
Abstract
The bone is an active tissue subjected to ongoing remodeling process regulated through a fine-tuned equilibrium between formation and resorption and is mainly regulated by osteoblasts, osteoclasts, and osteocytes. Recent developments have identified the essential importance of Osteal Macrophages (OsteoMacs), a unique subset of tissue-resident macrophages, in bone homeostasis. In contrast to osteoclasts, the mononuclear F4/80⁺ OsteoMacs are non-resorbing cells that promote osteoblast function, preserve the structure of the bone remodeling canopy, and regulate local immune responses of the skeletal microenvironment. This review was designed to summarize the uncovering, source, phenotypic characteristic as well as functional role of OsteoMacs in bone remodeling, osseointegration, and response to biomaterials. Knowledge of the cross talk between OsteoMacs and biomaterials provides new opportunities to improve bone regeneration via specific immunomodulation. OsteoMacs therefore, serve as a critical interface between the skeletal and immune systems; and have large relevance in implantology and regenerative medicine.
Keywords
Introduction
In addition to being the structural framework of the body, bone is a dynamic living tissue that continues to experience metabolic activity throughout life. The process of bone remodeling, which is a delicate balance between bone formation and resorption, takes place constantly. The primary cells responsible for this complex process are osteoblasts, osteoclasts, and osteocytes. Originating from mesenchymal progenitor cells, osteoblasts are the bone cells that make and mineralize the bone matrix. Osteoblasts are required for bone development and maintenance. Alternatively, osteoclasts are multinucleated, giant cells originating from hematopoietic precursors that cause bone resorption. 1
For their resorbing activity, the cells are most often located in Howship’s lacunae, which are nothing but minute depressions on bone surfaces caused during bone resorption. 2 Osteocytes are mature osteoblasts that get embedded in the mineralized bone matrix. They act as mechanosensors to help modulate bone remodeling by regulating the functions of osteoblasts and osteoclasts. 1 While traditionally the three cell types have been seen as the major contributors to bone biology, studies in the last several decades have identified OsteoMacs (OMs), a unique subset of macrophages that inhabit bone tissue, as another key player.3–5 The identification of OsteoMacs has revolutionized our knowledge of bone homeostasis and regeneration.
This narrative review was aimed and designed to determine the current evidences on the biology, functions, and clinical significance of osteal macrophages (OsteoMacs/OM’s) in bone remodeling, osseointegration, and biomaterial interactions. The review methodology was developed in accordance with the key principles of the PRISMA 2020 guidelines to maintain transparency and reproducibility, although formal PRISMA flowcharting and quantitative synthesis were not applicable due to the descriptive nature of the study. A comprehensive literature search was performed across PubMed, Scopus, and Web of Science databases, supplemented with relevant textbook references and cross-referenced citations. Publications from the 1980s to 2025 were considered to ensure historical and contemporary perspectives. The search was conducted using combinations of the following keywords and Boolean operators: “osteal macrophages” OR “OsteoMacs” AND “bone remodelling,” “osseointegration,” “macrophage polarization,” “biomaterials,” and “nano-topography.” Articles were screened for relevance based on title and abstract, followed by a full-text evaluation. Both original research and review articles published in English were included.
Studies were selected if they described the identity or biological characteristics of OsteoMacs, discussed their functional roles in bone physiology or regeneration, examined their involvement in implant osseointegration or biomaterial responses, and studied the influence of surface nano-topography or material composition on OM polarization and integration outcomes. Publications that did not specifically refer to OsteoMacs or that focused on macrophage biology unrelated to bone tissue were excluded. Each included study was analyzed and the extracted information was organized under categories addressing:
The cellular identity of OsteoMacs.
Functional roles of OsteoMacs in bone formation and turnover.
Their contribution to implant-related bone healing and osseointegration.
The immunomodulatory influence of biomaterials and nano-topographical modifications on OMs behavior.
This descriptive review aimed to provide an understanding of how OsteoMacs bridge the skeletal and immune systems and to highlight their potential in regenerative and implant dentistry.
The following subheads provide a summary of the main conclusions drawn from the literature.
The discovery of OsteoMacs
OMs are a cell population of macrophage-like cells showing the F4/80 marker and found in proximity to bone surfaces as originally described by Hume and Co-workers in mouse bone model in 1984. 4 OsteoMacs are not the same as osteoclasts. 6 Petit later came up with the nomenclature “OsteoMacs” only later, recognizing their unique occurrence and role as part of the bone microenvironment.5,7
Ontogeny and phenotypic characteristics of OsteoMacs
OsteoMacs (F4/80+ Mac-2−) are macrophages that live in the bones. They develop from embryonic sources which are the yolk sac and fetal liver, then invade into tissues to help regulate homeostasis. Additionally, circulating Ly6C+ monocytes (F4/80+ Mac-2+) can replenish these cells. 5
OMs are also normally found on the surfaces of bones, especially in the periosteal and endosteal areas. They are directly related to mature osteoblasts and are usually found in close proximity to regions of active remodeling. It has been established through research that over 75% of endosteal surface osteoblasts are covered by a cellular lid or a canopy-like structure created by F4/80, CD68 (Cluster of Differentiation 68), and Mac-3 positive OMs5,6 along with Bone marrow envelope cells and bone lining cells which separates the osteoclasts and Osteoblasts from the bone marrow.8,9
Although inflammatory macrophages and OMs have a number of markers in common (CD45, CD115, CD68, CD11b, CD107b, and Gr-1) making it difficult to differentiate between them,
10
even so OsteoMacs and osteoclasts differ from each other in three important ways: 2. Marker Profile: They lack characteristic osteoclast markers like TRAP (Tartrate-Resistant Acid Phosphatase), cathepsin K, and RANK (Receptor Activator of Nuclear Factor Kappa-Β), though they are positive for F4/80+.
7
3. Function: Rather than promoting resorption, OMs promote bone growth and homeostasis.
6
Regulatory mechanisms in bone remodeling
OMs are highly adaptable cells. They can either support anabolic (bone-building) activities or play a role in inflammatory processes, depending on the environment in which they exist. 11
OMs play a key role in osteoblast function; it has been found in vitro that their absence from primary bone cell cultures results in a 23-fold decrease in bone mineralization. 5
Their functional importance was also confirmed in transgenic mouse Macrophage Fas-Induced Apoptosis (MaFIA) system, wherein selective macrophage removal interrupted this canopy formation reducing mineralization. This directly demonstrates the essential function of OMs in the upkeep of the bone remodeling process, as it led to a depletion of mature osteoblasts and an abrupt halt in bone growth. 12
Advances in single-cell RNA sequencing have identified multiple macrophage subpopulations, each with distinct transcriptional profiles and regulatory pathways involved in bone remodeling.13,14 Single cell level transcriptomic analysis reveals that signals from macrophages, such as Oncostatin M, influence mesenchymal progenitor differentiation and osteogenesis. 13 Whereas other macrophage subsets activate cytokine and osteoclast related pathways that are essential for bone homeostasis. 14 These findings highlights the functional diversity of OMs within the bone microenvironment, corresponding with evidence of macrophage polarization and specialized bone-associated macrophage populations that regulate osteoblast activity and bone formation. 5 Together, these findings increase our understanding of osteo-immunological interactions in bone remodeling and emphasize the heterogeneous nature of OMs.
The incorporation of interactions between osteoclasts, osteoblast lineage cells, osteocytes, and immune-associated cells, mathematical modeling has improved our understanding of regulatory networks in bone remodeling. Hwang (2018) 15 used a modified computational model based on Graham (2013) that included pre-osteoblasts, osteoclasts, osteocytes, and osteal macrophages (OM), focusing on their signaling impact on osteoblast differentiation. The results showed that instability and a steady decrease in bone volume were caused by decreased signaling from osteocytes and OM. Notably, while osteocyte signaling enhancement alone was insufficient and linked to ongoing bone loss, increased OM signaling enhanced bone mass even in the presence of low osteocyte activity. These findings, which are in line with more extensive modeling data, emphasize the significance of threshold-dependent regulatory mechanisms and imply that OM might be important stabilizing components of the network of bone remodeling. These findings support the importance of immune-skeletal interactions and could guide future treatment approaches for bone disorders. 15
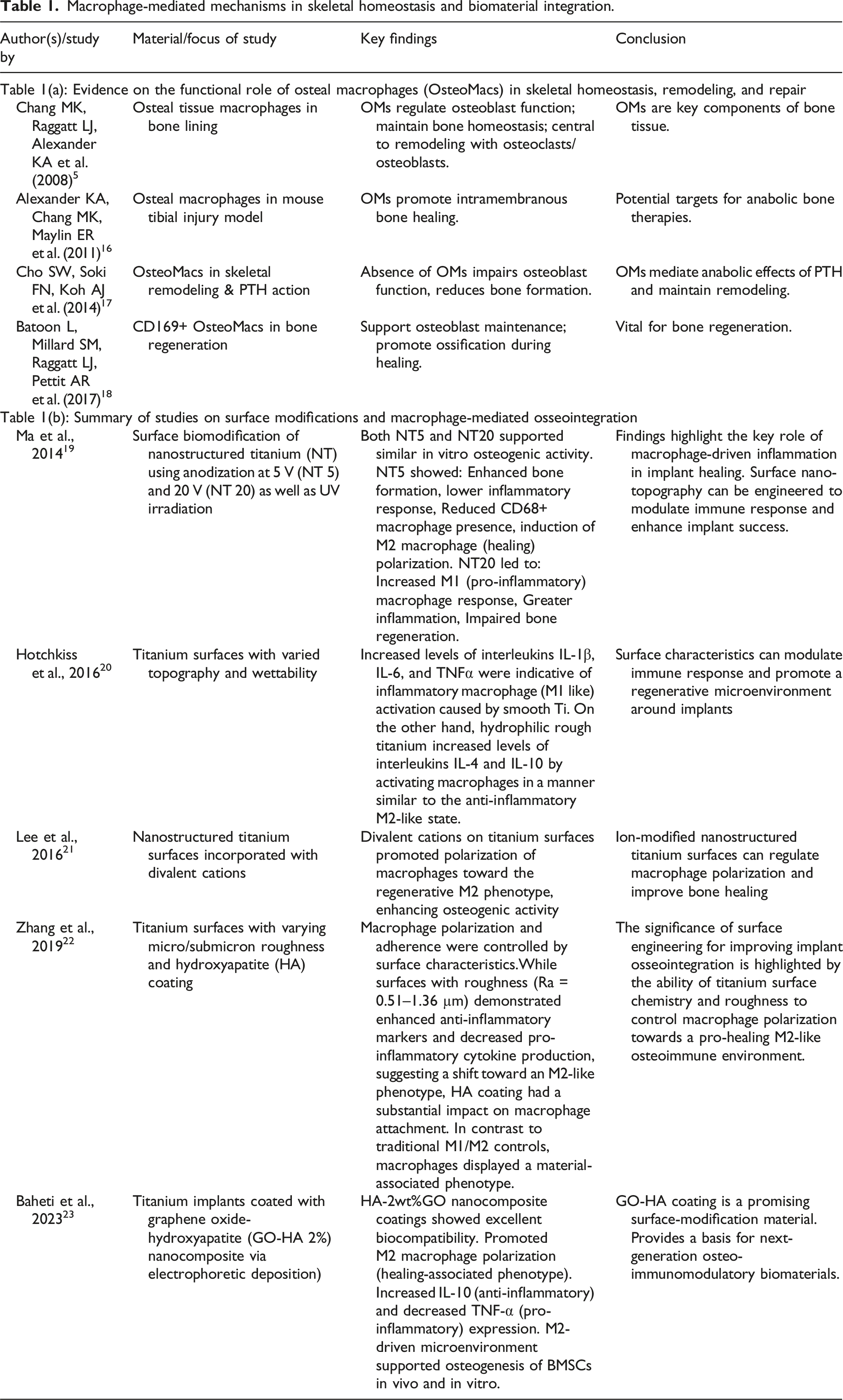
Macrophage-mediated mechanisms in skeletal homeostasis and biomaterial integration.
OsteoMacs in implants and bone healing
It is interesting that OMs are amongst the first immune cells to reach locations of new bone formation, including the areas around implants. Their capacity to impact the bone environment seems to come from their ability to switch between two functional phenotypes: 24 M1 (pro-inflammatory) and M2 (anti-inflammatory/healing).
When responding to stress or infection, M1 OMs commonly secrete inflammatory mediators including IL-1 (Interleukin-1), IL-12, TNF-α (Tumor Necrosis Factor Alpha), and MMPs (Matrix Metalloproteinases) Figure 1(a). The influence of biomaterial properties on OsteoMac (OMs) polarization.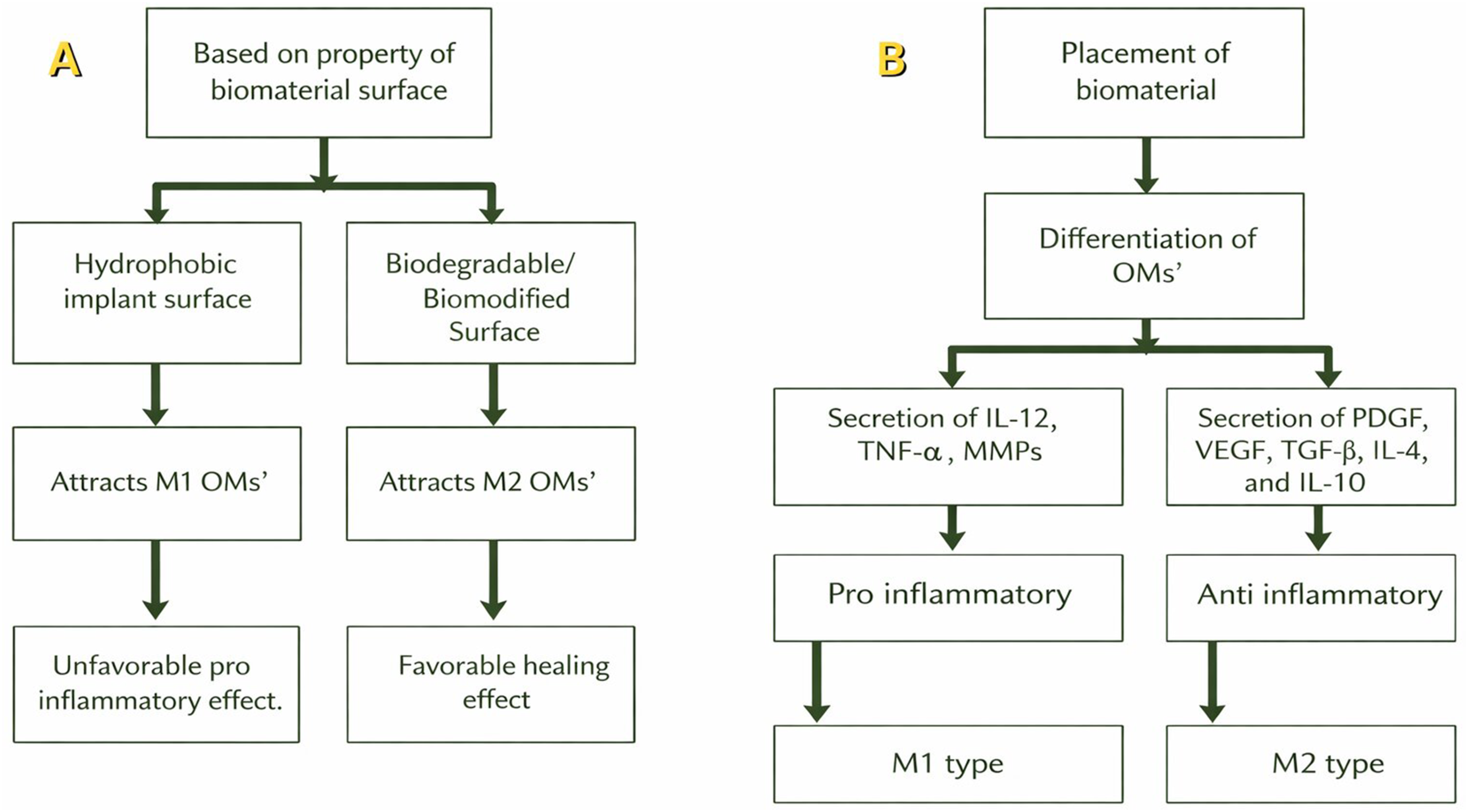
On the other hand, M2 OMs induce tissue regeneration via the release of growth and healing factors such as PDGF (Platelet-Derived Growth Factor), VEGF (Vascular Endothelial Growth Factor), TGF-β (Transforming Growth Factor Beta), IL-4, and IL-10. 24
The M2 macrophage phenotype can be further divided in several other phenotypes as M2a which Increase endocytic activity, tissue repair and cell growth, M2b which helps in balancing inflammatory response, M2c which is involved in phagocytosis of apoptotic cells and M2d which promotes angiogenesis.25,26
Influence of biomaterials on OsteoMacs
In addition, the materials that OMs are exposed to influence their behavior. For example, M1 OMs are drawn to hydrophobic implant surfaces because of the unfavorable perception of these surfaces by tissues.27,28 Biodegradable or biomodified surfaces, on the other hand, would tend to promote M2 polarization promoting healing (Figure 1(b)). 29
These findings emphasize the dynamic interaction between the immune-bone interface and implant materials. Biomaterials are highly important in establishing a healing environment that is supportive of osteogenesis, promoting osseointegration, and facilitating bone repair through promotion of an anti-inflammatory, healing-inducing phenotype. It showcases the highly versatile nature of OMs and their promising role as a therapeutic agent in implant dentistry and regenerative medicine.
Nano-topography-driven OsteoMac polarization and implant integration
After implantation, plasma proteins rapidly adsorb onto biomaterial surfaces, forming a conditioning layer through the Vroman effect, in which proteins with higher surface affinity gradually replace initially adsorbed proteins. 30 This adsorbed protein layer presents adhesion ligands that interact with integrin receptors on macrophages, activating signaling pathways that regulate macrophage behavior. 31 Changes in integrin signaling have been shown to influence macrophage phenotype, and alterations such as β3 integrin depletion can promote polarization toward an M2 (pro-healing) phenotype. 32 Thus, in this way the protein adsorption and subsequent integrin receptor interactions on implant surfaces can contribute to M2 macrophage polarization and a pro-regenerative immune response.
He et al. (2022)
33
reviewed how microscopic surface features called nano-topographical cues on dental and orthopedic implants forms a protein adsorption pattern immediately on their surface with which the immune cells of our body interact, this influences the way in which our body reacts to the implant (Figure 2). Rather than just focusing on bone-forming cells like osteoblasts, the important role of immune cells, especially the macrophages and osteoclasts, in the healing process was highlighted. It is found that certain nanoscale patterns, such as nanotubes and grooves, can help guide macrophages toward a more anti-inflammatory (M2) state and reduce the bone-resorbing activity of osteoclasts. These effects are achieved by how the cells sense and respond to the surface structure through their receptors and internal signaling. Therefore, by carefully designing implant surfaces at the nanoscale, we can encourage better healing, reduce inflammation, and improve how well implants osseointegrate. Schematic representation of how nano-topographical cues on the implant surface influence protein adsorption, which in turn guides immune cell interactions. This microenvironment modulates the polarization of osteal macrophages (OsteoMacs) into either the pro-inflammatory M1 phenotype or the anti-inflammatory, pro-healing M2 phenotype, thereby affecting the inflammatory response and osseointegration.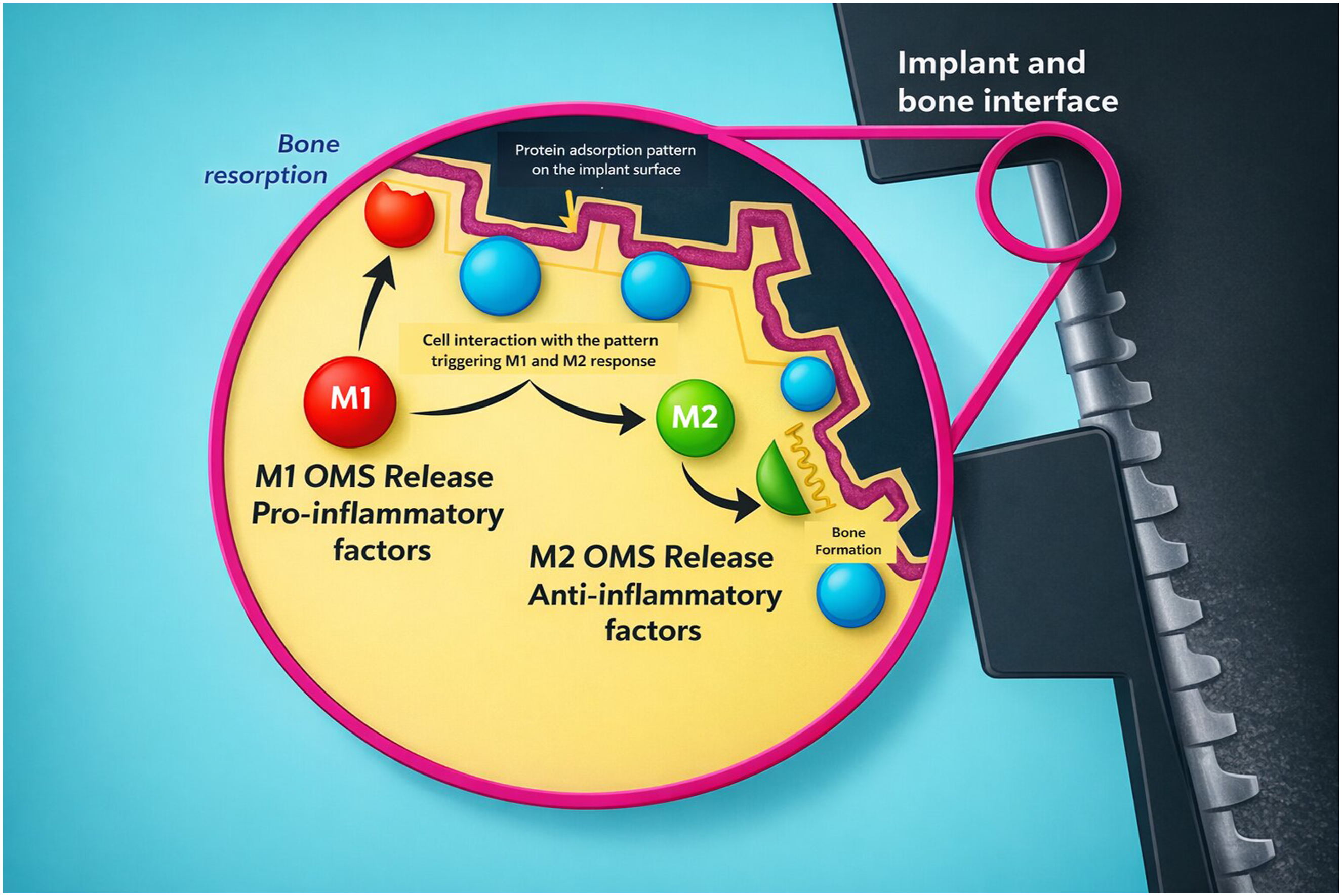
The effect of nano-topography of implant surface on macrophage polarization into M2 phenotype and its effect on osseointegration of implant is summarized in Table 1(b).
Both studies highlight how changing the surface of implants can play a key role in guiding immune cells, specifically macrophages, to adopt the M2 type, which helps reduce inflammation and supports bone healing. This shift is important for making implants work better in the body. Ma et al. 19 studied how physically altering the tiny surface features of titanium implants can influence healing. These studies provide ways to steer the immune response in a way that improves implant success. Hotchkiss et al. 20 showed that the characteristics of titanium surfaces affect macrophage polarization, with smooth surfaces encouraging pro-inflammatory M1-like responses, whereas rough hydrophilic surfaces increased anti-inflammatory M2-like cytokine production. In a similar way, Lee et al. 21 demonstrated that nanostructured titanium altered with divalent cations encourages macrophage polarization towards a regenerative M2 phenotype, boosting osteogenic activity. Zhang et al.22also indicated that micro/submicron surface roughness and hydroxyapatite coating influence macrophage adhesion and polarization, fostering a pro-healing osteoimmune setting that enhances osseointegration. Baheti et al. 23 focused on using a special biochemical coating combining hydroxyapatite and graphene oxide.
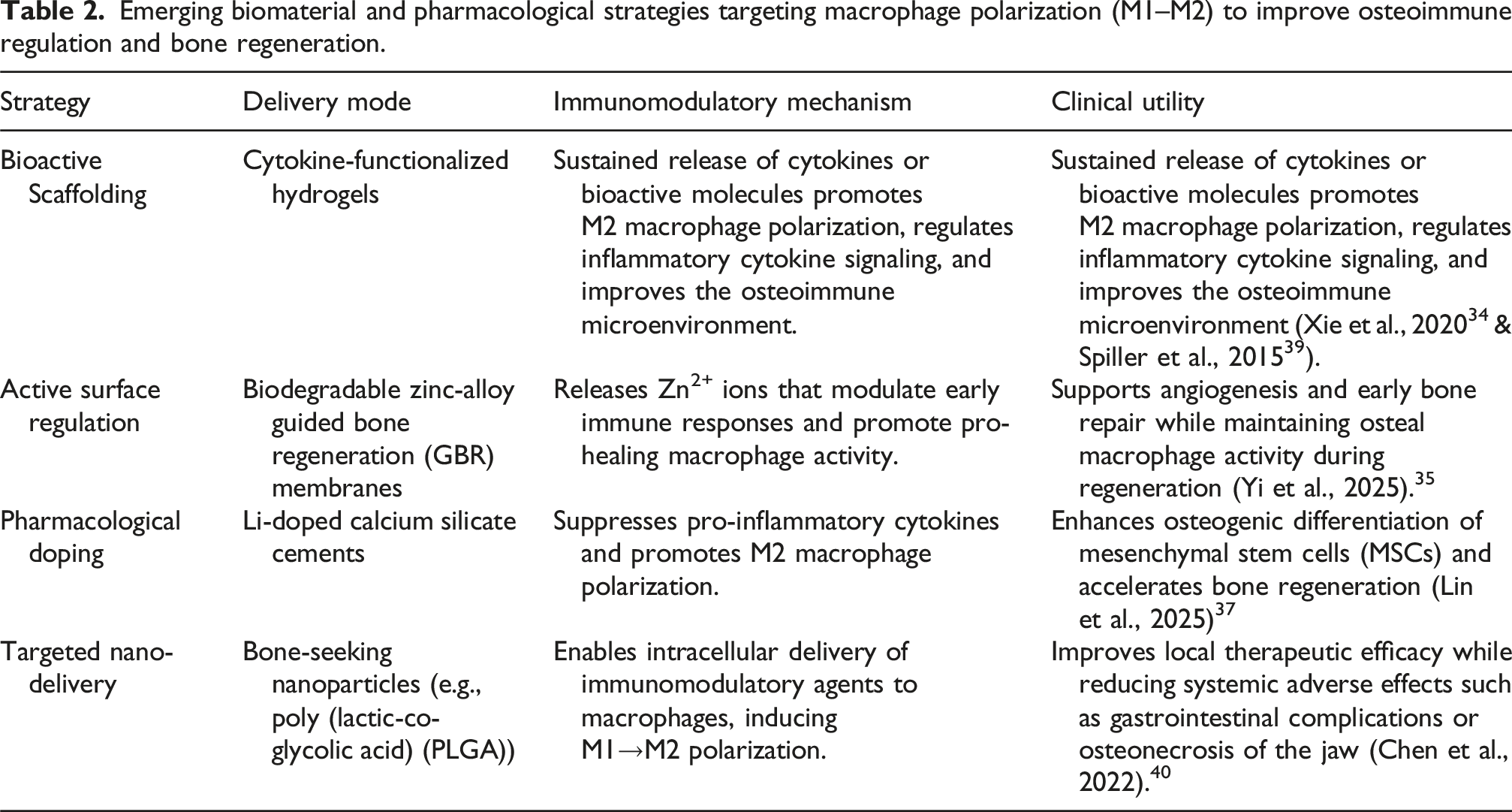
Therapeutic perspective of OsteoMacs
Emerging biomaterial and pharmacological strategies targeting macrophage polarization (M1–M2) to improve osteoimmune regulation and bone regeneration.
Discussion
This narrative review highlights the pivotal role of OMs as specialized bone-resident macrophages bridging the skeletal and immune systems. Since their initial description by Hume and co-workers in 1984, understanding of their biology has advanced significantly. Unlike osteoclasts, which mediate bone resorption, OMs are primarily anabolic, supporting osteoblast differentiation, mineralization, and maintenance of bone homeostasis. Their close association with osteoblasts highlights their role as regulators of the bone remodeling canopy.
The dual polarization potential of OMs into M1 (pro-inflammatory) and M2 (anti-inflammatory or reparative) phenotypes reflects their adaptability within the bone microenvironment. This plasticity is crucial in determining the balance between inflammation-driven bone loss and regeneration. Studies have shown that an initial M1 response is essential for immune activation, and the M2 phenotype promotes tissue repair, angiogenesis, and osteogenesis. Disruption in this transition, or prolonged M1 activation, may contribute to delayed healing or implant failure.
The interaction of OMs with biomaterials and implant surfaces represents an emerging topic in dental and orthopedic research. Surface chemistry, topography, and hydrophilicity can directly influence macrophage polarization and subsequent tissue response. Hydrophilic and bioactive surfaces tend to promote M2-type responses, whereas hydrophobic or unmodified titanium surfaces often sustain M1-dominant inflammation. Such evidence supports the concept of immunomodulatory biomaterials materials engineered to actively direct favorable immune responses rather than being inert substrates.
Nano-topographical engineering of implant surfaces provides additional control over cellular responses at the immune-bone interface. Nanoscale features can modulate protein adsorption and receptor-mediated signaling, thereby influencing macrophage behavior and osteogenic integration. This cross-disciplinary understanding of immune modulation through surface design provides a biological rationale for next-generation implant technologies.
Clinically, OMs represent a key therapeutic target in regenerative and implant dentistry. By modulating their activity or designing biomaterials that favor M2 polarization, it may be possible to accelerate osseointegration, improve bone healing, and enhance implant longevity. However, despite promising in vitro and preclinical data, translation to clinical application remains limited due to incomplete understanding of OMs signaling pathways and the heterogeneity of patient immune responses.
Conclusion
OM represent the concept of osteoimmunology in action linking immune regulation with skeletal repair. Future research should integrate molecular, materials, and clinical approaches to harness OMs biology for therapeutic benefit in bone regeneration and implant integration. With advancing research, the modulation or targeting of OMs activity can reveal new possibilities in periodontal therapy, bone regeneration, and implantology. Once unknown, OMs are now central to bone-immune interactions with great prospects for the future of regenerative and restorative medicine.
Further research is needed to clarify the molecular pathways governing OMs differentiation and polarization, as well as their precise role in osseointegration. Standardized markers and clinical validation studies are essential to translate experimental findings into therapeutic strategies. Future biomaterial designs should focus on modulating OMs responses to enhance bone regeneration and implant success.
Clinical significance
A deeper understanding of OM biology provides valuable clinical insights for improving outcomes in implant and regenerative dentistry. By influencing the early immune response at implant sites, OM play a decisive role in determining the quality of osseointegration and long-term implant stability. Designing biomaterials and implant surfaces that promote M2 type OM polarization can enhance bone healing, reduce peri-implant inflammation, and shorten recovery time. Furthermore, therapeutic modulation of OM activity may open new pathways for managing bone-related pathologies and improving success rates of bone grafts and implants in compromised patients.
Footnotes
Author note
The work belongs to Department of Periodontology, Rural Dental College, Loni.
Acknowledgments
I thank Mr Ankush Khotpal for proof reading the article.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The author declares that Artificial Intelligence (AI) tools were used solely to improve the readability and language of the manuscript and to enhance the schematic diagram, which was originally conceptualized and created by the author herself. No AI tool was used for generating scientific content, analysis, or references.