
Abstract
Experiential learning links knowledge to real practice through seasoned mentor support, professional reflection, and hands-on experience in authentic work environments. While academic public health programs seek to train the future workforce, the current workforce has a critical need for training as well. The Region IV Public Health Training Center’s Pathways to Practice Scholar program gives public health students the opportunity to apply knowledge to competency-based experiences while fulfilling the current workforce’s short- and long-term human resource needs. Placements are offered in all eight states of the region to broaden opportunities for both agencies and student scholars. On completion of the program, scholars are required to submit an executive summary, reflection statement, photos of the experience, and a draft abstract suitable for submission to a professional conference. Since 2015, 36 scholars have been placed in positions across Region IV, 11 in states other than those of their home universities. Students were placed at state, local, and tribal health departments; area health education centers (AHECs); and other agencies (e.g., primary care settings), and the most common work plan domains selected by scholars were analytic/assessment, policy development/program planning, and leadership/systems thinking skills. Scholars’ perceived confidence increased across all domains with the highest increases in financial planning/management and cultural competency. Program implementation and evaluation findings are described, including types of projects, differences in confidence in performing competency domains, and confidence and interest in working with underserved populations. Evaluation findings indicate that the Region IV Public Health Training Center scholars increased their confidence in performing practice competencies while providing support for public health agencies serving underserved populations.
Introduction and Background
Experiential learning is critical for equipping students for real-world community practice. This type of training involves practice-based learning through seasoned mentor support, professional reflection, and direct hands-on experience in authentic work environments. While constructing knowledge requires practice, practice also requires knowledge; experiential learning links the two (Higgins, 2009; Klein-Collins, 2013; Yardley, Teunissen, & Dornan, 2012). Universities are increasingly incorporating experiential learning into their curricula via techniques such as field experiences, discipline-specific applied learning, cooperative education, and service learning (Austin & Rust, 2015; Ryan, Toohey, & Hughes, 1996). In addition to general college programs, experiential learning is widely applied across health-related professional programs, including public health (Cox, Clutter, Sergakis, & Harris, 2013; de Oliveira et al., 2015; Hernandez, Bejarano, Reyes, Chavez, & Mata, 2014; Koponen, Pyörälä, & Isotalus, 2012; Warkentin, 2016). Best practices to maximize levels of active learning include providing student access to a wide range of practice opportunities with broad learning outcomes tailored to a student population’s needs (Coker & Porter, 2015; Gilbert, Banks, Houser, Rhodes, & Lees, 2014).
These skill-centered experiences align to meet the requirements of competency-based academic programs by applying specific knowledge to action (Klein-Collins, 2013). For example, accredited programs and schools of public health use competencies, including the Council on Linkages (COL) Between Academia and Public Health Practice (2014), to link curricula and experiential learning initiatives (Anderson, Royster, Bailey, & Reed, 2011; Hernandez et al., 2014; Oglesby et al., 2013). These core competencies are also used as a guide for public health workforce development in health departments (Stewart, Halverson, Rose, & Walker, 2010). Students benefit by achieving academic practicum requirements and applying knowledge and skills to real practice settings (McCormick, Reel, Alperin, Lloyd, & Miner, 2017; Steigerwald, Nolan, Loux, Baskin, & Scharff, 2016). Students can also enrich their experiences by problem solving, collaborating, and learning directly from disparate communities (Anderson et al., 2011; Villanueva, Hovinga, & Cass, 2011). Partner agencies gain supplemental support from students with formal academic training who complete projects that contribute to the organizational mission. With more substantive professional contact with students, agencies can also make more informed personnel decisions in hiring students post graduation. (Divine, Linrud, Miller, & Wilson, 2007; Frazee, 1997; McCormick et al., 2017).
While academic public health programs seek to train the emerging workforce, the current workforce also has a critical need to train new professionals. In 2014, the Association of State and Territorial Health Officials (2016) conducted the Public Health Workforce Interests and Needs Survey, a national survey of public health professionals. According to Sellers et al. (2015), survey results demonstrated a dramatic need for succession planning and retention of the future public health workforce. Over 42% reported that they were considering leaving their organization in the next year or retiring before 2020. This projected turnover creates an urgent need to continually recruit and train incoming professionals (Sellers et al., 2015). Experiential learning opportunities help public health students build essential professional competencies in preparation for joining this workforce.
Overview of Pathways to Practice Scholars Program
The Region IV Public Health Training Center (R-IV PHTC) is one of the 10 regional PHTC sites in the Public Health Learning Network funded by the Health Resources and Services Administration (HRSA, 2014; Public Health Learning Network, 2016). The R-IV PHTC Central Office at Emory University partners with six Local Performance Sites (LPSs) to train the current and future public health workforce in eight southeastern states (Alabama, Florida, Georgia, Kentucky, Mississippi, North Carolina, Tennessee, and South Carolina). LPS partners include East Tennessee State University, Florida A&M University, Medical University of South Carolina, University of Alabama at Birmingham, University of Louisville, and the University of North Carolina Wilmington.
Part of R-IV PHTC’s mission is to foster a learning community to build competence in the current and future public health workforce and expose public health students to the value of working in underserved areas. The R-IV PHTC nurtures future leaders and mentors through the Pathways to Practice Scholars program, placing students from accredited schools and programs of public health to work on practical field placement projects alongside seasoned public health practitioners. By design, the program includes elements—such as a competency-based work plan, agency deliverables, reflective writings and evaluation to build leadership, and real-world experience in the future public health workforce—while serving the immediate needs of public health agencies and building a mentorship infrastructure. The program creates and enhances linkages to benefit agencies and students throughout the region. Placements are offered in all eight states to broaden opportunities for both agencies and students. Students from across the region’s universities, with many different skill sets, apply for positions at a broad array of agencies addressing a variety of content areas. A smaller subset of the field placement positions, called Faculty–Student Collaborative Projects, also involve a faculty advisor from a university to contribute subject matter or methodology expertise. This examination of the program focuses on all field placements and does not distinguish between field placement types.
HRSA limits the number of field placement positions that can be posted by each of the Regional PHTC, regardless of the number of states in the region, to no more than 20 total positions per year. Each trainee is eligible to receive a stipend of up to $1,500 and must be a citizen of the United States, a noncitizen U.S. national, or a foreign national having in his or her possession a visa permitting permanent residence in the United States (HRSA, 2014).
Processes and Procedures
Host Agency Proposal Selection
The Central Office and LPSs solicit field placement positions from potential host agencies serving or working on behalf of medically underserved communities and populations (MUC/Ps) across the eight southeastern states. Positions must take place in governmental, nonprofit, or community-based agencies providing public health services and working on or behalf of MUC/Ps. Agencies complete a field placement proposal form to describe the agency, the populations it serves, and the proposed competency-based student projects. To be chosen, the proposed project must provide a meaningful (competency and skills-based) public health experience for students. The agency must identify a mentor who will serve as the primary point of contact, guide the student, oversee day-to-day tasks, and evaluate the student’s progress.
The Central Office and LPSs identify and select two to three agency proposals per state to post on the R-IV PHTC website, advertising the positions to the accredited schools and programs of public health within R-IV. Students apply for positions by sending their application materials (i.e., resume, cover letter with citizenship status, transcript, and writing sample) to the field placement coordinator at the R-IV PHTC Central Office. The Central Office holds orientation webinars for mentors and LPS partners on the Pathways to Practice program, timeline, student deliverables, and expectations for mentor involvement. Mentors are expected to educate the student on agency policies and procedures, supervise and mentor the student to ensure that they accomplish deliverables, and participate in final placement evaluation.
Student Recruitment and Selection
Each LPS or Central Office promotes the positions at their universities and/or partner universities. Promotional methods include posts on the R-IV PHTC Website, online student job portals, and e-mail listservs, and through faculty/staff recommendations. Students can apply to multiple positions, including positions outside the state of their home institution. The Central Office reviews student applications for completeness and to ensure eligible citizenship status. Application materials for all eligible candidates are sent to the host agencies and, when requested, affiliated LPS for review. Agencies review applications, contact candidates for telephone interviews, and select the top candidate. The agencies then notify the Central Office, which sends the official offer by e-mail to students along with information on deliverables and stipends. If the agency requires a memorandum of understanding, the Central Office works with the student’s home university to put that into place before the student begins work.
Implementation of Pathways to Practice Scholars Program
The selected students (scholars) participate in an orientation webinar with an overview of the program, including program timeline, mentorship, scholar responsibilities and deliverables, work plan, field placement evaluation, and agency policies and procedures. The Central Office provides each agency with a work plan template to document placement-specific tasks and deliverables, and the scholars and mentors collaborate to create the final work plan. This process involves the mentor selecting up to 10 COL Tier 1 (entry-level) competencies that could be covered within the scope of the project(s). The scholar then selects 5 of those 10 competencies to strengthen during the field placement. The work plan also clarifies expectations for the scholar, agency mentor, and R-IV PHTC, and is signed prior to the start of the placement.
The R-IV PHTC scholars program requires scholars to submit an executive summary, reflection statement, photos of the experience, and a draft abstract suitable for submission to a professional public health conference. The program’s deliverables do not supersede those of the scholar’s home institution’s degree requirements; instead, the Central Office helps scholars determine the potential overlap in the deliverables to streamline the process.
Program Evaluation
The R-IV PHTC implemented evidence-based strategies to evaluate its performance and progress toward outcomes aligned with its Scholar program. These strategies monitor the operational aspects of the program and assess the effectiveness of the program in meeting its overall goals (to build student competencies and confidence in working with or on behalf of MUC/Ps). Evaluation instruments include a presurvey, midpoint survey, final evaluation, and 1-year follow-up survey for students, as well as a final evaluation survey for mentors.
Scholars complete a presurvey at the beginning of their placement to report their level of confidence in performing each of the five COL competencies indicated in their work plan. Scholars also rate their confidence and current interest in working with MUC/Ps. Halfway through the experience, scholars complete a midpoint evaluation that serves as a progress report. At the end of the placement, a final evaluation is completed, assessing their perceived confidence in performing each of their selected five COL competencies, their confidence and interest in working with MUC/Ps, and their overall ratings of the agency and mentor. One year after the placements, scholars complete a follow-up survey to report current employment, particularly work in MUC/Ps and rural communities. Scholars also indicate how the program affected their current career focus or aspirations.
On their final evaluation survey, mentors rate the scholar’s personal attributes, professional skills, and strengths as an entry-level public health professional. In addition, mentors are asked if they would recommend hiring this individual if given the opportunity. The 16 scholars that completed their field experience in 2015 were sent a 1-year follow-up survey in July 2016. This survey was programmed into Qualtrics© and distributed via e-mail with an invitation to participate in the survey.
Evaluation Findings and Program Outcomes
Since 2015, 36 scholars have been placed in positions across Region IV, 11 in states other than those of their home universities. The average age of the 36 scholars was 25 years (range: 22-37 years). Twenty-seven (75%) of the scholars identified themselves as female; 9 (25%) as male. Racial distribution was 22 (61%) White, 11 (31%) Black or African American, 2 (6%) Asian, and 1 (3%) native Hawaiian or Pacific Islander. Eleven scholars (31%) indicated that they were raised primarily in a rural area and 6 (17%) indicated they were from disadvantaged backgrounds, defined as having limited access to educational opportunities due to environment or severely limited finances.
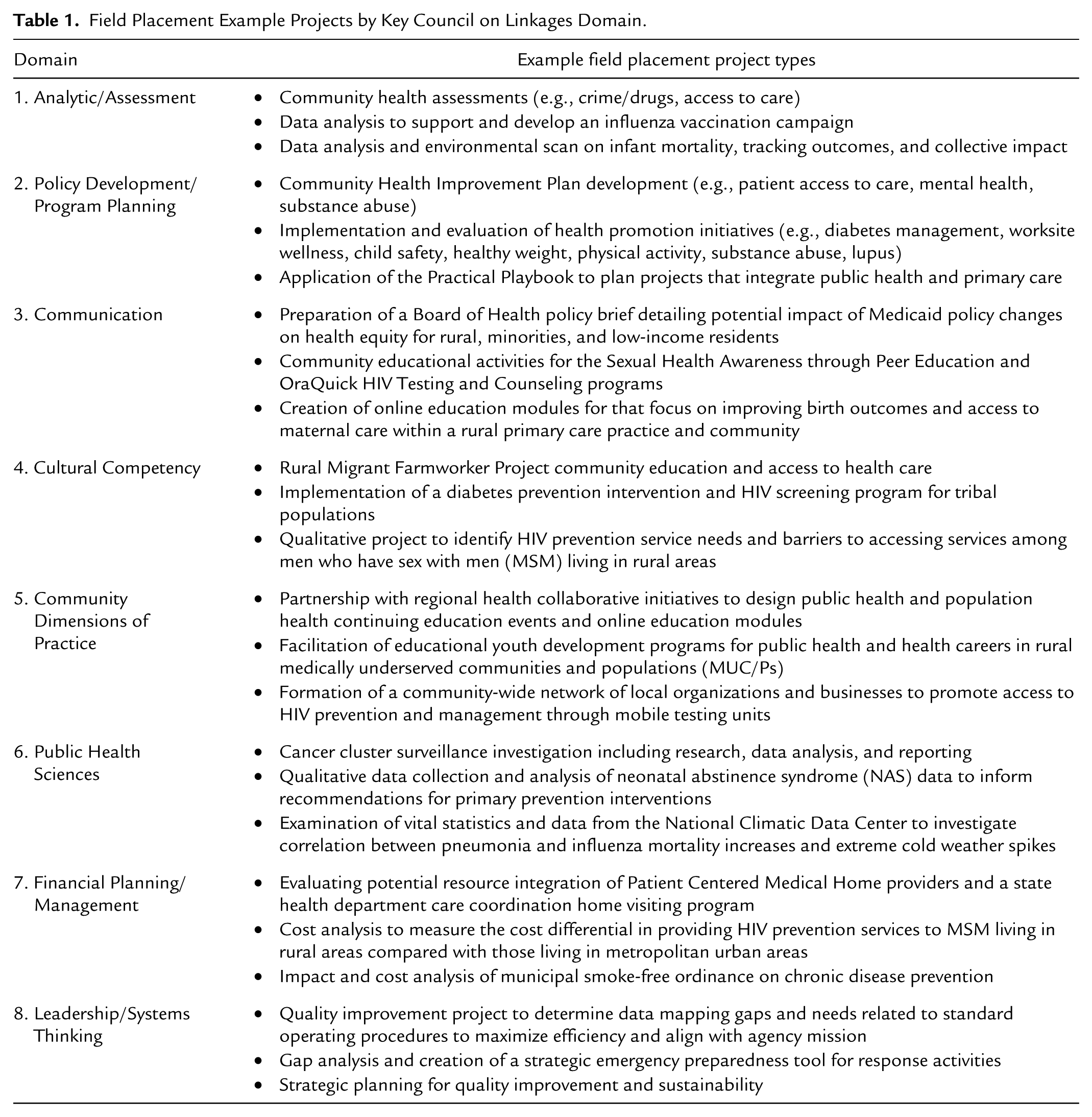
Ten (28%) of the placements were at state health departments, 11 (30%) at local health departments, 9 (25%) at AHECs, 5 (14%) at other agencies (e.g., primary care settings, academic centers), and 1 (3%) at a tribal health department. Most projects were multidimensional and often fulfilled requirements of multiple competency domains. Table 1 provides select examples of the types of field placement projects and a key competency domain addressed.
Field Placement Example Projects by Key Council on Linkages Domain.
In the work plans, the top COL competency domains selected by scholars were analytic/assessment (selected by 81% of the scholars), policy development/program planning (67%), community dimensions of practice (61%), leadership/systems thinking (58%), and communication (50%). In both the presurvey and final evaluation, scholars were asked to assess their confidence in performing each selected competency using a scale of 1 (not at all confident) to 5 (extremely confident). For scholars with matching pre- and postdata, Table 2 illustrates the students’ perceived change in confidence pre- and postplacement by the competency domains they selected to address. The highest confidence scores prior to the field placement were in the analytic/assessment, communication, and leadership/system thinking domains, each of which had an average score of 3.1. After the field placements, the highest confidence scores were in communication and leadership/systems thinking domains, each of which had an average score of 4.8. According to an examination of the differences between pre- and postscores, scholars gained the most confidence in financial planning/management domain (difference: 2.0), followed by the cultural competency domain (difference: 1.9).
Average Pre- and Postconfidence Scores a by Competency Domain.
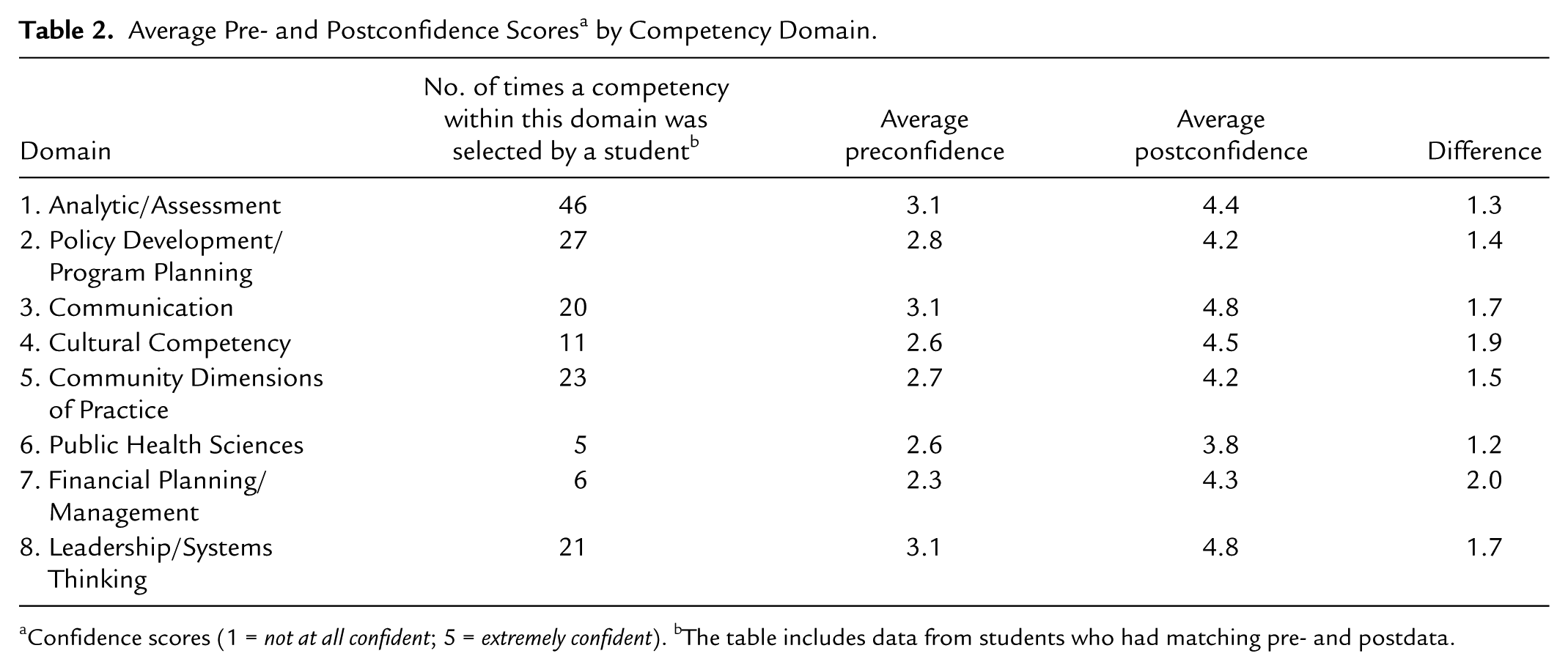
Confidence scores (1 = not at all confident; 5 = extremely confident). bThe table includes data from students who had matching pre- and postdata.
Prior to their field placement and again at the conclusion of their placement, scholars were asked about their confidence working with or on behalf of underserved populations (1 = not at all confident, 5 = extremely confident) and their interest in working with vulnerable or underserved populations (1 = not interested, 5 = very interested). While Table 3 shows a positive difference—indicating that as a whole, scholars had higher confidence and higher interest in working with underserved populations at the end of their placements than they did at the beginning—the differences are small. This small difference may reflect the fact that those who are drawn to public health and these types of field placement experiences already have confidence and interest in working with vulnerable populations.
Confidence and Interest in Working with Underserved Populations.
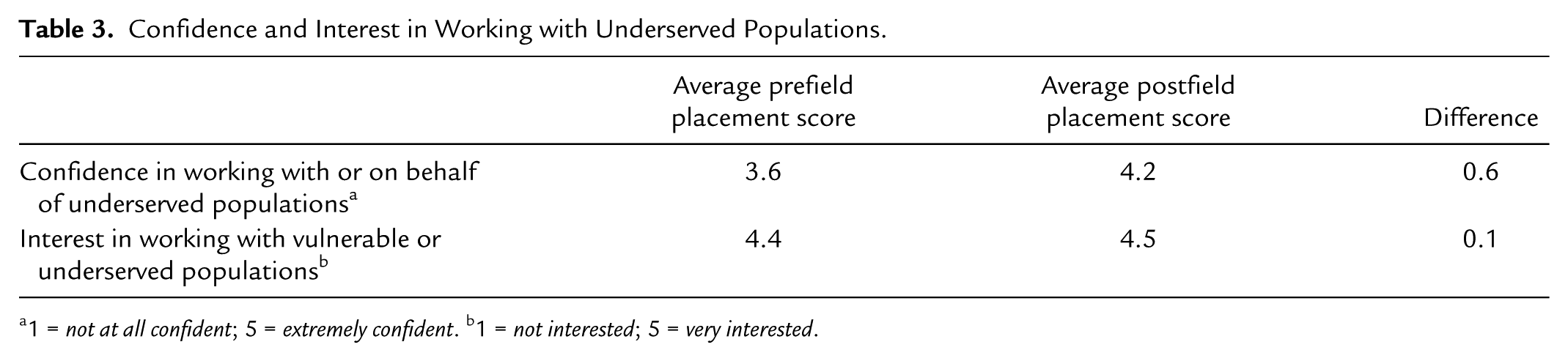
1 = not at all confident; 5 = extremely confident. b1 = not interested; 5 = very interested.
In their final evaluation survey, mentors were asked to rate the student’s proficiency in performing the selected competencies. All mentors who responded rated the students as proficient or extremely proficient in those competencies. Mentors were also asked to describe the impact of their scholar’s work on the agency. Examples of typical comments include the following: [The scholar] conducted an excellent analysis of the intersection of evidence-based home-visiting programs offered by the [health department] and patient-centered medical homes. [This] work has started a conversation about the future of both of these initiatives in [the state] and how they might align. The work [the scholar] did for us has actually been critical to completing several of our high-priority quality improvement projects, in addition to providing a new perspective on existing processes. We’ve already incorporated some of her findings and summaries into internal policies, plans, and procedure documents. [Scholar’s] work provided practical tools that were implemented as part of the daily work flow. Additionally, she provided an action plan which listed clearly stated objectives that assisted one program in planning for short- and long-term goals.
Eleven of 16 scholars responded to the 1-year follow-up survey for a response rate of 69%. Of those who responded, 100% are currently employed or have an official job offer. Currently, four respondents (36%) are employed with nonprofit organizations, two (18%) with the federal government, two (18%) with state public health agencies, one (9%) with a county health department, one (9%) with a community health center, and one (9%) with a government outside the United States. [Percentages do not add to 100% due to rounding error.] Two of the 11 respondents indicated that they are currently employed with the same agency for which they completed their field placement. Nine of the 11 respondents (82%) indicate they are currently working in the United States (two in Florida, two in Georgia, two in South Carolina, one in Kentucky, one in Massachusetts, and one in Pennsylvania).
Previous scholars were asked to indicate if they are currently employed in an MUC/P. Nine of the 11 respondents (82%) indicated they are currently employed in an MUC/P. Three of these nine respondents are also working in a rural setting. Scholars were also asked how their field placement experience affected their current career focus or career aspirations. Examples of typical comments include the following: It strengthened my aspirations for working with underserved populations. My experience with the __ Clinic greatly helped me in regards to my current career focus. As a Peace Corps Volunteer in Nicaragua in the health sector, I am able to use so many of the skills I learned in my internship to effectively plan interventions here in the field, especially a lot of the HIV-specific information. It helped me realize and develop my career interest in health data. Understanding the plight of medically underserved populations and those who are not afforded the same level of care as many of do have has pushed me to emphasize the importance of preventive medicine.
Discussion
The Pathways to Practice Scholars program evaluation findings indicate that experiential learning via competency-based field placements can enhance the ecology of public health in the southeast region by increasing scholar confidence and interest in working with MUC/Ps. Priority domains initially selected by scholars included analytic/assessment, policy development/program planning, and leadership/systems thinking. Scholars’ perceived confidence increased across all domains. However, the highest increases were in financial planning/management and cultural competency, possibly because these may be domains in which they had the least experience. Several of these domains align with priority training needs identified by the current public health workforce, based on assessment findings in Region IV (McCormick et al., in press).
While the primary goal was to enrich student experiences, the program likewise aimed to contribute to the current needs and practice of the mentors and host agencies. The R-IV PHTC also considered it a success that nearly one third of the scholars were placed in agencies outside the state of their home universities. This cross-pollination across the eight states enhanced the dynamic network of partnerships across the region. Through the program, new partnerships were forged and current collaborations were reinforced among the R-IV PHTC Central Office and LPSs, other colleges and universities, AHECs, and health departments in other states that hosted or helped to place students. In some cases, the field placements coincided with or directly supported collaborative efforts with partners such as workforce development trainings. Scholars developed products (e.g., action plans, community assessments, and quality improvement/strategic planning reports) that addressed multiple domains of the COL competencies and are currently being utilized by the agencies and communities. Notably, a number of alumni of the field placement program have continued to work postplacement in the same or similar agencies serving rural and/or MUC/Ps.
While successful in several dimensions, challenges and limitations included having only a limited number of funded slots (20 per year) for field placements to cover a large and diverse eight state region. Placements across states and universities posed challenges, such as varied semester timelines, deliverables, and hour requirements across universities, and the need of some agencies for memorandums of understanding with universities.
Process evaluation and partner feedback helped streamline processes and scholar deliverables. For example, student deliverables from home universities were accepted if they overlapped with the scholars program’s requirements. Rather than having scholars develop a final presentation of their experience (which the home institution may already require), scholars were instead asked to draft an abstract suitable for submission to a professional conference, an exercise that is useful for future public health practice.
Future Directions and Recommendations
Workforce needs have become more nuanced and complex, creating additional demand for specific competency-based training and mentorship across diverse public health occupations for long-term preparation and sustainability (Gebbie, 2000; Gebbie, Merrill, Sanders, Gebbie, & Chen, 2007). For the field of public health, expansion, funding, and increased focus on experiential learning through competency-based field placements are priorities for augmenting the future public health workforce. The R-IV PHTC plans to enhance the scholars program by building more robust mentorship infrastructure and professional development to equip the mentors as well as the students. In light of the projected short-term turnover in governmental public health (Sellers et al., 2015), this type of program can serve as a rapid response by increasing student confidence and interest to continue work after graduation with MUC/Ps through local, tribal, and state health departments, as well as AHECs and similar agencies.
Footnotes
Acknowledgements
We would like to acknowledge all of our Region IV Public Health Training Center colleagues at the Central Office and Local Performance Sites as well as the Steering Committee and practice partners who have provided support and input to the program. We would also like to thank our graduate assistant, Cidney Chanel Wilson, for her assistance with the literature review.
Authors’ Note
The information or content and conclusions are those of the author and should not be construed as the official position or policy of, nor should any endorsements be inferred by the Health Resources and Services Administration, the U.S. Department of Health and Human Services, or the U.S. government.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This program is sponsored by the Region IV Public Health Training Center which is supported by the Health Resources and Services Administration of the U.S. Department of Health and Human Services under Grant Number UB6HP27875-02-01, Affordable Care Act (ACA) Public Health Training Centers.
Supplement Issue Note
This article is part of a Pedagogy in Health Promotion: The Scholarship of Teaching and Learning supplement, “U.S. Public Health Learning Network: Innovative Competency-Based Training for the Public Health Workforce,” which was supported by the Society for Public Health Education and the Region IV Public Health Training Center, Health Resources and Services Administration of the U.S. Department of Health and Human Services under Grant Number UB6HP27875, Affordable Care Act (ACA) Public Health Training Centers. The entire supplement issue is available open access for one year at ![]() .
.