
Abstract
Effects of pervasive exposure to trauma result in a costly public health crisis. Trauma-informed care (TIC) is a well-known and established health care approach for supporting individuals who experience trauma. Despite increasing recognition of its importance, TIC remains poorly integrated into nursing education, with reasons that are not yet well understood. This interpretive descriptive study explored nurse educators’ perspectives on the facilitators and barriers for embedding TIC into nursing curricula in Ontario, Canada. Twenty eight participants were purposively sampled from an online survey of 145 respondents for semistructured interviews. Reflexive thematic analysis guided the generation of key facilitators and barriers. Facilitators included: passionate educators, innovative teaching strategies, supportive leadership, and collaborative teaching models. The barriers to TIC integration in undergraduate nursing programs included: the invisibility of TIC in curricula; a lack of faculty training and confidence; overloaded, siloed program structures; challenges with authentic assessment; and inconsistent role modelling in clinical settings. Embedding TIC into undergraduate nursing education requires intentional curricular mapping, institutional support, faculty development, and alignment with clinical practice and experiential learning. Effective integration of TIC in undergraduate nursing curricula is needed to equip nurses to address the growing global burden of trauma and support a resilient nursing workforce.
Keywords
Traumatic exposure represents a pervasive and costly public health crisis, producing profound biological, psychological, social, and physical consequences that demand urgent attention (Fallot & Harris, 2009; Stokes et al., 2017). Trauma is defined as an event, series of events, or circumstances experienced as physically or emotionally harmful or threatening, with lasting adverse effects on an individual’s functioning and overall well-being (Substance Abuse and Mental Health Services Administration [SAMHSA], 2014). People who experience trauma are at risk for significant mental and physical health effects that are complex, long-lasting, and intergenerational (Benjet et al., 2016; Campbell, 2002; Han et al., 2021; Perfect et al., 2016). The complexity of these health effects results in frequent interactions with health care providers across various settings and sectors of care (Elliot et al., 2005; Varcoe et al., 2019). Given the profound impact of trauma on physical and emotional well-being, trauma is considered a significant public health issue (Orionzi, 2023; SAMHSA, 2014). Because trauma is defined by the individual’s subjective experience rather than objective criteria, nurses must be prepared to recognize and respond to its diverse and lasting impacts on health and well-being (Harris & Fallot, 2001). Because of the high prevalence of people who experience traumatic events and to prevent people from being unintentionally distressed and re-traumatized (Coyle et al., 2019; Wathen et al., 2021a), health care providers and organizations must address the effects of trauma in the delivery of all health care services, regardless of context (Elliott et al., 2024; Muskett, 2014; Ross et al., 2025; Stokes et al., 2017). This approach to service delivery is known as trauma-informed care (TIC), an emerging concept in the nursing education literature (Elliott et al., 2024; Li et al., 2019; Overstreet & Chafouleas, 2016). Importantly, TIC does not directly treat or resolve trauma itself, nor does it require disclosure; rather, it is an approach to care that seeks to recognize trauma and mitigate its negative impacts on individuals’ health care access and experiences, including preventing re-traumatization and promoting psychological safety within care encounters (Stokes et al., 2024). A critical global gap in best practices for preparing nurses to deliver TIC exists. Although nurses are often the first point of contact for individuals with trauma histories, there is no internationally recognized framework for integrating TIC into undergraduate nursing education (Goddard et al., 2021). This lack of preparation undermines nurses’ ability to provide safe, equitable, and competent care and risks perpetuating harm in clinical encounters. As a result, the academic sector is increasingly called upon to develop and embed curricular resources that equip graduates to recognize trauma, prevent re-traumatization, and foster healing (Burton et al., 2019; Goddard et al., 2021; SAMHSA, 2014).
In Canada, the Canadian Association of Schools of Nursing (CASN) includes TIC as one of the expected learning outcomes in its overall undergraduate nursing education framework (Canadian Association of Schools of Nursing, 2022). In the province of Ontario, the College of Nurses of Ontario (CNO) updated their Entry-to-Practice (ETP) Competencies for Registered Nurses to require the competent application of TIC by entry-level nurses (CNO, 2019). Otherwise, policy and evidence that inform nursing education in TIC remain sparse (Burton et al., 2019; Elliott et al., 2024; Wheeler & Phillips, 2021). Therefore, this study aims to address this critical gap by examining nurse educators’ perceptions of TIC and the barriers and facilitators to its integration.
Background
Trauma-Informed Care
TIC is a well-established, theoretical, and organizational framework that acknowledges the widespread prevalence of trauma and the need to meet the needs of trauma survivors by understanding the effects of trauma and its close links to health (Goldstein et al., 2024; Grossman et al., 2021; Wathen et al., 2021a). Universal approaches to TIC implementation are required to prevent people from becoming distressed or re-traumatized during health care experiences (Stokes et al., 2017). TIC frameworks can be applied to create a safer environment for patients and health care professionals and improve both process and patient outcomes (Ashworth et al., 2023; Brown et al., 2022). When practicing with a TIC lens, health care providers and organizations deliver care and services on the assumption that everyone has a history of trauma (Coyle et al., 2019; Elliot et al., 2005; Hopper et al., 2010; Stokes et al., 2017; Strand et al., 2016). It requires a fundamental shift from thinking, ‘What is wrong with you?’ to considering ‘What happened to you?’ (Stokes et al., 2017, 2024; Sweeney et al., 2018).
Providers who understand the exposure to and experiences of trauma can help create safe spaces in care settings and limit further harm (SAMHSA, 2014). In particular, front-line providers must recognize the complex and lasting impacts of trauma (Baker et al., 2016; Levine et al., 2021; Ponic et al., 2016; Varcoe et al., 2021) as this has been shown to improve provider and patient experiences and outcomes (Chafouleas et al., 2016; Ford-Gilboe et al., 2018; Purkey et al., 2020; Ross et al., 2025; Stokes et al., 2017). Provider outcomes include improvements in patient-provider relationships (Bendall et al., 2021) and increased practitioner knowledge (Demers et al., 2022; Lewis et al., 2023). Patients have been shown to benefit from improved client mental health (Chin et al., 2024), improved client self-efficacy and perception of self-management of chronic illnesses (Demers et al., 2022), and reduced re-traumatization (Bargeman et al., 2022; Goldstein et al., 2024).
Global evidence further highlights the persistent gap between TIC principles and their implementation in practice. In Australia, multiple reports and inquiries over the past decade have recommended implementing TIC across health systems. In response, the implementation and evaluation of TIC have become federal, state, and local priorities, particularly within mental health services. Despite these efforts, managers, clinicians, and consumers continue to report challenges translating core TIC principles into practice, citing limited implementation support and the need for system-wide culture change (Agency for Clinical Innovation, 2022). These findings underscore that the integration of TIC into undergraduate nursing education is not solely a curricular issue, but a critical strategy for preparing graduates with the capacity to apply trauma-informed principles effectively within complex health care environments (Agency for Clinical Innovation, 2022).
Trauma-Informed Care in Baccalaureate Nursing Education
Emerging evidence suggests that educating health and social services providers about TIC can lead to practice change (Ross et al., 2025). People who have experienced trauma frequently receive care from nurses as their primary caregivers; therefore, registered nurses are especially well-positioned to implement a trauma-informed approach to care (Stokes et al., 2017). A recent systematic review highlights significant challenges to delivering universal TIC education to providers once they have entered practice (Huo et al., 2023). This underscores the importance of integrating trauma-informed education into the undergraduate program. Unfortunately, undergraduate nursing students have limited or no access to TIC education (Li et al., 2019), and little is known about how best to educate nursing students about TIC before they enter professional nursing practice (Elliott et al., 2024). In particular, the experiences of nursing educators and learners have not been explored, thereby perpetuating a gap in nursing education (Elliott et al., 2024; Li et al., 2019).
Given the growing evidence about the impact of TIC education on practice (Coyle et al., 2019; Niimura et al., 2019; Rodger et al., 2020) and the relationship between using a trauma-informed approach and patient experiences and outcomes (Chafouleas et al., 2016; Ford-Gilboe et al., 2018; Purkey et al., 2020; Ross et al., 2025; Stokes et al., 2017), it is important to understand how to prepare ETP nurses to apply trauma-informed practices (Li et al., 2019). Academic nurse educators should be equipped with evidence-based resources to deliver curricula that prepare ETP nurses to provide safe, competent TIC (Ponic et al., 2016; Stokes et al., 2017). Knowledge of the most effective methods and factors influencing its implementation remains limited (Elliott et al., 2024). Given the very high community prevalence of trauma exposure and high rates of service use in health care settings, this limited knowledge stands in the way of preparing nurses who are equipped to meet the unique needs of clients who experience trauma (Huo et al., 2023). The purpose of this interpretive descriptive research study was to describe and interpret the perceived facilitators and barriers of nurse educators in Ontario, Canada, regarding TIC integration in undergraduate nursing curricula.
Method
This research study used an interpretive descriptive approach situated within a constructivist paradigm. Constructivist research methodologies help to understand the meanings of experiences, informing and improving health care practice (Burns et al., 2022). Interpretive description is a qualitative research approach with epistemological roots within nursing science (Thompson-Burdine et al., 2021). The inductive and pragmatic orientation of interpretive description supports the rigorous exploration of applied clinical and educational problems (Hunt, 2009; Thorne et al., 2004) and the generation of practical insights that can inform and enhance nursing education and practice (Thorne et al., 2016).
Theoretical Framework
This study was guided by transformational learning theory (TLT). Developed by Mezirow, 1978, Mezirow (1991) and influenced by Freire’s (1970) concept of critical consciousness, TLT emphasizes learners’ capacity to critically examine and act upon the social, cultural, and structural forces shaping their perspectives (Dirkx, 1998; Tsimane & Downing, 2019). Transformational learning involves developing awareness of how lived experiences shape beliefs and assumptions and engaging in praxis to foster change (Freire, 1970; Kitchenham, 2008). Freire (1970) conceptualized this process as emancipatory, enabling individuals to become agents of change. Building off this work, Mezirow (1991), Mezirow, 2000, Mezirwo, 2018further conceptualized transformative learning as a process of meaning-making through critical reflection and self-reflection, whereby individuals revise their frames of reference. This process challenges existing beliefs and supports the development of more inclusive and reflective perspectives, shaped by both individual reflection and broader social contexts (Mezirow, 1991), Mezirow, 1996. As a pedagogical approach, TLT facilitates perspective transformation through reflection and dialogue, leading to sustained changes in beliefs, values, and practice (Tsimane & Downing, 2019; Mezirwo, 2018). TLT is particularly well-suited to this study as it has a central focus on critical self-reflection, which provides a robust foundation for developing the reflexivity required for TIC. Its emphasis on perspective transformation prioritizes shifts in underlying beliefs and assumptions, aligning with the need to move beyond procedural competence toward relational, trauma-informed practice (Mezirwo, 2018).
Recruitment
Following research ethics board clearance at the University of Windsor [REB# 24-086], recruitment postcards were mailed to eligible nurse educators who had consented to the College of Nurses of Ontario sharing their contact information with researchers for potential research participation (n = 1156). Recruitment materials were also posted on professional association social media sites, and links were provided to members via email campaigns. An initial recruitment survey, in the form of an online questionnaire, was designed using the Qualtrics XM® software. Purposeful sampling, a form of non-probability sampling, was employed to solicit data from individuals who are especially knowledgeable about or experienced with a phenomenon of interest (Thompson-Burdine et al., 2021), while convenience sampling recruited a sample that is accessible and close at hand, which is helpful in the early stages of documenting a phenomenon (Thorne, 2016).
Participants
Eligible participants included nurse educators, defined as anyone who has been employed as an educator for at least two years in a CNO-approved undergraduate nursing program in a College or University setting. Nurse educators could be full-time, adjunct, or sessional faculty, or clinical/lab instructors. Participants were limited to Ontario because all participants practiced in the same provincial context and were licensed under the same professional standards and ETP competencies (CNO, 2019). A purposive and convenient sample (n = 145) of nurse educators in Ontario who spoke English and had at least two years of experience teaching in baccalaureate nursing programs were invited to participate in the recruitment survey. This initial recruitment survey facilitated theoretical sampling for the next phase of qualitative data collection by identifying diverse participant experiences and ensuring representation from equity-deserving groups of nurse educators (Thompson-Burdine et al., 2021).
Theoretical sampling was used to explicitly build on evolving theoretical variations produced from the initial survey and invite participants who consented to participate in follow-up semistructured qualitative interviews conducted via Microsoft Teams® (Roberts et al., 2021). Theoretical sampling was directed toward generating data through the strategic selection of participants whose views and experiences can add meaning to, illuminate, and, in some cases, help explain the research phenomenon (Cleary et al., 2014; Conlon et al., 2020). The perspectives of clinical instructors or adjunct faculty have largely been excluded from the literature on TIC and its integration to date (Elliott et al., 2024); therefore, clinical instructors and adjunct faculty from colleges and universities across Ontario were strategically recruited to help address this gap in the literature. Interviews were conducted in an interactive, dialogic manner (DeVault & Gross, 2011; Hesse-Biber, 2007) with nurse educators who represented diverse ages, ethnicities, years of teaching, and practice. From the online survey, 28 nurse educators were recruited to participate in qualitative interviews to further investigate the barriers and facilitators to integration of TIC into undergraduate education.
Data Collection
The ten stages of the TLT (Mezirow, 1991) were mapped to the research questions and used to develop the semistructured interview guide (Supplemental Material 1). Data were collected from nurse educators (n = 28) until there was evidence of sufficient depth, richness, detail and coherence in the findings to make the interpretations and conclusions relevant and credible (Morse, 1999; Thorne, 2020). Data collection continued until the dataset was sufficiently rich and diverse to capture a meaningful range of educator experiences relevant to the study purpose (Thorne, 2016). Interview transcripts were shared with a faculty supervisor as a fidelity check and to enhance the trustworthiness of the findings generated (Hunt, 2009; Thorne, 2016). Participants were provided with a $20 gift card as compensation for their time.
Data Analysis
Braun and Clarke’s (2022) approach to reflexive thematic analysis was used to identify, analyze, organize, describe, and generate themes in the data. When rigorously employed, it is known to produce trustworthy findings (Braun & Clarke, 2022; Nowell et al., 2017). Data analysis was conducted concurrently with data collection to enable generated insights to inform subsequent participant interviews (Stokes et al., 2017). Reflexive thematic analysis began with data familiarization and proceeded to a rigorous, systematic coding process, followed by the exploration, development, review, and revision of themes (Braun & Clarke, 2022). Rather than imposing predetermined categories, an inductive approach was used to allow category labels and conceptual groupings to be generated naturally from the data as insights evolved. This process was guided by broad, reflexive questions such as “What am I learning about this?” which supported ongoing analytic openness and flexibility (Braun & Clarke, 2022; Thompson-Burdine et al., 2021). Data were sorted by coding category using NVivo 14®. Data in each category were examined for what they indicate about the concept they represent, using malleable and in vivo coding to ensure validity (Morse, 1994).
Rigour
Within interpretive description, four additional criteria, epistemological integrity, representative credibility, analytic logic, and interpretive authority, have been developed to evaluate rigour (Thorne, 2016, p. 96). Epistemological integrity was achieved through alignment between the research questions, methodology, and theoretical scaffolding (TLT), which informed the study design and analytic approach (Thorne, 2016). Records were also kept of raw data, field notes, transcripts, and a reflexive journal to help systematize, relate, and cross-reference data and report the research process (Braun & Clarke, 2022). Representative credibility was supported through purposeful sampling of 28 nurse educators across theory, lab, simulation, and clinical contexts, and through semistructured interviews supplemented by field notes and analytic memos (Yous et al., 2019). By providing a documented audit trail, the researcher’s decisions and choices regarding theoretical and methodological issues, along with the supporting rationale for those decisions, are evident (Koch, 1994). Researchers maintained records of raw data, field notes, transcripts, and a reflexive journal to systematize, relate, and cross-reference data and to report the research process (Braun & Clarke, 2022). After a prolonged data engagement period (June-December 2024), the data were sorted (January-February 2025) using a structured codebook using NVivo 14. See Figure 1 for a snapshot of the evolving coding structure for two themes. Coding tree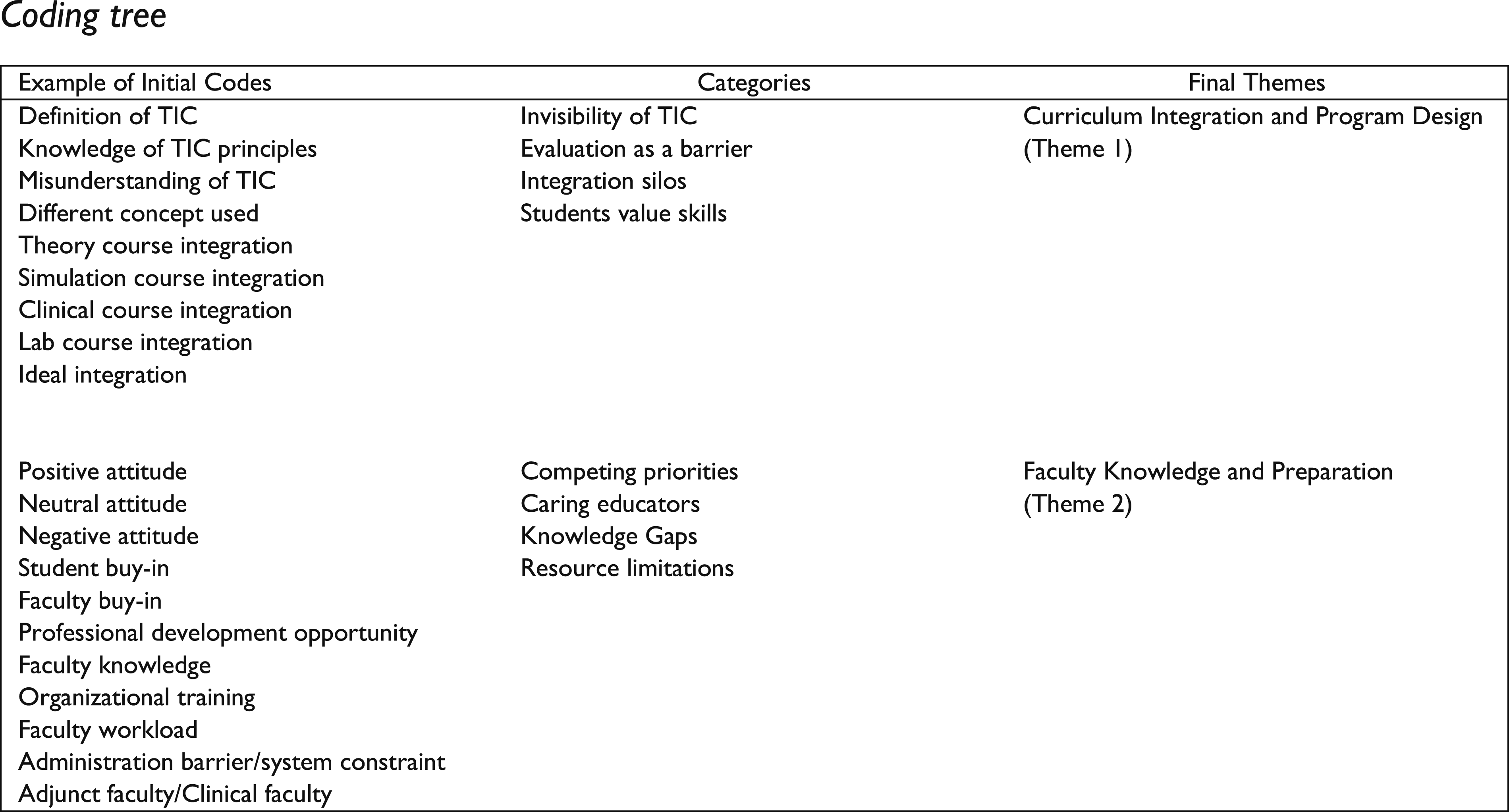
Analytic logic requires reflexivity and holds that researchers are transparent about the decisions they make when transforming data into findings (Braun & Clarke, 2023; Thompson-Burdine et al., 2021). Field notes and memos recording impressions and insights about individual transcripts were maintained throughout the analysis to foster self-reflexivity (Heaton, 2004). Finally, interpretive authority is an assurance of trustworthiness that should account for bias or disciplinary hardwiring and consider how these factors impact interpretation and the generated findings (Thorne, 2016, p. 225). Researchers paid considerable attention to engage in self-reflexive practice through journaling and regular check-ins with faculty supervisors to avoid perpetuating the silencing of less powerful voices throughout this process with constant reflection, raising of critical questions, and considering all interpretive options (Braun & Clarke, 2022; Denzin & Lincoln, 2017; Hunt, 2009; Thorne et al., 2014).
Results
Participant Demographics (n = 145)
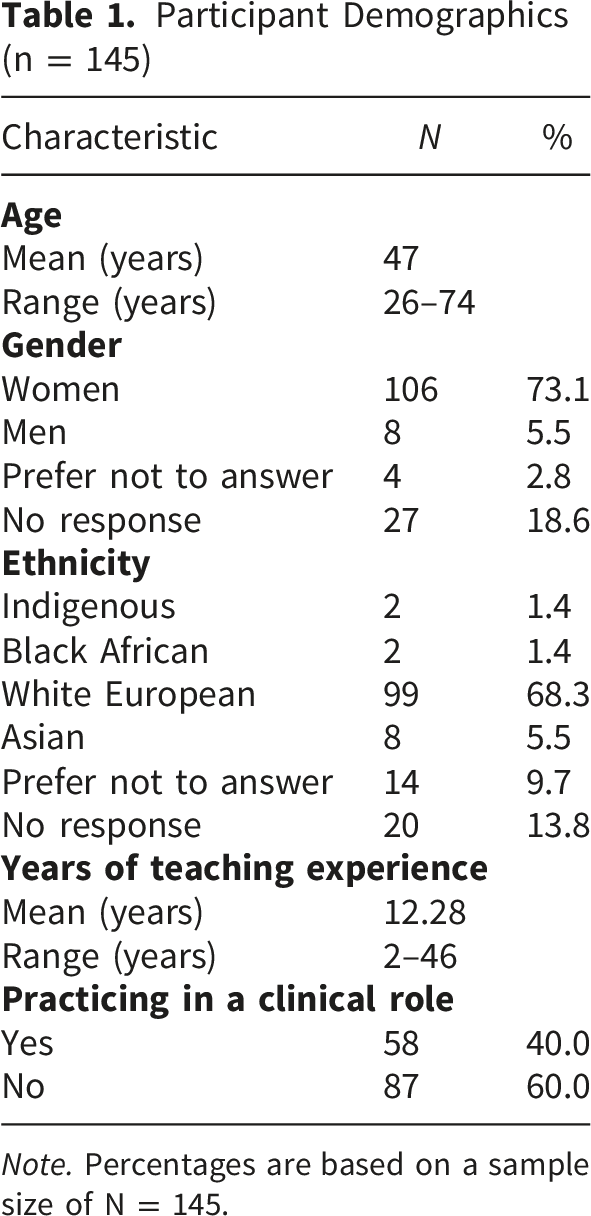
Note. Percentages are based on a sample size of N = 145.
Four major themes were generated from the qualitative analysis and presented here: 1) Curriculum Integration and Program Design, 2) Faculty Knowledge and Preparedness, 3) Innovative Pedagogical Teaching and Learning Strategies, and 4) Systemic and Administrative Supports. In this paper, we present findings on the facilitators and barriers to integrating TIC into undergraduate nursing education.
Theme 1: Curricular Integration and Program Design
TIC is often embedded only superficially, “hidden,” or “invisible” within broader topics (e.g., cultural safety, social determinants, psychological safety) rather than being distinctly and consistently integrated throughout the curriculum. TIC was described as unevenly distributed across the curriculum, often appearing implicitly, sporadically, or in isolated courses rather than as a unifying pedagogical approach.
This resulted in a pattern where TIC was present but not always visible, explicit, or consistently reinforced across learning contexts. Often, there was a continuum of understanding of TIC principles. Participants described how TIC concepts were often embedded but not explicitly named, with one educator noting that it was “kind of masked with other things… like cultural safety or communication” (Participant 25) and not clearly identified as TIC within curriculum documents. Due to the content-rich curriculum, TIC often struggled to secure dedicated curricular space and align with existing coursework. Ultimately, this led to delayed exposure in learning environments and a reliance on checkbox evaluations that may not capture deep, applied understanding. TIC was frequently concentrated in later courses, limiting early exposure. One educator explained that students “don’t really become introduced to it until like year three…and then they’re a little bit more aware of it” (Participant 1). As a result, TIC was encountered as something peripheral rather than foundational. Within this first theme, no facilitators were identified, but three barriers were generated and will be presented next.
Conceptual Invisibility and Definitional Inconsistency in Curricula
This barrier to implementation was evident across participants’ accounts. While overall, all nurse educators interviewed (n = 28) endorsed the inclusion of TIC within Ontario undergraduate nursing programs, they expressed concerns that existing curricula do not explicitly address TIC. The absence of a clear, shared definition among nurse educators was viewed as a significant barrier to its integration, potentially limiting a consistent understanding of the concept. Furthermore, the lack of intentional curricular integration resulted in TIC being retrospectively incorporated into courses rather than systematically embedded.
Given the continuum of TIC conceptual understanding among nursing educators, many terms are used interchangeably (e.g., psychological safety, cultural safety, social determinants of health, trauma- and violence-informed care). When discussing their role as a curriculum committee member, one educator said, “at that level of governance, we’re not calling it that.” (Participant 7). Another nurse educator agreed that the concept is not explicitly identified or integrated, saying, “I don’t see its inclusion explicitly, but I see a lot of people talking about classroom safety”. Another educator stated, “I think that I might not say this is trauma-informed care, but all the time, every time I highlight it, when I tell a story that goes with whatever I’m teaching, it’s always embedded in there, right?” (Participant 25).
TIC content ultimately became hidden or “masked”, making it invisible in coursework. Nurse educators described TIC as being embedded within broader curricular topics, rendering it invisible: “There’s no like [TIC] framework that we teach them specifically and it’s kind of just like integrated throughout. I don’t know if we have like a single lecture that’s just like all about trauma-informed care, but yeah, we try to integrate it.” (Participant 11).
Reductionist Learning and Evaluation Limit Curricular Integration
Evaluating competency in TIC was described as challenging in theory and practice-based courses. Most educators (n = 24) viewed current evaluation methods (e.g., rubrics, skill checklists, reflective assignments) as ‘tick boxes’ and insufficient to evaluate the depth of required understanding and application of TIC assumptions and principles, potentially leading to a “one and done” mentality regarding TIC integration into theory courses. Without the shared definitions, rubrics drift toward reductionist checklists. A shared language enables criteria that capture the application of learning (e.g., communication, safety, choice) rather than mere mention. Participant 21 problematized this approach: We take things in their little boxes. Boxes of knowledge, and we deliver it, like we deliver Med/Surg...and I'm going to give you the lecture, and it's going to be very clear because this is what it looks like. The symptoms and tick, tick, tick, tick, tick. You know it, fine, here are the interventions, but trauma and [TIC] is not that! It's much more complex.
Another nurse educator highlighted the challenges with authentic evaluation, stating, “Yeah, and a prof[essor] could have two slides in their entire semester on this concept. Ticked! Submit that to the director and say yep, I did the work well! But did you? Was it authentic?” (Participant 7). Half of the nurse educators (n = 14) cautioned that integrating TIC within their courses could lead to or reinforce a reductionist approach with a “checkbox” mentality, where key principles are referenced but not deeply explored or applied in practice. For example, a nurse educator stated, “…so it’s not that you just presented it all in one class and check off a box! It’s meant to come in as the program evolves.” (Participant 12).
The ‘tick-box’ concerns were also evident in practice-based courses. Participant 15 viewed checklists supporting a reductionist approach in nursing practice and barriers to implementation of TIC, stating, “it was just a checklist, I completed the boxes, I ticked it off…but what was missing a lot was the idea of the relationship, the therapeutic relationship.” (Participant 15). Many educators (n = 17) highlighted the fact that assessment strategies, especially in the clinical or experiential lab setting, tended to focus on skills acquisition rather than evaluating the application of TIC principles into clinical practice, leading to a potential disconnect for students. One new educator acknowledged, “it’s frustrating that our clinical evaluations are reduced to checklists…it may be ‘done’ on paper, but they don’t capture whether students have truly internalized a trauma-informed approach.” (Participant 4).
Nevertheless, a few nurse educators (n = 9) felt that a checklist is a good starting point for novice learners to help them apply TIC in patient interactions. For example, one educator who concentrated on Indigenous nursing education advocated, “you have to bring it to the surface. But I do wonder about a tick box situation even the concept of reconciliation, it can be perceived as a tick box. I think it’s a good step forward, but it’s not where it should end.” (Participant 14). A simulation educator suggested integrating reflexivity into current evaluative measures to reinforce TIC and its application. “I think having reflective practice is important…right now, we’ve gotten to a particular point in education where I feel like we’re doing a lot of box checking.” (Participant 17).
Competing Priorities in an Overloaded Curriculum
Many faculty members (n = 18) commented on the challenge of effectively teaching the ETP competencies within the time available in very overloaded, highly regulated curricula that often prioritize other areas, such as acute care and NCLEX-RN preparation. One educator with decades of teaching experience highlighted, “the curriculum is so packed at this point, how do you sort of, squeeze it in?” (Participant 23). Another participant echoed this concern, “we treat our classrooms like a container where we just pour content…but our students need to have the capacities, especially related to TIC, and use the knowledge to survive when they go to clinical.” (Participant 20). In addition to the volume of content, Participant 21 emphasized the fast pace of delivery: “the stuff that we have to teach in four years is incredible. We’re just piling on knowledge at a rapid speed than human brains can cope with.” This created challenges for newer educators, who were rapidly adjusting to teaching a very overloaded curriculum and balancing this with meeting ever-increasing student needs, and professional obligations: “And then, yeah, you go to a conference and education, then it’s like fire hose of just things that should probably be in the curriculum.” (Participant 5).
Theme 2: Faculty Knowledge and Preparedness
A central pattern across this theme was that the integration of TIC was highly contingent on individual educators rather than systematically supported within programs. As such, TIC was often enacted through personal commitment, prior experience, or interest, rather than through shared expectations or standardized approaches. There was an evolving consensus that, because most clients and students experience traumatic events, the principles of TIC should be applied in learning environments to equip students to practice. Educators highlighted how some educators intentionally integrated TIC through their own passion and experience, often extending beyond formal curriculum expectations. However, this led to variability, with others unsure how to incorporate TIC. This was further compounded in clinical settings, where part-time instructors often lacked preparation, leading to inconsistent expectations and implementation. As one participant reflected, “some faculty… don’t understand it… they’re very focused on like pharmacology… so where would you bring [TIC] in?” (Participant 25). Although most educators had a positive attitude toward understanding TIC as a curricular concept and toward its integration in both the recruitment survey and in follow-up qualitative interviews, they lacked formal training and felt uncomfortable incorporating TIC principles.
Passionate Educators
The role of enthusiastic, caring faculty who are personally invested in TIC is a recurring theme in the data. Although some educators (n = 14) suggested working groups, think tanks, collectives, roundtables, or supportive collaborations among like-minded educators, other faculty members were concerned that this would add additional workload or responsibilities without the required institutional support. Despite this, educators’ passion and commitment to TIC are perceived as major facilitators in driving curriculum enhancements in the face of institutional demands. Six educators promoted the idea of having a faculty champion or leader, or a group of educators who champion the integration of TIC into the curriculum. I think if you have a champion truthfully of [TIC] practices, that can be helpful. If you have somebody who is passionate about that within your faculty, passion really breathes life into those spaces because people like wow, this person's so excited about this as a concept that it's driving joy! And like and at that's so translatable I've found and I think maybe that's why, because [TIC] is really important to me in my work and space. I mean I buy into it! And I really want people to understand TIC because I think personal history, my experience as a nurse has been really driven like this is you have no idea how much this effects everything. (Participant 19).
The majority of educators (n = 20) articulated the desire to move from teaching about TIC concepts toward teaching from a trauma-informed pedagogical perspective, with role modelling as a critical step. “This is something that we want to embody…we want to make sure we’re role modelling for our students so when they go out and they graduate they can be trauma-informed practitioners and it’s just in their being, it’s their essence.” (Participant 13). Another educator, extremely passionate about TIC stated, “It’s a way of being. I just get excited and passionate about it...it’s revolutionary to me. I talk about [TIC] and how this can be game-changing for humans…I think for me it’s just really embodying it.” (Participant 9). A third educator described the need for more role modelling of TIC in the clinical setting: I need to do a bit more role modelling in clinical. Pointing it out with patients or with students, posing questions to them about “why?” why do you think the patient responded that way, why did they react that way? And just kinda getting them to look at it from that perspective. To engage them in those conversations and maybe even just reflect. (Participant 6).
Most faculty members valued graduating students who are both capable and able to apply TIC concepts in patient care interactions. One experienced educator accurately described it in the following terms, “because if you’re not graduating a compassionate and safe nurse…do you think they will do a good job?” (Participant 3). Another agreed with this ideal and said, “so, if the end goal is that we have trauma-informed practitioners, then it kind of needs to be in everything.” (Participant 13). Another experienced educator seconded this statement, suggesting, “we have to start thinking differently about what we want our ends to be.” (Participant 25).
Nurse Educator Knowledge Gaps
Most educators (n = 21) reported that the absence of TIC training was a significant barrier to their work and that it resulted in a lack of confidence in teaching TIC concepts. “In terms of faculty comfort, when you’re talking about trauma-informed care, you’re getting into conversations that might not be comfortable, or maybe getting into conversations with faculty who don’t feel equipped to manage.” (Participant 1). Another faculty member agreed that the lack of effective training discouraged faculty from stepping outside their comfort zone, indirectly reinforcing the status quo in nursing education. “It’s easier to just keep the same thing status quo. I think there’s comfort zones too. I think comes back if somebody doesn’t even understand that in trauma-informed care can be something as simple as just relearning language or being sensitive with language. They don’t want to you know, tackle it. They’re uncomfortable.” (Participant 18). Among those surveyed in the phase-on survey, 83% (n = 121) were familiar with the concept of TIC; however, only 26% (n = 31) had received formal training, and only five (4%) reported feeling ‘very confident’ in their ability to teach nursing students to practice from a TIC framework.
Insufficient time was universally viewed as a barrier to engaging in profound, reflective scholarship or professional development that would enhance TIC education. Limited resources and increasing workloads meant the nurse educators had fewer opportunities to pursue specialized TIC training. “There’s nothing, no continuing development, no professional development, it’s non-existent.” (Participant 24).
Clinical educators (n = 8) discussed the gaps in onboarding and training, suggesting that their orientation primarily covered administrative basics (such as payroll, learning management systems, and human resources), but lacked sufficient support for effective clinical instruction, let alone integration of TIC. For example, one clinical educator stated, “honestly, that is not something we were ever given as faculty, any extra training. It’s all about the urgent stuff…policy and program development takes up all our time.” (Participant 10). Another clinical educator echoed this sentiment, “yeah, high turnover, new staff. I was on-boarded in 2020, and because of COVID, I literally got like an eight-minute like, here you go! And I was like, okay, I gotta figure this out!” (Participant 6).
When nurse educators were asked if they would like to receive more training on TIC, 68% agreed or agreed strongly with the need for formalized TIC training for all faculty members. As a result of these gaps, some faculty went above and beyond to learn about TIC through external courses or graduate-level work on their own, without institutional support. One educator who engaged in “off the side of their desk” training said, “I think that’s the bigger issue. Is management allowing these [TIC] discussions? Like where is the training? There’s no training, especially for educators, there’s none!” (Participant 18).
Theme 3: Innovative Teaching and Learning Strategies
A gap exists between how TIC is taught in theory and how it is applied in clinical placements, highlighting the siloed integration of TIC, the primary barrier in this theme. Faculty consistently reported that if TIC is not properly integrated, students may miss opportunities to develop essential communication and self-reflection skills needed for sensitive clinical interactions. Participants described using interactive and creative strategies, such as case studies and storytelling, to make learning more meaningful. As one educator explained, “I see a lot of learning come to life when I do that… actually working through these case studies” (Participant 11), highlighting how applied approaches support deeper understanding. Similarly, fostering self-awareness was seen as foundational, with educators encouraging students to reflect on their own experiences: “it’s all about reflection and that self-awareness” (Participant 10). Collaboration among faculty further supported these practices, with participants describing the value of shared dialogue: “all of us were kind of brainstorming together… what a fantastic idea” (Participant 23), illustrating how collective reflection facilitated innovation in teaching. As a result, while TIC could be enacted in rich and meaningful ways at the classroom level, these practices remained localized and difficult to sustain across the broader program or mapped curriculum. Institutional structures also reinforced superficial engagement. Participants described accreditation and curriculum requirements as promoting a “checkbox mentality… like, ‘we teach it here, we teach it here’… but are we doing it to any depth?” (Participant 2).
Creative Pedagogical Strategies
Nurse educators emphasized the need to create space in curricula for students to process, reflect, and build upon their self-awareness, as they viewed this as the foundation for trauma-informed practice. Many educators (n = 22) suggested the need for creative teaching methods, such as simulations, case studies, storytelling, and varied assessment modalities, to foster self-awareness as a pathway towards understanding TIC. Rather than relying solely on traditional didactic lecture formats and traditional evaluative strategies, these educators employed relational, experience-based learning and alternative assessments that catered to diverse learning styles and encouraged active reflection. They were viewed as “opportunities…to foster a safe space for students to be their authentic selves and feel safe to ask questions...spaces where people can be authentic and truly learn.” (Participant 7). For example, one nurse educator created a unique opportunity to embed simulation experience a community experience in a year-two clinical placement. Educators also described arts-based strategies as ways of enhancing student learning and facilitating challenging conversations about personal values, biases, beliefs, nursing practice philosophies, and/or reflections of self. For example, one educator remarked, In first year, we do this mask making experience. The students lay down and they have to put a plaster mask on their friend or on their partner. And it's a very vulnerable situation to be laying there. They're trying to like shape it around you. It's messy…It's all about communicating and relational practice. They end up painting the outside of the mask how society sees them and then the inside of the mask is how they see themselves. (Participant 4).
Storytelling and reflection were repeatedly emphasized to make theory applicable, fostering moments of “aha” when students see their own experiences reflected in the learning materials. One nurse educator offered self-assessment as a skill for building competency in TIC: One of the things that I do wherever possible is trying to promote student evaluative judgment. Self-assessment is something that's easy [to implement], even in larger classes! Integrate in different ways that will help students develop that ability and maybe the whole assessment isn't super authentic, but at least they're developing that skill. (Participant 2).
Collaboration With Colleagues
Several educators (n = 8) discussed the positive impact of being part of a group that regularly discusses and shares innovative ideas. Regular discussions and joint planning sessions with colleagues (e.g., faculty meetings, curriculum conversations, co-teaching or shared teaching, and shared curricular spreadsheets) facilitated the integration of different perspectives and bridged gaps between TIC theory and practice. One educator noted, “I think when we collaborate, whether in small group discussions or in our team meetings, it really moves trauma-informed care into praxis…we’re all bouncing ideas off each other so that our approaches become more robust and nuanced.” (Participant 27).
Collaboration was also viewed as vital in supporting clinical instructors, where shared case studies and simulations can build a common language around trauma-informed practices. Simulations and other experiential learning strategies were suggested to support faculty collaboration in incorporating TIC, especially in the face of a current scarcity of clinical placements. One educator suggested that collaboration could be a way to integrate clinical instructors into the program and offer additional training or opportunities to learn about TIC within the lab or simulation environment: “I feel like there’s a lot of room for growth [in simulation] and so maybe incorporating TIC is a good strategy.” (Participant 2).
Most educators (n = 16) discussed opportunities for mentorship among faculty and suggested co-teaching or shared teaching as opportunities for mentorship. An experienced educator discussed the value of collaborating with colleagues to share teaching assignments and learn from each other in the process: It's a work in progress for sure. I think we're getting there, and I think you know, every time we teach the course, every time we come together as a faculty, and we're very lucky. We have seven people attached to the course now, so there's a lot of unique perspectives! (Participant 27).
Fragmented Integration
The analysis revealed that TIC is frequently taught in isolation from the rest of the curriculum, and when the nurse educators attempted to include TIC in their curricula, it was often integrated within teaching silos. One nurse educator expressed, “So we definitely made sure that [TIC’s] there, but like in terms of like the infusion throughout the entirety of the curriculum, I think like that’s very specific to the individual professors.” (Participant 11). The definitional plurality (TIC, TVIC, trauma-informed pedagogy) further propagates the invisibility of TIC in course plans and fragmented assessments, which students experience as ‘add-ons’ rather than a program standard. Participant 26 asserted: “It’s not an add-on, it has to be foundational to the approach of everything, right. So, it’s a big change! So, [educators] need to be on board wholly, completely.” Another nurse educator viewed TIC as an easy concept to neglect or deprioritize in a curriculum, stating, “[TIC] might be one of those principles that maybe falls to the wayside, and it’s like, oh, yeah, I learned about that in whatever year, but it’s not necessary for me to pass the NCLEX.” (Participant 4).
Clinical, lab, and adjunct educators (n = 23) reported not being introduced to or involved in curricular design, leading to inconsistent application of the concept in patient care settings. One experienced nurse educator summarized the problem beautifully, stating: “structurally, we have a much bigger problem. I worked as a clinical instructor for five years…there was absolutely no connection to the University. It’s, ‘here’s your badge, here’s your paycheck,’ it’s so precarious…how do you onboard every semester?” (Participant 7). With evaluations mostly dependent on individual clinical instructors, there was variability in how TIC was assessed. Participant One, a program coordinator, expressed frustration with the inconsistent evaluation of TIC in clinical placements. That’s tricky, right? That’s really tricky, because with the year two clinical placements, students wrote a reflection about [TIC] and it was up to their clinical instructor to evaluate, but we found that the clinical instructors didn’t know what to do with this, because it was seen as separate.
Theme Four: Systemic and Administrative Supports
Beyond individual and curricular factors, the integration of TIC was profoundly shaped by broader institutional, structural, and systemic constraints that limited the capacity for meaningful implementation. Many educators noted the lack of direction from senior leadership (e.g., Chairs, Associate Deans, Deans, and administrators) regarding the inclusion of TIC as a required component of the curriculum. Without institutional mandates and administrative support, TIC integration depends on individual initiative rather than systemic support. Specifically, participants described significant resource constraints, including limited time and large class sizes, which made relational teaching more difficult. Increasing workload further compounded these challenges, with faculty describing how TIC-related work often occurred “off the side of your desk” (Participant 1). Policies and administrative expectations sometimes conflicted with trauma-informed principles, particularly when flexibility was required, with one educator questioning “where is that wiggle room?” (Participant 12) when trying to support students experiencing difficulties. In this context, leaders were often tasked with ensuring compliance with external standards, which could inadvertently be prioritized over meaningful engagement with TIC. This tension highlighted how institutional policies could both enable and constrain trauma-informed approaches, depending on how they were interpreted and enacted. Collectively, these systemic constraints created conditions in which TIC was difficult to embed deeply or consistently, reinforcing its partial, fragmented, and often surface-level integration across programs. Although leadership was referenced as influential, educators suggested that leaders themselves often had limited autonomy within these broader systems.
Institutional Leadership and Structural Supports
Supportive school leadership at both the departmental and institutional levels was considered critical for advancing TIC’s integration into nursing education. Truly endorsing student-centred learning and providing the infrastructure, such as adjusted workload models and access to professional development, were viewed as ways to foster a culture in which TIC can flourish. Although some educators (n = 12) felt they consistently had to “do more with less,” supportive leadership, time and resources were considered essential at all levels of the academic institution for TIC integration. One nurse educator highlighted this: I’m so lucky that my institution is so supportive at, like, up to the College President. I don't know if it's possible without that institutional support…you need people at every level that will support this. You need the coordinator’s support, you need your Dean’s support, you need your [administration]. Without that upstream approach and institutional backing, it’s nearly impossible to implement these changes. (Participant 11).
Another experienced educator agreed, stating, “right now it’s a very patchwork system, where if a professor understands [TIC] then it’s enacted…But at the school level, a faculty level, an institutional level, it’s not a core philosophy that guides us in our work.” (Participant 7). Several educators (n = 14) noted that without supportive leadership, structural and systemic factors, such as collective agreements, increasing workload, limited resources, and the pressure to fulfil multiple curricular demands, would severely limit the flexibility of nurse educators in incorporating TIC meaningfully.
Educators described how system-level policies and workload constraints prevented them from dedicating time to developing and integrating trauma-informed approaches in their theory and experiential courses. Some educators felt that policies are used to justify inflexible teaching methods rather than being critically examined for their impact on student learning and well-being. A novice educator described their attempt to implement a trauma-informed approach to assignment due dates in a large theory course and how they became overwhelmed by the additional workload demands without the necessary institutional support. I think sometimes I would say that you need to do what makes you feel like you can sleep at night and that you've done, you know, the best to and reconcile what are your hopes and dreams and desires are as an educator versus some of those structures and realities that we're within. (Participant 5).
Discussion
Summary of Facilitators and Barriers to TIC Integration
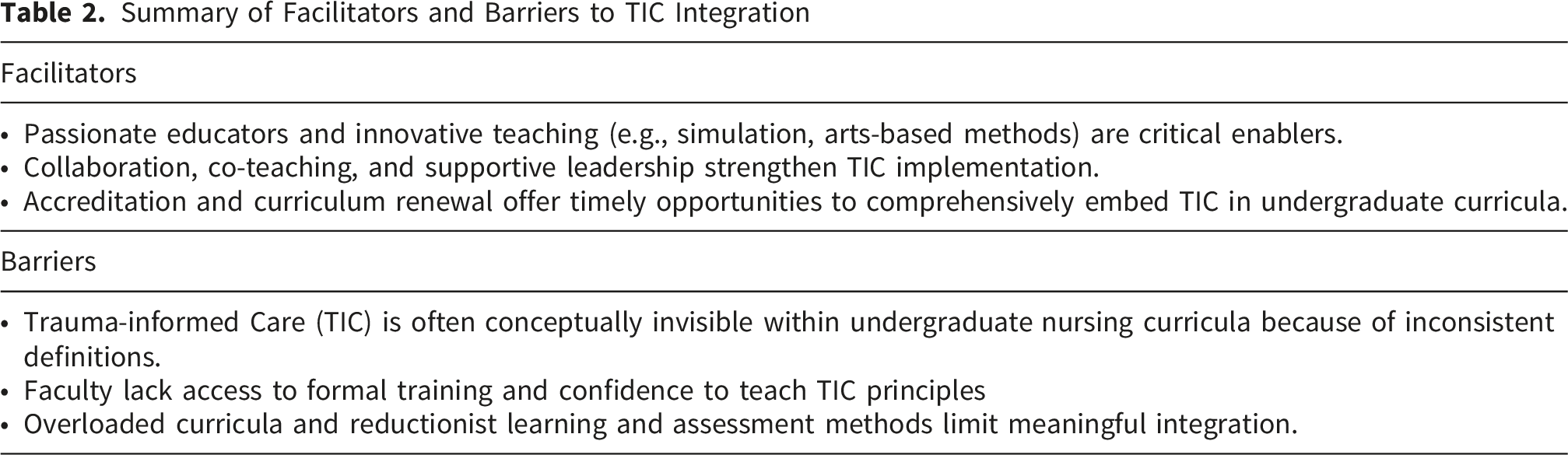
Although this study was conducted in Canada, the findings reflect a broader global need to develop a robust educational framework for embedding TIC in undergraduate and prelicensure nursing education, ensuring that all nurses can apply this approach to care across diverse settings. Where best practices for educational interventions had been unclear and largely unexplored in the existing literature (Burns et al., 2023; Ross et al., 2025), this study is one of the first to investigate the significant barriers and the emerging best practices for integrating TIC into undergraduate nursing education, which has the potential to translate to a global setting. Our findings strongly highlight the importance of integrating TIC into all aspects of nursing education, recognizing that role modelling and a shift in pedagogy are essential to fostering the development of students and future practitioners who can apply these principles in their clinical and future professional practice.
An Imperative to Make the Invisible Visible
A significant barrier identified in our study, the invisibility of TIC in nursing curricula, mirrors the theme of inconsistency and lack of conceptual clarity described in previous research (Cannon et al., 2020; Elliott et al., 2024; Hall et al., 2016; Muskett, 2014; Qin et al., 2025). Without a clear understanding of the core principles of TIC, educators struggle to embed a coherent, intentional TIC framework, which is a significant barrier to meaningful curricular integration. The absence of conceptual clarity may lead to fragmented, siloed integration, in which TIC is reduced to isolated mentions in lectures or assignments rather than woven systematically through curricula (Li et al., 2019; Qin et al., 2025; Wheeler & Phillips, 2021). The lack of formal curricular mapping also reflects a broader trend across nursing programs where TIC is not aligned with course objectives, content delivery, or program outcomes (Kuzma et al., 2022). If nurse educators do not explicitly identify TIC concepts and intentionally integrate them into their courses and curricula, learners will be challenged to fully understand the approach to care and apply it in their clinical settings.
At the time of data collection in Ontario, several nursing programs were undergoing curriculum renewal or developing new curricula, prompting educators to think creatively about integrating ETP competencies. While these structural changes created opportunities for innovation, they also revealed the absence of consistent expectations for TIC integration. This finding underscores the importance of aligning regulatory expectations with meaningful curricular implementation, rather than solely documenting inclusion. A recent systematic review of the current state of TIC in nursing practice and education highlighted challenges related to diversity and the application of TIC theoretical and conceptual frameworks (Qin et al., 2025). This study indicates that TIC is a priority learning area for nurse educators. Nevertheless, there are no accountability measures in Ontario to address nursing knowledge gaps among educators.
A Pressing Need to Address the Educational Evidence Gaps
Our findings are consistent with previous research demonstrating limited consensus on what trauma-informed education should look like when enacted in the classroom (Maynard et al., 2019; Venet, 2023). However, this study contributes a more nuanced understanding of how this lack of consensus translates into practical challenges for educators attempting to operationalize TIC within content-heavy curricula. Recent reviews of the literature highlight a growing body of literature on TIC education frameworks, but also a highly variable curriculum and content delivery method (Bell et al., 2025; Jackson & Jewell, 2021; Mahon, 2025; Ross et al., 2025; Steen et al., 2022). This ambiguity presents significant implementation challenges among educators (Norrish & Brunzell, 2023; Stratford et al., 2020). A recent scoping review of practices for designing, implementing, and evaluating TIC curricula for health care workers included only two articles on best practices in undergraduate nursing education (Burns et al., 2023). Best practices on the integration of TIC remain both underdeveloped and inconsistent across sectors. Despite several theoretical and guidance documents, it is unclear exactly what schools are doing when they say they are using a trauma-informed approach (Maynard et al., 2019). The findings of our study align with the existing literature emphasizing the need for effective learning techniques and trauma-informed educational practices to help students apply TIC skills in clinical settings (Ross et al., 2025; Zarnello, 2023).
Nursing students often lack the confidence and competence to engage with clients experiencing trauma and expressed a need for more practical training, including simulations, case studies, and skill-building exercises, to enhance their ability to apply TIC in clinical practice (Cannon et al., 2020; DeFoor et al., 2024; Qin et al., 2025). Our findings demonstrate a disconnect between what is taught and the intended trauma-informed approach to care in diverse clinical settings. Recent encouraging research suggests that simulation may help students enhance their ability to respond to clients and their TIC skills (Farrell & Sebastian, 2024). While existing research by Pfeiffer and Grabbe (2022) notes the inclusion of TIC in theoretical content, our findings indicate that current evaluation methods often fall short of capturing the depth of students’ understanding or their application in clinical practice. Bell et al. (2025) highlighted that TIC training incorporated hands-on practice opportunities, such as role play, simulations, demonstrations, or patient interviews, received highly positive feedback from learners, with simulations rated as the most beneficial learning strategy. Simulation has been reported as a feasible and effective tool for training medical students to apply TIC in acute care settings (Bell et al., 2025; Lee et al., 2023) and to use TIC principles to improve empathy when caring for equity-deserving clients (Palnati et al., 2024). Our findings suggest an opportunity for nurse educators to align TIC with competencies (Pfeiffer & Grabbe, 2022) while ensuring that students are assessed on these principles and provided with deliberate hands-on learning activities that guide them in applying trauma-informed approaches, thereby linking theory to clinical practice.
Reframing Health Care Practices
New evidence has identified and synthesized findings on barriers and facilitators to implementing TIC in health care settings. In a systematic review, Huo et al. (2023) demonstrated that training health care professionals is more likely to lead to TIC implementation where training is targeted at staff across all levels of an organization, including front-line workers. Our findings are consistent with research that calls for the universal and systematic application of TIC as routine best practice for care by clinicians and within organizations (Burns et al., 2023). Widespread TIC implementation requires institutional policies and procedures that include staff, practitioner, and consumer input (Ross et al., 2025). To fully appreciate the impact trauma-informed approaches can have across an organization, leaders should create standardized policies to inform the change process (Goldstein et al., 2024). When TIC is not routinely role-modelled by experienced health care professionals or embedded within clinical settings, students struggle to connect theoretical knowledge to real-world practice. Therefore, it is essential for educational programs and clinical settings to align their practices, policies, and leadership to consistently role model and implement TIC, ensuring students are adequately prepared to apply these approaches in their professional practice.
Reframing health care delivery by integrating the core principles of TIC into existing clinical practice and processes can enhance everyday delivery of care to clients who experience trauma in primary care settings and emergency departments (Ashworth et al., 2023; Coleman, 2024; Holod et al., 2025). Adequate knowledge of TIC among leadership and providers has the potential to foster a paradigm shift within health care organizations. In this way, organizations would be able to truly tackle the societal, cultural, structural, and organizational inequities that otherwise hinder the delivery of TIC, particularly in diverse and under-resourced settings (Browne et al., 2018; Levine et al., 2021; Ross et al., 2025). A recent targeted needs assessment of interdisciplinary health care workers in Ontario highlighted similar findings to barriers to the effective implementation of TIC in clinical practice (Ross et al., 2025). Their findings demonstrated a critical gap in TIC knowledge and skills among a broad range of health care providers, particularly in the practical application of TIC in everyday clinical practice (Ross et al., 2025). Other research confirms a significant knowledge gap among current health care providers (Bell et al., 2025; Burns et al., 2023). Adopting a multilevel approach that integrates TIC into organizational policies and procedures while engaging the entire workforce is essential for achieving a system-wide transformation. Implementing TIC within an organization’s care practices must not be viewed as additional work, but rather as a reframing of how health care is delivered through the application of TIC principles (Ashworth et al., 2023; Ross et al., 2025).
Implications for Nursing Education
Findings from this study offer recommendations for advancing the meaningful integration of TIC into undergraduate education. Although conducted in Ontario, these findings reflect broader global challenges in undergraduate nursing education, suggesting that nurse educators internationally may be experiencing similar difficulties in consistently and meaningfully integrating TIC into curricula and practice. The integration of TIC into undergraduate nursing education is a shared responsibility, and educational leadership is needed locally, nationally and globally to develop a framework and tools. Involving health care stakeholders in the development and implementation of resources that address provider knowledge gaps and the policies that drive practice is critical. Clarity and visibility of TIC as a curricular concept are priorities, as well as integration and levelling across the curriculum.
First, curriculum committees should prioritize explicit inclusion of TIC content across all years of study, ensuring consistent definitions and learning outcomes that align with professional standards and regulatory competencies. Clear curricular mapping and purposeful levelling of TIC content can promote its visibility and integration within courses and prevent gaps in its application. Best practices include the recommendation to introduce the concept and principles early and progressively build upon the initial introduction as the content is threaded through the undergraduate curriculum. Collaboration among regulatory bodies, accreditation bodies, and nursing education programs may help to ensure alignment with professional standards while fostering shared ownership and innovation in curriculum when integrating TIC. When external regulators and accreditation bodies provide frameworks that compel undergraduate nursing programs to assess and improve the integration of TIC, this creates opportunities to better embed TIC in both clinical practice and classroom teaching. It also creates accountability among nurse educators to explicitly embed, level, and map TIC competencies across their curricula, and to develop processes to enact trauma-informed learning environments.
Second, authentic and contextually relevant teaching and assessment methods should be developed to evaluate students’ understanding and practical application of TIC principles, moving beyond checklists to reflective practice, simulation-based assessments, and interprofessional scenarios. This aligns with best practices in trauma-informed educational frameworks, which emphasize relational pedagogy, student safety, and reflexivity (Bosse et al., 2021; Wheeler & Phillips, 2021). We recommend educators consider creative teaching strategies that motivate learners to apply TIC principles. Creating a universally safe environment by implementing trauma-informed educational practices could create spaces for nursing students to thrive as learners (Wheeler & Phillips, 2021). Open-access teaching resources could enable a global community of practice in which nurse educators can access and share evidence-based materials to support excellence in trauma-informed pedagogy.
Third, faculty development must be strengthened for meaningful integration and application of TIC. Given both the pervasiveness of trauma and the lack of shared definitions, we recommend a threaded, levelled integration across the curriculum with explicit language (i.e., naming TIC when it appears) rather than a single, stand-alone lecture that risks siloing and superficial uptake. Academic institutions should invest in mandatory, ongoing professional development on TIC for all educators, including sessional, adjunct, and clinical instructors, to close the identified knowledge gaps and increase educators’ confidence in teaching and modelling trauma-informed approaches. Supportive leadership is critical to fostering an institutional culture in which TIC is valued and sustained. Embedding trauma-informed principles in the academic environment itself, by creating safe, inclusive, and supportive learning spaces for both students and faculty, can serve as a living model of TIC in action (Elliott et al., 2024). Faculty must be trained to establish classroom practices that promote safe spaces, encourage self-reflection, and provide flexibility to meet diverse students’ needs. A commitment to embedding trauma-informed pedagogical models in undergraduate education may help produce graduates who practice from a trauma-informed lens and advocate for TIC across diverse health care contexts, ultimately advancing equity. In situations where faculty development opportunities, nursing faculty members may wish to consider using their regulatory body’s quality assurance program to expand their knowledge and understanding of TIC concepts and principles.
Implications for Nursing Research
This study highlights the ongoing need for robust empirical research to guide the integration and evaluation of TIC in nursing education. The importance of rigorous implementation and evaluation methods, as well as of understanding the impact of TIC education on patient care outcomes, has been outlined in recent reviews of TIC (Berring et al., 2024; Mahon, 2025; Sherfinski et al., 2021; Wathen & Mantler, 2022). There is broad agreement among clinicians, academicians, and researchers that the lack of outcomes research on TIC is a significant impediment to implementation (Huo et al., 2023; Lewis et al., 2023). More international and collaborative research is needed on how to embed trauma-informed teaching practices into the undergraduate curriculum. Specifically, there is a clear need for more longitudinal follow-up to assess the sustainability of TIC training outcomes and real-world application in clinical practice (Bell et al., 2025).
Future research should develop and empirically test evidence-based teaching strategies and curricular models that systematically embed TIC across theory, simulation, and clinical learning environments. Rigorous studies using validated measurement tools are needed to evaluate the effectiveness of these interventions in improving student knowledge, attitudes, confidence, and, ultimately, patient outcomes. Current instruments are self-report measures that assess the knowledge, attitudes, and practices of TIC (Wathen et al., 2021b). A review of organizational TIC interventions identified similar gaps in the literature, including inconsistent use of validated instruments (Purtle, 2020).
Limitations
This small, qualitative study reflects the perceptions of a purposive sample of nurse educators in Ontario, Canada. While theoretical sampling and diverse recruitment strategies were employed to maximize variation, the findings may not be generalizable to other provinces, countries, or nursing programs with different regulatory frameworks, cultural contexts, or institutional structures. The relatively homogenous sample represents a limitation, as it may constrain the inclusion of diverse perspectives and inadvertently perpetuate dominant narratives within nursing education. Given the strong connections between TIC and health equity, future research should intentionally engage educators from equity-deserving groups to better understand how TIC is conceptualized and implemented across diverse contexts. Participants self-selected for participation in this study, and many educators expressed personal or professional interest in TIC, which may reflect greater awareness or motivation to integrate TIC into undergraduate nursing programs. In the future, analyses of curriculum documents could provide deeper insights into how educators operationalize TIC in teaching contexts. Finally, this study focused primarily on nurse educators’ perspectives. While TLT offers a valuable lens for understanding how nurse educators and students may shift their perspectives toward trauma-informed practice, its individual-level focus and limited guidance on implementation highlight the need to consider broader structural and pedagogical factors that influence TIC integration. The views of students, administrators, and clinical partners were not directly explored in this phase, but are critical for a comprehensive understanding of the barriers and facilitators to effective TIC integration. Future studies should include these key voices to enrich the findings and inform best-practice recommendations.
Conclusion
This study contributes important new knowledge about the barriers, facilitators, and opportunities for integrating trauma-informed care into undergraduate nursing education in Ontario. Despite growing recognition of trauma’s impact on health, the meaningful integration of TIC remains limited, conceptually unclear, and inconsistently applied. Nurse educators are well-positioned to lead change, yet many lack the training, time, and institutional support to effectively embed TIC across curricula. Learners struggle to apply TIC principles when these are not clearly taught or consistently modelled in clinical environments. Embedding TIC into nursing education must move beyond isolated lectures or assignments to become a foundational global framework for practice. This requires clear curricular mapping, sustained faculty development, and leadership support to create a trauma-informed academic culture. Accreditation standards and curriculum renewal processes offer timely opportunities to embed TIC systematically and with accountability. Continued research is needed to evaluate implementation strategies, identify best practices, and assess the impact of TIC education on student outcomes and clinical practice. Establishing TIC as a core international competency in nursing education is essential to preparing future nurses to provide equitable, compassionate, and safe care across diverse health care settings.
Supplemental Material
Supplemental Material - Facilitators and Barriers to Integrating Trauma-Informed Care in Undergraduate Nursing Education
Supplemental Material for Facilitators and Barriers to Integrating Trauma-Informed Care in Undergraduate Nursing Education by Rachel A. Elliott, Edward Cruz, Sherry Morrell, Adrian Guta, and Kathryn Pfaff in Global Qualitative Nursing Research.
Footnotes
Ethical Considerations
We received ethical clearance from the University of Windsor REB# 24-086.
Consent to Participate
Please include any participant consent information under this heading and state whether informed consent to participate was written or verbal. Both written and verbal consent were obtained from participants prior to participation. No generative AI was used for the purpose of writing this manuscript.
Consent for Publication
We have not submitted this original manuscript elsewhere, nor have we published the data used in this manuscript anywhere else. No generative AI was used for the purpose of writing this manuscript.
Author Contributions
Rachel Ann ELLIOTT: Writing – review & editing, Writing – original draft, Visualization, Validation, Supervision, Software, Resources, Project administration, Methodology, Investigation, Formal analysis, Data curation, Conceptualization. Edward CRUZ: Writing – review & editing, Methodology. Sherry MORRELL: Writing – review & editing. Adrian GUTA: Writing – review & editing. Kathryn PFAFF: Writing – review & editing, Writing – original draft, Methodology, Formal analysis
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.