quantitative intersectionality to adequately account for the experiences and structural conditions of multiple marginalized groups while maintaining intersectionality’s critical foundation (Bowleg 2008; Else-Quest and Hyde 2016a, 2016b; Hancock 2007; McCall 2005). In her analysis of existing intersectionality research, Leslie McCall (2005) distinguishes between three categories of complexity: intercategorical complexity, often used in quantitative research, which compares intersectional groups on various outcomes; anticategorical complexity, which challenges existence of groups altogether; and intracategorical complexity, often used in qualitative research, which focuses on diverse experiences within an intersectional category. Dissecting this further, Greta R. Bauer (2014; Bauer and Scheim 2019) identifies descriptive intercategorical intersectionality as research that focuses on heterogeneity in outcomes, arguing that such research can be important for identifying inequalities and developing theories, but without attention to causal processes it risks reinforcing intersectional categories as essentialized characteristics. Greta R. Bauer and Ayden I. Scheim (2019) advance analytic intersectionality as a model for quantitative intercategorical intersectionality research that highlights heterogeneity in causal processes, such as discrimination, and provide guidelines for conducting such research. Thus, despite the qualitative focus of early intersectional research, there is some agreement that quantitative intersectionality can advance health science research in emancipatory ways (Bauer 2014; Bauer and Scheim 2019; Else-Quest and Hyde 2016a, 2016b; McCall 2005).
Although these developments in quantitative intersectionality hold promise for directing future research on reproduction, it is important to assess existing health science research to identify how intersectional subjects are currently portrayed. Existing scholarship demonstrates that Black women are particularly damaged by scientific constructions in the realm of reproduction. Dorothy Roberts (1997) demonstrates how controlling images of Black women as promiscuous have been used throughout U.S. history to control Black women’s reproduction, serving as justification for slave-breeding during slavery and for coercive contraception and aggressive welfare reform in the 1980s and 1990s. Similarly, stereotypes of Black women’s obstetrical hardiness, or ability to tolerate higher levels of pain during pregnancy and childbirth than other women, provide rationale for abusive obstetrical procedures such as non-therapeutic hysterectomies and involuntary surgeries (Bridges 2011; Hoberman 2005). Examination of how Black women are constructed in health science literature on breastfeeding will both advance understanding of how intersectional gendered and racialized subjects are produced through scientific research and contribute to the growing critical literature on race and reproduction.
Health Promotion, Breastfeeding, and Race
How Black women are constructed in health science research aimed at understanding race disparities in breastfeeding is likely connected to programming designed to reduce disparities. Health promotion campaigns have been identified as sites that foster and institutionalize notions of individual responsibility for personal and public health outcomes. Breastfeeding promotion campaigns typically focus on individual-level perspectives and knowledge of breastfeeding among expectant parents (Kukla 2006), which, like other reproductive health (C. Barcelos 2018; Mann 2013; Waggoner 2015, 2017) and HIV (Hoppe 2017) campaigns, place blame for illness or poor health on individuals and minoritized groups, ignoring U.S. cultural and structural factors that stratify health outcomes. Drawing on discourses of scientific medicine and risk, breastfeeding campaigns frame breastfeeding as a moral obligation and core component of being a “good mother” (Kukla 2006; Wolf 2007). This approach shifts responsibility for meeting national health objectives and improving population health from the state to the individual (C. Barcelos 2018; Jansson 2009; Waggoner 2015, 2017) and, in some cases, positions public health officials to work with other state agents to impose coercive and punitive strategies for managing individual (Hoppe 2017) and reproductive (Flavin 2008; Roberts 1997) health behaviors.
Health promotion campaigns have also been identified as sites of the production of harmful representations of gendered and racialized subjects (C. Barcelos 2018; C. A. Barcelos and Gubrium 2014; Mann 2013; Waggoner 2015, 2017). While ostensibly designed to improve health outcomes, particularly among minoritized groups, they often draw upon and reinforce stereotypical images in their campaign materials, reinforcing notions of racial difference and hierarchy. For example, in her analysis of the CDC’s preconception health campaign, Miranda Waggoner (2015, 2017) illustrates how White women are represented in heterosexual relationships as family “planners,” taking individual responsibility for their health and future fertility. In contrast, Black and Latina women are represented as unmarried, unpartnered, and financially unstable “non-planners,” who are “at risk” of unintended pregnancy and single motherhood. She argues that such messages reinforce a racialized good mother-bad mother dichotomy that reproduces harmful stereotypes and ignores systemic inequalities that contribute to disparate health outcomes. Chris Barcelos (2018) draws similar conclusions from analysis of community-based public health efforts to minimize teenage pregnancy among Latinas, which ignores structural causes and reproduces a narrative of Latino culture centered on Latina sexuality and domesticity. Our project seeks to expand this literature by examining the science behind health promotion campaigns, specifically in relation to race disparities in breastfeeding.
African American mothers face distinct social and institutional barriers to breastfeeding, which may or may not be acknowledged in the health science literature that informs promotion campaigns. The historical legacy of African American women being forced to breastfeed White babies in the Antebellum south underlies collective trauma and feelings of ambivalence toward breastfeeding (Blum 2000; Harrison 2016). Breastfeeding takes place within a broader context of medical racism in reproductive healthcare systems (Davis 2019; Roberts 1997), in which African American mothers have less access to maternity care practices that support breastfeeding than other groups (Cricco-Lizza 2006; Lind et al. 2014) and disproportionately undergo procedures—such as cesarean birth—that complicate breastfeeding (Getahun et al. 2009; McDonald et al. 2012). The hypersexualization of Black women’s bodies in U.S. history and culture make breastfeeding in the presence of others, whether in public spaces or private homes, a vulnerable act (Blum 2000; Hausman 2007; Owens et al. 2018). African American mothers are also disproportionately employed in full-time non-professional jobs, lacking paid maternity leave and adequate break time to express milk (Thulier and Mercer 2009). In recognizing the structural barriers that disproportionately inhibit breastfeeding among Black mothers, many do not regard breastfeeding as a requirement of good mothering, but instead either have conflicted views or associate it with extraordinary mothering, involving dedication and self-sacrifice beyond the requirements of being a “good mother,” which are not available to all mothers (Carter and Anthony 2015).
Some public health efforts to increase breastfeeding rates and reduce disparities do address structural barriers to breastfeeding, but they do not address forms of cultural and structural racism that contribute to race disparities. All U.S. states now have laws that at least decriminalize breastfeeding in public, with some states making it a crime to interfere with breastfeeding in public places (Carter and McCutcheon 2013). Other state initiatives include banning the aggressive marketing of infant formula, expanding breastfeeding support services offered through Women, Infants, and Children (WIC), and state-based quality collaboratives aimed at improving obstetric and neonatal healthcare (Gupta, Donovan, and Henderson 2017; Landau 2011). At the national level, the Patient Protection and Affordable Care Act of 2010 requires most employers to provide reasonable break time and a private, non-bathroom space to express milk at work, and requires health insurance companies to provide a breastfeeding pump and supplies. However, the provision for breastfeeding equipment does not extend to all Medicaid recipients, and many lower income workers have employers who are exempt from providing time and space to express milk (Hawkins, Dow-Fleisner, and Noble 2015). Furthermore, policies shown to have the greatest impact on increasing breastfeeding, such as paid extended maternity leave and the system of structural racism contributing to disparate breastfeeding rates, remain unaddressed.
Our study contributes to literature on how African American women are represented in health science research, specifically regarding racial disparities in breastfeeding. We analyze how quantitative research articles perpetuate or challenge embedded assumptions of Black women as racialized and gendered subjects and add to literature that illustrates the need for quantitative methodologies to intentionally avoid reifying essentialized racial and gender categories. Finally, we highlight alternative representations that clearly situate disparate outcomes in breastfeeding within a stratified social structure.
Research Method
In this study, we utilize CDA (Fairclough 1992; van Dijk 1993) to identify how intersectional positionality is constructed in contemporary quantitative health science research on race disparities in breastfeeding in the United States. We focus specifically on the constructions of Black/African American female subjects in research to unveil the underlying assumptions about this intersection of race and gender that drive research findings, which are, in turn, used to inform public policies and outreach campaigns aimed to increase breastfeeding rates.
The sample consisted of 80 quantitative research articles on breastfeeding disparities published in health science journals between January 1, 2010, and December 31, 2019. The sample was generated by conducting four article searches (two on MEDLINE and two on PubMed) using two sets of search terms for each year: (1) “race” and “breastfeeding,” and (2) “African American” and “breastfeeding.” The citation for each article was copied to a Microsoft Excel spreadsheet. Although the four searches generated many of the same articles, each original article was included only once. After the complete list of articles was compiled, each article was examined to determine whether it met the inclusion criteria using a four-question sequence. If the answer to a question was “yes,” then the article was passed on to the next question. If the answer to a question was “no,” the article was eliminated at that point and not assessed further. The inclusion questions were as follows: (1) Does the article focus on breastfeeding? (2) Does the article focus on breastfeeding in the United States? (3) Does the article focus on race disparities in breastfeeding in the United States between Black or African American women and women of another race/other races? (4) Is the article an original quantitative analysis or a quantitative meta-analysis? Only articles that met all criteria (“yes” to all questions) were included in the sample. The work of creating the sample was conducted by a team of student research assistants who were specially trained for the project and cross-checked by the authors.
The searches generated a total of 988 original articles; 536 were eliminated because they did not focus specifically on breastfeeding but on tangentially related topics such as pregnancy, childbirth, and early infant care. An additional 103 were eliminated because they focused on breastfeeding in some country other than the United States. Among the remaining articles, 221 were eliminated for not focusing on race differences in breastfeeding or not including Black or African American women. Finally, 48 articles were eliminated because they were not quantitative. The final sample consists of 80 articles, of which full-text versions were obtained for analysis.
We analyzed data using CDA (Fairclough 1992; van Dijk 1993) to examine how Black women are constructed in the articles. CDA is an analytic approach that aims to uncover the ways power is exercised through language and discourse, contributing to the production and reproduction of domination. CDA is based on the premise that power and domination are institutionalized, embedded in the specialized language of institutions. This language creates images of intersectional racialized and gendered subjects in society, which are socially constructed through unequal power relations and are subsequently acted upon through public policies, programs, and everyday interactions. To identify how Black women are constructed in the data, the following questions guided our analysis: What is a “Black woman” in the data? Based on this construction, what causes race disparities in breastfeeding, and what practical implications are suggested to address the identified causes? Consistent with our CDA approach, we attended to the overt portrayals of Black women, the more hidden, covert, or stereotypical images that were implied by the texts, and also what was missing or not included in the texts (Clarke 2005).
To begin coding, the first and third authors independently examined a sub-sample of 30 articles, each identifying similar patterns regarding how Black women, as intersectionally raced and gendered subjects, were portrayed in the articles. Due to lack of compatibility of some of the PDFs with NVivo software, we analyzed electronic or printed articles, highlighting relevant sections and making notations where themes were identified, and entered notes and pertinent quotes into a coding table in Microsoft Word. This organization facilitated comparison across articles, through which we identified discernable themes. These themes were presented to the other authors, who confirmed the analysis and generated additional insights. Following Emily S. Mann and Patrick R. Grzanka (2018), we incorporated each author’s insights to build the analysis rather than seeking uniformity in initial coding. After the general pattern of results was identified and confirmed, the first author coded the remaining articles into the identified categories, staying open to the possibility of identifying new themes.
Results
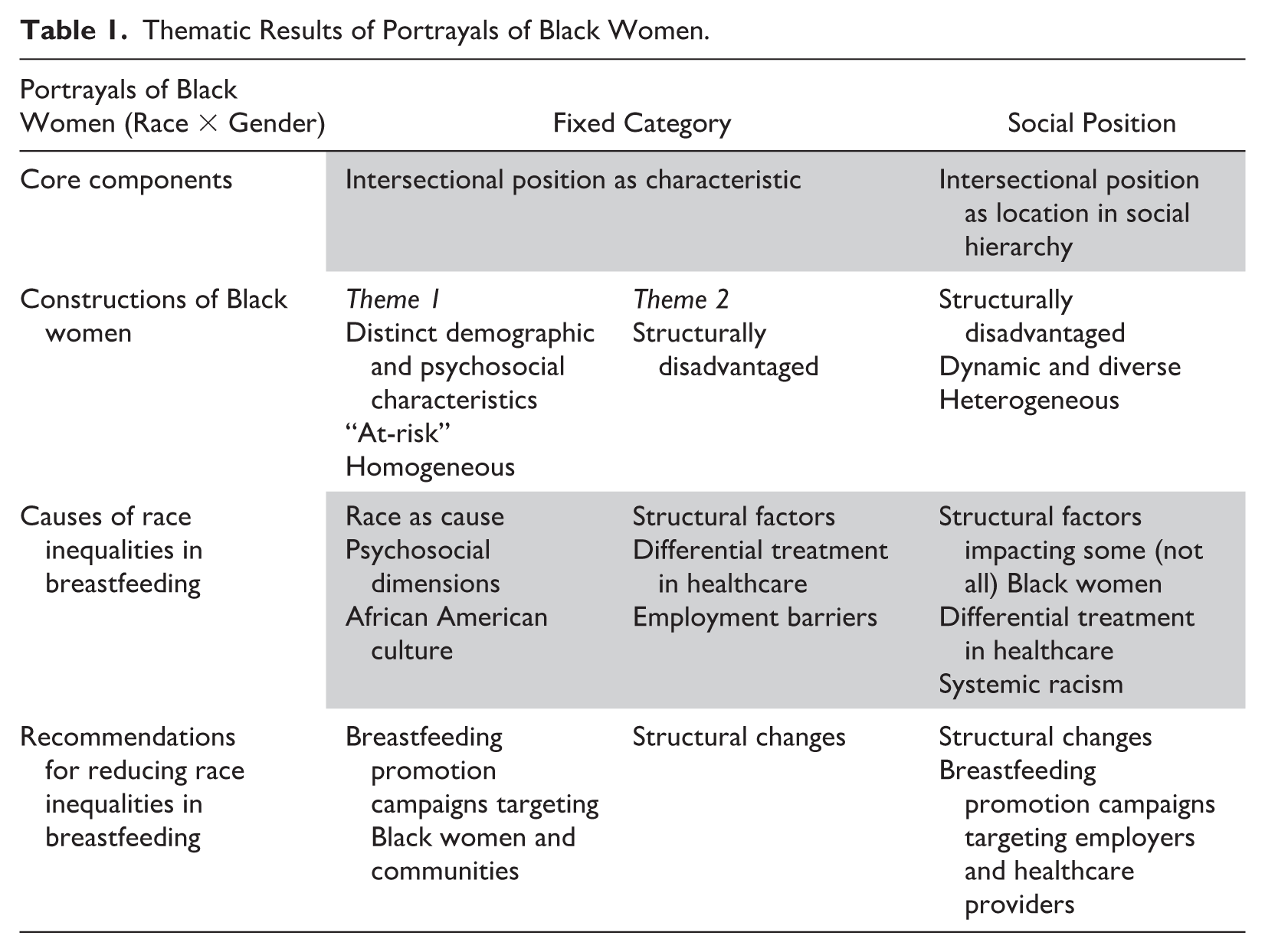
Data analysis revealed two distinct categories in the ways Black women were represented in health science research on race disparities in breastfeeding (see Table 1). The first and most prevalent category, identified among 75 percent (n = 60) of the articles, represented Black women as a fixed category of people. There were two themes within this category. The first and most common theme, identified among 72 percent of articles in this category (n = 43; 54 percent of the entire sample), represented Black women as a homogeneous group with distinct demographic and psychosocial characteristics that differ from other groups. The second theme, identified among 28 percent of articles in this category (n = 17; 21 percent of the entire sample), represented Black women as a homogeneous group that is structurally disadvantaged. The second, less common category, identified among 25 percent (n = 20) of the articles, represented Black women as occupying a distinct intersectional social position. Articles in this category portrayed Black women as a diverse group of individuals, who, based on social and material conditions, share some similar and some divergent experiences in U.S. society. There are distinct differences between the two categories in the characteristics associated with Black women, conclusions about the causes of race differences in breastfeeding rates, and policy recommendations to reduce disparities. We present the results by category to highlight the differences in how these approaches construct Black women in the context of breastfeeding research.
Thematic Results of Portrayals of Black Women.
Category 1, Theme 1: Black Women as a Fixed Category
Articles in the first category portray Black women as a fixed category of people, who possess attributes that are distinct from women of other racial and ethnic groups. In this portrayal, race, gender, and their intersection are presented as things, as concrete facts. Their existence is taken for granted, and the goal of research is to discern other characteristics that distinguish Black women from other groups which contribute to lower breastfeeding rates. Because all participants in the studies are identified as women, articles emphasize race as the distinguishing feature. For example, “Mean scores of 2 predictors (attitude and subjective norm) of [breastfeeding] intention were significantly different (P<0.01) among groups, which suggested a race-dependent difference in predictors for intention” (Bai, Wunderlich, and Fly 2011:1261) and “Being non-Hispanic black compared with Hispanic was marginally associated with half the odds of breastfeeding intention” (Sipsma et al. 2013:378). These examples illustrate the presentation of race as a fact, a characteristic of people that results in observable differences confirmed through scientific research. Because race is treated as something that exists, racialized intersectional subjects are portrayed as different kinds of people, with different attributes.
Approaching Black women as a fixed category, articles in this category portray them as a homogeneous group with distinct demographic and health characteristics. Black women are presented as disproportionately unmarried, low-income, WIC eligible or enrolled, and uneducated, constructions also identified in reproductive health outreach campaigns (Waggoner 2015). They are presented as having low “health literacy” and higher levels of distinct health issues related to breastfeeding, including being overweight or obese and having diabetes. As such, race is commonly constructed as a “risk factor” for not breastfeeding and, correspondingly, Black infants “at risk” of not being breastfed. Common statements alluding to risk include the following: “low socioeconomic status and African-American race have been shown to be risk factors for low rates of breastfeeding” (Alexander, Dowling, and Furman 2010:17) and “problem-solving and assessment of barriers is needed for at-risk populations such as single parent or step-families, [and] non-Hispanic black infants” (Odar Stough et al. 2019:54). One article, which examined the likelihood of being breastfed among babies of interracial parents, took the concept of risk further by stating in their abstract, “Breastfeeding non-initiation continues to pose the greatest risk for infants with at least one black parent” (Wallenborn et al. 2019:140). Consistent with broader discourses of race and reproduction (Solinger 2007; Waggoner 2015, 2017), articles in this category construct Black motherhood as a risk, posing a threat to Black children.
Based on these constructions of Black women, articles in this category aim to contribute to the literature by further identifying race differences in breastfeeding rates or by isolating causes or consequences of breastfeeding disparities. They draw on what Bauer (2014; Bauer and Scheim 2019) refers to as descriptive intercategorical complexity, which focuses on comparing intersectional groups on outcomes. Such an approach emphasizes between-group differences in measurable outcomes, while overlooking structural causal processes that produce disparate outcomes and minimizing within-group heterogeneity.
Articles seeking to verify race differences in breastfeeding or identify race differences among subpopulations (e.g., those living in rural areas) treat race as a cause of breastfeeding disparities, operating independently of other measured characteristics. For example, an article aiming to identify which maternal characteristics have the greatest impact on breastfeeding concluded, “maternal race and ethnicity was ranked as the fourth factor, once maternal education, age at delivery, and prepregnancy obesity were considered” (Xiang et al. 2019:172). These articles present race—a socially constructed concept—as operating independently to produce disparate outcomes.
Articles in this category that sought to identify causes of race disparities focused on race differences in psychosocial characteristics related to breastfeeding, such as individual-level beliefs, attitudes, preferences, and intentions. For example, an article seeking to identify “modifiable factors” related to breastfeeding concludes, . . . formula feeding comfort was higher among women who were African-American, less educated, and younger . . . In a proportional odds logistic regression model including all three demographic covariates, African-American ethnicity remained significantly associated with a higher level of formula feeding comfort . . . , whereas education level was marginally associated . . . , and maternal age was no longer significant. (Nommsen-Rivers et al. 2010:28)
By isolating other variables and comparing African American women with all other women combined, the article identifies a greater likelihood of reporting comfort with formula feeding among African American women, positioning them as an intersectional group with individual-level characteristics distinct from all other groups. Other articles in this category identify race differences in knowledge about breastfeeding, fear of associated pain, breastfeeding intention, and desire for bottle feeding. These individual-level differences are presented as causes of breastfeeding disparities, thereby reifying notions of racial difference.
Based on this understanding of racial difference in breastfeeding, articles that approached Black women as a fixed category typically concluded that their research supported breastfeeding promotion campaigns that target Black women and their communities. These interventions typically focus on changing the attitudes, knowledge, or perceptions of breastfeeding among Black expectant mothers and the people around them. For example, an article in this category recommends, Low-income African-American women appear relatively well educated about the health benefits of breastfeeding but much less knowledgeable about the actual process of breastfeeding, so an important area for intervention will be education about what to expect when breastfeeding . . . “Life coaching” after the infant’s birth to help the mother negotiate lifestyle challenges associated with breastfeeding, such as work/school issues, holds potential promise as an innovative area for intervention. (Alexander et al. 2010:22)
As this excerpt illustrates, articles in this category tended to recommend promotion campaigns aimed to modify African American women in ways predicted to increase breastfeeding. The emphasis on individual-level modification programs, based on the construction of African American women as possessing distinct characteristics, aims to modify these characteristics as a way of achieving breastfeeding objectives determined by the state. Consistent with other health promotion campaigns, such an approach makes racialized gendered subjects individually responsible for public health outcomes (C. Barcelos 2018; Jansson 2009; Waggoner 2015, 2017).
Category 1, Theme 2: Black Women as a Fixed Category Who Are Structurally Disadvantaged
Articles in the second theme within the first category construct Black women as structurally disadvantaged. These articles approach race as a significant characteristic but emphasize it as a source of disparate treatment in society. Articles in this category construct Black women as an “underrepresented group,” “minority group,” and “vulnerable population.” They note patterns in disproportionate social conditions, such as food security or income level, while also highlighting heterogeneity in factors such as income and education.
Articles using this construction aim to identify structural inequalities that contribute to race differences in breastfeeding such as differential treatment by healthcare providers or employment barriers. For example, an article investigating differences in breastfeeding by race and geographic state in the United States treats race as a fixed characteristic, stating, “Because black infants have consistently had the lowest rates of breastfeeding initiation and duration compared to other groups, the state-level estimates presented are limited to black and white infants” (Anstey et al. 2017:723). The article presents data showing lower levels of breastfeeding by Black infants and focuses on structural barriers in the discussion, stating, “Certain barriers are disproportionately experienced by black women (e.g., earlier return to work, inadequate receipt of breastfeeding information from providers, and lack of access to professional breastfeeding support)” (Anstey et al. 2017:724). In contrast to articles presenting Black women as a particular type of person, articles in this category present Black women as a distinct category that engages in observable patterns of actions that are attributable to collective disadvantaged by current social conditions.
Consistent with the view of breastfeeding disparities as an outcome of structural disadvantage, articles in this category recommended structural changes as mechanisms for promoting breastfeeding among African American women. Recommendations include more comprehensive state laws supporting breastfeeding in workplaces, more equitable distribution of lactation services in rural areas and race-segregated neighborhoods, and changes in maternity care practices, especially in hospitals. For example, an article identifying that provider bias and differential treatment correspond with race differences in breastfeeding concludes, “Acknowledging and addressing equitable perinatal provider support could be an important step for improving breastfeeding rates and reducing maternal and child health disparities” (Sipsma et al. 2019:747). Another article that identifies disparate treatment in hospital care posits, “. . . addressing racial disparities in in-hospital breastfeeding support may be an important modifiable factor in increasing breastfeeding rates and encouraging mothers who do breastfeed to practice correct methods” (Gee, Zerbib, and Luckett 2012:433). This article presents hospital practices as a “modifiable factor” in contrast to several articles in the previous category which present individual-level factors such as comfort with formula as a “modifiable factor.” Although articles in this category do not overtly challenge the concept of race as a fixed characteristic, they point to structural inequalities as both the cause and solution for disparities in breastfeeding outcomes.
Category 2: Black Women as Occupying a Social Position
Articles in the second category portray Black women as a dynamic group occupying distinct social positions in U.S. history and society. This representation acknowledges difference and diversity, presenting Black women as a heterogeneous group, and emphasizes structural barriers that contribute to disparate outcomes. This approach draws upon what McCall (2005) calls intracategorical complexity, which identifies differences within an intersectional category. It emphasizes structural barriers that may have a differential impact based on the intersection of multiple characteristics including race, ethnicity, and gender as well as other social statuses such as nationality, social class, education, and employment status. For example, an article in this category states, “Given the trend of more working mothers, the intersection of race, work, and family has become increasingly important and is further highlighted in the instance of the promotion of breastfeeding” (McCarter-Spaulding, Lucas, and Gore 2011:38). This excerpt illustrates how articles in this category portray race as one factor that intersects with others to produce distinct social positions, which in turn correspond with identifiable outcomes. This perspective presents Black women as occupying multiple distinct social positions rather than comprising a single, fixed category of people. Similarly, another article states, “This racial disparity in breastfeeding is not explicated by demographic characteristics (e.g., education) alone, signifying that external factors within each race may have a stronger association with breastfeeding” (Jefferson 2017:149–50). This article attributes race disparities in breastfeeding to external factors, considering how the intersection of race and gender positions individuals in society to have different social experiences. Like others in this category, this representation attributes observed differences as an outcome of external social conditions rather than individual characteristics.
Articles that approach Black women as occupying a social position present them as a dynamic and diverse group. For example, In this sample, where only Black women were invited to participate, participants were also asked to describe whether they were Hispanic (8.6% of the sample), and additionally how they would describe their family background, allowing for further information about ethnicity. Several ethnicities were represented, with the majority (32.2%) being African-American. One quarter (25%) of the sample reported that they were of mixed or multiple backgrounds, and one quarter of the sample (25%) described themselves as Caribbean. Women who described themselves as African comprised 9.9% of the sample, and 7.9% of the sample described their ethnicity as Cape Verdean. (McCarter-Spaulding et al. 2011:40)
This excerpt illustrates the portrayal of Black women as a diverse group, and race and ethnicity as identities rather than fixed characteristics.
Articles that present Black women as occupying a social position emphasize the social conditions more commonly experienced by Black women compared with other intersectional groups. Black women in these articles are portrayed as a group of people similarly impacted by social conditions, such as maternal employment, workplace characteristics, or hospital practices, which in turn constitute discernable patterns of actions. For example, an article assessing breastfeeding among women living in military settings states, We speculate that such well-known racial disparities [in breastfeeding] may disappear in the military setting . . . the military setting provides stable employment to populations who face an otherwise poor labor market and offers educational opportunities and healthcare to soldiers and family members . . . Notably, military health insurance features a well-child program, which, since 2001, has covered breastfeeding consultation for military families. (Lundquist et al. 2015:420)
This article presents Black women as a group of people who are similarly positioned in relation to the labor market, educational opportunities, and healthcare. Finding that “Black women in the military breastfeed for a longer duration than civilian black women,” the authors conclude, “This paper is an important first step in calling attention to the fact that breastfeeding prevalence and racial disparities in duration are elastic and alterable depending on the setting” (Lundquist et al. 2015:425). Articles such as this one present race disparities in breastfeeding as an outcome of disparate structural and material conditions. Whereas most articles in this category refer to disadvantage or disparate treatment, one article explicitly names racism as a cause of breastfeeding disparities, identifying connections between experiences of racism, neighborhood segregation, and breastfeeding (Griswold et al. 2018).
Although most articles in this category analyze structural-level factors, four articles examine psychosocial dimensions that impact breastfeeding, yet they examine differences among Black women rather than between Black women and women of other races and ethnicities. An article seeking to understand the role of breastfeeding self-efficacy and breastfeeding outcomes among African American women states, “Placing African American women at the center of research related to their infant feeding practices may offer clarity to previous contradictions noted in the literature related to this population and infant feeding” (Robinson and VandeVusse 2011:321). Using this approach, the article concludes, The findings from this study suggest that breast-feeding self-efficacy has an impact on infant feeding intentions for African American women . . . Researchers examining women of African descent found that women in this population who had high self-efficacy scores breast-fed for similar durations when compared with White women. Therefore, in regard to breast-feeding, the more self-efficacious a woman is, the more likely she is to intend, initiate, and continue to breast-feed. (Robinson and VandeVusse 2011:326)
By analyzing differences among African American women, these articles represent African American women as a dynamic and diverse group, which contrasts with articles in the first category that presented them as homogeneous. Thus, although African American women share a common race and gender intersectional subject position, their psychosocial attributes are diverse, which correspond with varying levels of breastfeeding among African American women.
Articles that approach Black women as occupying social positions focus their policy implications on the structural level, aiming to modify social conditions that contribute to disparate breastfeeding rates. These articles recommended changes in legislation regarding healthcare coverage for lactation support, geographic availability of lactation support services, and campaigns to educate healthcare providers and employers about current disparities in breastfeeding support and the benefits for institutions to support breastfeeding. For example, an article focusing on connections between employment conditions and breastfeeding among Black women shows that the timing of returning to work was connected to weaning. The article concludes, This puts women without access to maternity leave at greater risk for early weaning, and suggests the need for a maternity leave policy that allows women to breastfeed longer . . . Many women are combining employment and breastfeeding. For many, their socioeconomic position does not allow them any other choice. What must then be addressed is the need for “family-friendly” workplaces that include being “breastfeeding friendly.” (McCarter-Spaulding et al. 2011:43)
In advocating breastfeeding friendly workplaces, the article addresses the benefits to businesses for supporting breastfeeding, stating, “In fact, the United States Department of Health and Human Services has recently begun a coordinated outreach program, the Business Case for Breastfeeding, to educate employers about the long-term economic benefits of breastfeeding” (McCarter-Spaulding et al. 2011:43). In contrast to the health promotion campaign approach, which targets groups of women to change their beliefs or behaviors, articles in this category recommend education programs for business leaders about the benefits of workplace breastfeeding programs. This approach seeks to modify the social conditions that position Black women to be less likely to breastfeed rather than modifying Black women themselves. In doing so, it shifts responsibility for meeting public health objectives from individual women to the social institutions and material conditions that impact their lives.
Articles in this category not only recommend changes at the structural and institutional levels, but they also critique breastfeeding promotion campaigns for being ineffective and for setting women up to fail. The article cited above continues, In order to meet current breastfeeding goals, particularly for low-income women and women of color, maternity leave and employment policies must be in place to facilitate continued breastfeeding. Encouragement to continue breastfeeding without such support will not suffice, and will most likely contribute to continued disparity in breastfeeding rates and health outcomes. (McCarter-Spaulding et al. 2011:44)
This example illustrates a critique of breastfeeding promotion campaigns and other approaches that target individual women with breastfeeding advice or information but do not change the conditions that inhibit breastfeeding, arguing that such approaches contribute to continued race disparities.
In sum, articles in this category emphasize that social conditions, not types of people, are the cause and solution to race disparities in breastfeeding. This construction is achieved by representing Black women as a diverse and dynamic group who may share some common treatment based on the intersection of race and gender, but who also have divergent experiences based on other status characteristics such as education or employment status, and individual-level psychosocial attributes.
Discussion
In this article, we used CDA to investigate how African American women are constructed in health science research articles on race disparities in breastfeeding. Our analysis yielded two main categories of representations: (1) Black women as a fixed category and (2) Black women as occupying a social position. Articles in the first and most common category treat race, gender, and their intersection as things, or as concrete, factual characteristics of people. Consistent with scholarship from critical race (Zuberi 2001; Zuberi and Bonilla-Silva 2008), feminist (Haraway 1991; Hartsock 2004; Smith 1987), and intersectionality (Bauer 2014; Bauer and Scheim 2019; McCall 2005) perspectives, this approach reifies intersectional categories, thereby producing racialized gendered subjects who are shown, through science, to have attributes that differ from other groups. In most of the breastfeeding research we analyze that uses this approach, individual-level attributes are examined and consequently identified as the cause of breastfeeding disparities, which, correspondingly, positions Black women as the appropriate targets of government efforts to reduce disparities. This approach portrays race rather than racism as the cause of race disparities in health outcomes. Fewer articles in this category examine structural rather than individual causes of breastfeeding disparities, yet they still utilize the concept of race, and the construction of racialized gendered subjects, uncritically. Although these articles do some good by addressing structural factors contributing to racial inequalities, they do not push for a critical interrogation of the construction of Black women as a category. Likewise, they examine the manifestation of oppression in particular institutions (e.g., healthcare, workplace) without addressing broader overlapping systems of racism, sexism, and other -isms, or their historical contexts.
The reification of intersectional categories through health science research positions Black women as racialized gendered subjects who are individually responsible for broader public health outcomes. This research provides scientific evidence supporting the need for breastfeeding promotion campaigns targeting Black women which focus on attitudinal and behavioral changes at the individual level. Such promotion campaigns are critiqued in social science research for perpetuating neoliberal approaches to health by emphasizing self-governmentality, which shifts responsibility for achieving public health objectives from states to individuals (Hoppe 2017; Jansson 2009; Mann and Grzanka 2018; Waggoner 2015, 2017). In the context of breastfeeding, such initiatives would likely hold African American women individually responsible for current disparities in breastfeeding rates and for making individual-level changes to mitigate such disparities at the state and national levels. Scholars have also identified that health promotion campaigns reproduce stereotypical images in their promotional materials that further reify racial differences and problematize Black women’s sexuality and reproduction (C. Barcelos 2018; C. A. Barcelos and Gubrium 2014; Mann 2013; Waggoner 2015, 2017). Breastfeeding promotion campaigns tend to publicize the health benefits of breastfeeding without providing guidance on breastfeeding techniques which, within the broader U.S. context of inadequate hospital- and community-based lactation services and lack of structural support such as extended paid maternity leave, set women up for breastfeeding failure (Jansson 2009; Wolf 2007). Taken together, our findings represent an important contribution to existing knowledge: Much of health science research uses approaches that provide evidence for health promotion campaigns that are not likely to have a significant impact on breastfeeding disparities. Furthermore, our findings suggest that, even though much of this research ostensibly intends to improve outcomes for Black women and reduce racial disparities, it may do more harm than good to Black women.
Articles in the second and less common category treat Black women as occupying a distinct intersectional position in U.S. society. As such, this approach acknowledges Black women as a socially constructed group comprised of individuals who may share similar social histories and current conditions of systemic marginalization and discrimination. This construction acknowledges differences within the category, drawing on what McCall (2005) identifies as intracategorical complexity, which presents Black women as a diverse group of individuals, with different ethnicities, education levels, employment conditions, and so on. More closely aligned with the analytic intersectionality approach that Bauer and Scheim (2019) advocate, when combined with an emphasis on structural factors that impact breastfeeding, this approach presumes that differences in social position are created by heterogeneity in causal processes, such as discrimination in healthcare or unequal access to quality lactation services. Research from this perspective seeks to identify structural factors associated with breastfeeding initiation and duration among Black women, further portraying the group as diverse and dynamic, yet identifying barriers to breastfeeding that are specific to the intersectional social positions that Black women occupy. Policy implications focus on removing barriers that inhibit breastfeeding among Black women at the institutional level, aiming to provide equal opportunities to breastfeed by mitigating disparate treatment in healthcare and the workplace. This approach holds greater promise for the future of health disparities research and policy, yet it still largely relies on a neoliberal approach to solving social problems whereby simply removing institutional obstacles for historically disenfranchised groups is presented as the sole factor needing to be changed to create actual equality. It identifies race inequalities as a cause of disparate outcomes, but it does not directly address racism as a fundamental cause (Phelan and Link 2015).
We also make an important contribution to health science research by demonstrating the existence of a problematic knowledge set about Black women’s reproductive and infant feeding practices that is both ahistorical and decontextualized. This body of research, along with other research on sexual and reproductive health, would benefit from greater interrogation of how broader systems of oppression and privilege operate intersectionally to produce unequal health outcomes, and from stronger historical contextualization. Cynthia Prather and colleagues (2018) assert the importance of historicizing reproductive health disparities by illustrating parallels in African American women’s personal and healthcare experiences in the United States from slavery to the present day. Beginning with public gynecological exams to determine reproductive ability and the systematic rape of enslaved Black women, which corresponded with non-consensual reproductive surgeries performed without anesthesia, they illustrate how historical and contemporary exploitation in reproductive healthcare settings is inextricably connected with broader systems of gendered racism. In the post–Civil Rights Era of today, hypersexual images of Black women along with disproportionate systemic poverty correspond with unequal access and provision of healthcare and lack of trust based on targeted birth control and sterilizations. Contemporary breastfeeding practices among African American women take place within this historical context of exploitation by reproductive healthcare providers and forced breastfeeding during slavery (Blum 2000; Harrison 2016) along with a current healthcare system that creates disparate reproductive outcomes (Bridges 2011; Davis 2019). The fact that there is a significantly lower likelihood that African American women and their infants will survive the U.S. maternity care system due to medical racism (Davis 2019) cannot be ignored when seeking to understand early infant feeding practices. Yet, the bulk of the research articles we analyzed, even those which approach Black women as occupying a distinct subject position, tend to de-historicize current trends. A body of research is needed that uses critical intersectional perspectives to unveil the deep connections between African American women’s history of exploitative and coercive reproduction and breastfeeding and the overlapping racist and sexist structures that continue to produce unequal outcomes.
Finally, our analysis demonstrates a clear need for research that can account for multiple interlocking systems of oppression beyond only race and gender. The articles we analyzed often accounted for socioeconomic inequalities, yet they did not include any mention of gender or sexual identity. Mainstream health science research must identify how heterosexist and cisnormative structures shape reproductive and breastfeeding discourses and practices, and how they intersect with other forms of systemic oppression to create an interlocking system that produces sexual and reproductive health disparities. As Lisa Bowleg (2012) points out, Acknowledging the existence of multiple intersecting identities is an initial step in understanding the complexities of health disparities for populations from multiple historically oppressed groups. The other critical step is recognizing how systems of privilege and oppression that result in multiple social inequalities (e.g., racism, heterosexism, sexism, classism) intersect at the macro social-structural level to maintain health disparities. (P. 1267)
Expanded research using these approaches holds promise for producing real solutions to intersectional inequalities.
Footnotes
Acknowledgements
We appreciate the constructive feedback we received from the journal editors David Embrick and David Brunsma, managing editor Kevin Zevallos, and the anonymous reviewers, which helped us develop our article. We would also like to extend a special thank you to our student research assistants, Darryl Washington, Seth Shepard, Emely Matos, Alexandria Engle, and Maxine Campisciano, who dedicated many hours sorting through research articles to help construct the data set for this project.