
Abstract

Introduction:
Epigastric hernias, located superior to the umbilicus in the linea alba, are found in the pediatric population. 1 –3 Surgical repair is typically performed open with a periumbilical incision; however, if the hernia is located greater than 3–4 cm above the umbilicus, open repair may be technically challenging. 1 Technical challenges of open surgery, such as small or multiple defects that are difficult to palpate, invite surgeons to perform laparoscopic repair. Suture passing devices may create fascial holes as large as the defect itself. We describe a technique for repairing epigastric hernias, employing a lasso technique and a small-gauge needle.
Materials and Methods:
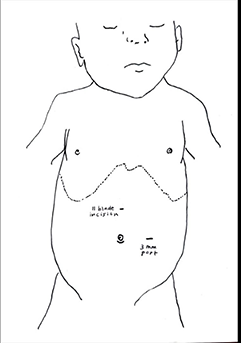
A small curvilinear infraumbilical incision is made, and a 3 mm port is placed upon entering the abdomen. Pressure of 10 mm Hg is adequate. A 3 mm port is placed on the patient’s left, lateral to the umbilicus (Fig. 1). Once the defect is identified. A small incision is made with a #11 blade in the skin over the hernia site.
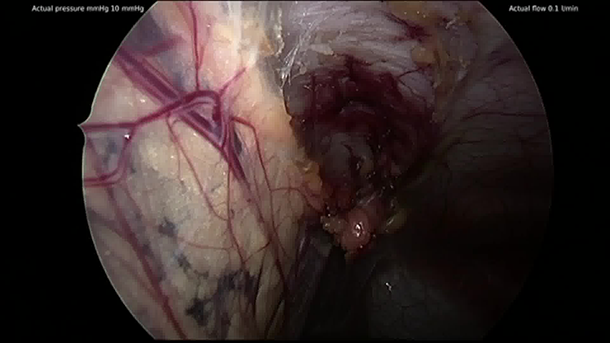
Figure-of-eight technique steps
(Fig. 2):
An 18-gauge spinal needle loaded with a 3-0 Prolene suture loop is introduced in the superior right part of the defect. The suture is passed into the abdominal cavity, and the spinal needle is removed, leaving the suture loop. The spinal needle is then introduced into the inferior right part of the defect, and a 3-0 Vicryl suture is passed into the spinal needle and through the Prolene lasso. The Prolene lasso is then pulled out of the abdomen to take out the distal end of the Vicryl suture such that the first throw is placed. This behaves as the “needle” end. The spinal needle is then removed and reintroduced into the superior left part of the defect, and a Prolene lasso is again passed into the abdomen. The spinal needle is removed and reintroduced into the inferior left part of the defect, and another Prolene lasso is passed into the abdomen and through the previous Prolene lasso (lasso in the lasso). The first left-sided lasso is pulled outside of the abdomen such that the second lasso is also above the skin. The inferior right Vicryl (“needle” end) that is outside the skin is passed into the lasso. The lasso is then pulled back into the abdomen and out of the skin in the inferior left part of the defect. The figure-of-eight stitch is finally tied in the subcutaneous space. For larger defects, the technique can be repeated along the defect to create a running stitch before tying. Larger suture materials may be used.
Summary:
Laparoscopic repair of epigastric hernias using the figure-of-eight technique described is a technically feasible and durable option. The use of this technique works well with epigastric hernias that are 3–4 cm or more superior to the umbilicus. Laparoscopy can help ameliorate the technical challenges of open surgery by avoiding a large incision in the epigastric area, offering better cosmesis, better visualization of the defect, and comparable outcomes.
Patient consent statement:
The authors have received and archived patient consent for video recording/publication in advance of video recording of procedure.
Authors’ Contributions:
C.N.: Conceptualization, methodology, validation, investigation, writing—original draft, and visualization. C.C.-T.: Conceptualization, methodology, validation, investigation, writing—original draft, and visualization. T.K.: Conceptualization, methodology, investigation, and writing—review and editing. A.V.C.: Conceptualization, methodology, validation, investigation, writing—review and editing, and visualization. J.Z.: Conceptualization, methodology, validation, investigation, writing—original draft, visualization, and supervision.
Author Disclosure Statement:
Authors have received and archived patient consent for video recording/publication in advance of video recording of procedure. The authors have no disclosures to report.
Funding Information:
The authors have no funding to disclose.
Runtime of video:
2 mins 25 secs.