
Abstract

Case Report
A 9-year-old boy was referred to our pediatric department with symptoms of chronic fatigue, headache, intermittent nausea, and vomiting for 2 months. At admission a weight loss of 2 kg and intermittent subfebril temperature as well as an unspecific tremor of both hands was reported. He had a medical history of erythema migrans 2 years ago treated adequately with amoxicillin for 2 weeks. There was no history of trauma or stay in subtropical countries. Family history revealed a Waldenstrom’s macroglobulinemia of his father and paternal uncle. Clinically, only mild postural tremor of both hands and mild horizontal nystagmus with no other clinical symptoms was noticed.
A cerebral magnetic resonance imaging (MRI) angiography was performed, showing 2 small acute cerebellar infarctions in the posterior inferior cerebellar artery area and occlusion of the basilar artery, highly suspicious of an underlying vasculitis (Figure 1A and B). Conventional cerebral angiography detected a subtotal occlusion of the basilar and bilateral vertebral arteries with retrograde blood flow to the posterior cerebral circulation (Figure 1C).
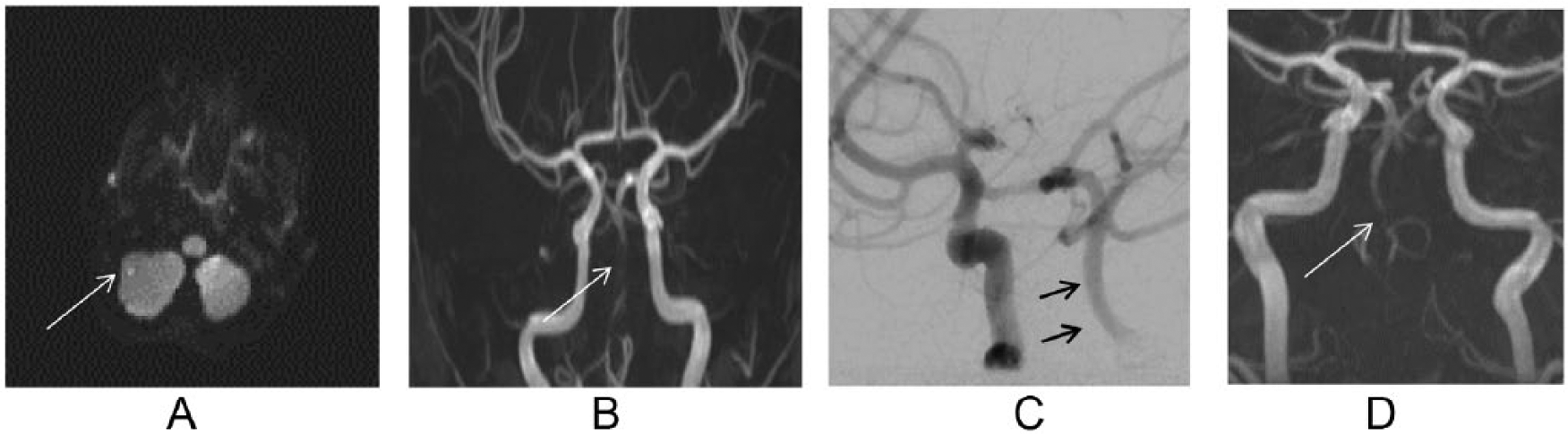
Radiological findings. (A) Acute microinfarction of the right cerebellar hemisphere. (B) MRI angiography with absence of blood flow in the basilar artery. (C) DSA angiography with retrograde filling of the distal basilar artery. (D) MRI angiography 3 months later shows minimal recanalization of the distal basilar artery.
Extended immunological, hematological, and endocrinological laboratory evaluation revealed no abnormalities, among others normal blood count; negative C-reactive protein; normal erythrocyte sedimentation rate; normal renal, thyroid, and liver function; negative thrombophilic parameters; and negative immunological tests with no contribution for systemic lupus erythematosus, antiphospholipid syndrome, or other rheumatologic diseases (Table 1). Instead, Borrelia burgdorferi serology was positive for IgM and IgG, with confirmation of 4 positive bands in Western blot. A lumbar puncture was performed, showing lymphocytosis with increased protein and decreased glucose levels along with an intrathecal production of Borrelia burgdorferi IgM antibodies.
Differential Diagnosis and Laboratory Evaluation in Our Patient.

Abbreviations: CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; CMV, cytomegalovirus; EBV, Epstein–Barr virus; B, Borrelia species; Bb, Borrelia burgdorferi; Ba, B afzelii; Bg, B garinii; SLE, systemic lupus erythematosus; AAS, antiphospholipid antibody syndrome; CNS, central nervous system; cPACNS, childhood primary angiitis of the CNS; IB, immunoblot; MS, multiple sclerosis; cMRI, cerebral magnetic resonance imaging; PFO, persistent foramen ovale.
Positive B. IB: IgG VlsE (Ba + Bb), VIE (Bg), p83 (Ba), p41 (Bg), p39 (Bg), OspC (Bg). IgM OspC (Ba + Bb + Bg).
Therefore, neuroborreliosis was assumed and treatment was started with intravenous ceftriaxone 80 mg/kg/day for 3 weeks in addition to oral acetylsalicylic acid (ASS) 5 mg/kg/day and prednisolone 1 mg/kg/day. Clinical symptoms subsequently improved and neurological examination returned to normal soon after therapy was started.
A follow-up lumbar puncture 3 weeks later showed a reduction of pleocytosis and normalization of liquor glucose and protein. Two months later, MRI angiography showed the absence of cerebellar diffusion restrictions, but an unchanged presentation of the basilar and bilateral vertebral arteries occlusion. The prednisolone therapy was tapered over 3 weeks, whereas ASS therapy was continued. Three months later, a subsequent MRI angiography showed an unvaried occlusion of the basilar and bilateral vertebral arteries with no areas of new infarction (Figure 1D). Clinical and radiological follow-up 6 and 12 months after diagnosis showed a boy without any residual symptoms but an unchanged MRI angiography with ongoing vascular occlusion.
Discussion
Lyme disease is a tick-borne infection that is caused by gram-negative spirochetes, Borrelia species, that induce 3 manifestations: the early and localized presentation as erythema migrans (the most frequent form in children and adults); several early and disseminated forms like neuroborreliosis, lymphozytoma, arthritis, carditis, and myositis, manifesting within weeks; and late disseminated forms like acrodermatitis chronica atrophicans and others, presenting months after infection. 1 Neuroborreliosis is one of the most common infections during childhood and diagnosis can be challenging because of its variety of noncharacteristic symptoms like long-lasting headache, fatigue, and loss of appetite up to presentations with acute hemiparesis.
Lyme disease has been only rarely identified as cause of ischemic or hemorrhagic stroke due to vasculitis in adults2,3 and even more rarely in children.4-6 Lesions due to vascular changes resulting from neuroborreliosis seem to be widely distributed within the brain, showing perfusion deficits due to infarction of the middle cerebral artery, the anterior and posterior artery, or of the central white matter and basal ganglia region.
Differential diagnosis of cerebral vasculitis of childhood is large. Beside systemic lupus erythematosus with central nervous system (CNS) involvement, clinical findings of fatigue, headache, and focal motor deficits are also frequently reported in childhood primary angiitis of the CNS, an entity of vasculitis restricted to the CNS with either anterior and/or posterior cerebral circulation involved. 7 Signs of systemic inflammation such as C-reactive protein, erythrocyte sedimentation rate, white blood cells, or serum IgG elevation may be completely absent. Other differential diagnoses include genetically defined systemic inflammatory diseases with predominant CNS manifestation, 8 antibody-mediated brain inflammation, 9 and metabolic diseases with inflammation of the CNS. 10
Conclusion
Children with chronic neuroborreliosis may have nonspecific and only mild clinical signs but concomitant cerebral vascular involvement may be present, implying a risk for possibly severe secondary complications. Additional neurological symptoms together with a differential diagnosis of neuroborreliosis should prompt supplementary radiological evaluation searching for associated cerebral vasculitis.
Author Contributions
NL and KW contributed equally to this paper. NL, KW, AW and MH contributed in acquisition of data and drafting and reviewing the manuscript and approved the final version of the paper. JS contributed radiological images and interpretation and approved the final version of the paper.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.