
Abstract
Objectives. A community-based training with core competencies in health insurance, health care resources, and outreach for over 1,700 Affordable Care Act navigators in Illinois from 2013 to 2014 was designed, delivered, and evaluated by an academic–community partnership with expertise in health care, social services, health policy, and community outreach. Methods. Pre- and posttraining scores on a knowledge-based certification exam were linked to navigators’ baseline sociodemographic characteristic. Additionally, self-reported training evaluation and posttraining support were summarized from an online follow-up survey of the workforce. Results. Although the material was initially unfamiliar and the population heterogeneous, the training program brought all identified subgroups from a below passing mean score (71%) on the pretest up to above proficiency (80%) in a posttest assessment—suggesting a highly accessible training program across navigator sociodemographic groups. Navigators reported additional training on Medicaid and marketplace structure and eligibility to be very important. Conclusions. Supplementing or replacing diminishing federal funding for consumer outreach workforce training and support at the state or community level was found to be an important priority that can increase competencies in a diverse population. Findings also indicated that the inclusion of ongoing wrap-around resources remain in high demand among navigators in the complex, ever-changing health care landscape in the United States.
Introduction
Funding for consumer outreach and education under the major 2010 U.S. health care reform, the Patient Protection and Affordable Care Act (ACA), has been a target for reduction or elimination under the current federal administration. As such, some communities and states are looking to bolster their workforce of ACA navigators and assisters locally to continue supporting consumers facing the increasing complexities of the U.S. health care and health insurance system. Originally established with state and federal grant funding in 2013, this workforce was developed to help consumers understand the ACA and guide them through the insurance enrollment process, which changed appreciably as part of the reform effort. In 2014, a series of ACA provisions regarding insurance coverage expansions were officially launched. Eligibility for the Medicaid program—the primary coverage vehicle for low-income populations in the United States—was greatly expanded, and a new Health Insurance Marketplace was created, providing subsidized coverage to populations both ineligible for Medicaid and lacking access to employer-based insurance, the largest source of private insurance plans in the United States.
ACA navigators had a broad range of prior work experience in public health and health promotion, ranging from novice level through long-term careers as community health workers, case managers, or care coordinators (Landers & Levinson, 2016; Lopez-Sanders, 2017; Pollitz, Tolbert, & Ma, 2014; Vargas, 2016). Aiding individuals in overcoming barriers to achieving health care goals has historically been a core function within these roles, however, adding health insurance navigation to that scope was novel. In many cases, the navigators were as new to the complex topics related to the ACA and health insurance as were the consumers they were working to assist. As a result, additional workforce training was needed, and the U.S. federal government developed an online certification program that provided approximately 5 to 20 hours of training. Some states chose to supplement this with enhanced local content. The federal government has since reduced or eliminated most funding for these programs leaving state and local stakeholders as the primary actors in supporting navigator-type work in the hopes of continued improvement in the rates of insurance coverage (Krisberg, 2017; Pollitz, Tolbert, & Diaz, 2018). While state and local training initiatives have enjoyed demonstrated successes across other areas of health promotion, including cancer patient navigation (Calhoun et al., 2008), client needs assessment (Ruiz et al., 2012), and emergency preparedness (Frahm, Gardner, Brown, Rogoff, & Troutman, 2014), to date, little evidence exists regarding the efficacy of these efforts to support insurance coverage goals.
Our study sought to address this gap in the literature by exploring the impacts of a community-based, in-person training effort in Illinois launched in support of the ACA rollout known as the Illinois Assister Training Program (IATP). With data drawn from trainees’ pre- and posttraining examination results as well as a posttraining online survey, we addressed the following specific research objectives:
Describe the development, content, and approach of the IATP.
Characterize the variation in baseline levels of knowledge about the ACA and health insurance–related topics among the socioeconomically heterogeneous navigator population.
Assess subject matter mastery following training, with a specific focus on the performance of subgroups demonstrating lower levels of baseline knowledge.
Gather navigator preferences regarding ongoing continuing education and workforce support with the goal of informing future curriculum development and other training activities.
Background
As introduced above, the ACA included several measures intended to increase access to health care, with a primary focus on reducing uninsurance rates in the United States. In 2013, approximately 14.5% of the national population was uninsured; in Illinois, the comparable figure was 12.7% of the population (1.6 million individuals; U.S. Census Bureau, 2014).
The ACA’s two key strategies to reduce the number of uninsured in the United States—expanding Medicaid and creating an online Marketplace—were both designed with an eye toward easing the enrollment and purchasing process of procuring health insurance. However, evidence suggests that low-income uninsured individuals remained largely unaware of potentially beneficial provisions of the ACA, even though these new provisions were promoted via traditional marketing channels including radio and television advertisements (Bias, Agarwal, & Fitzgerald, 2015; Long & Goin, 2014). To augment the marketing efforts, the ACA required that every state Marketplace also establish a navigator program at the 2014 insurance expansion launch. Recent studies outside of Illinois have found that the strongest predictor of an uninsured individual completing the Marketplace application process was receiving help with enrollment from a navigator or application assister, and conclude that support for ongoing funding for this type of work will be important to maintain or increase the gains in insurance rates for those not insured or for those underinsured (Call et al., 2015; Sommers, Maylone, Nguyen, Blendon, & Epstein, 2015).
To be eligible to be a grant-funded navigator program, organizations must have met a number of requirements, including being a community- and consumer-focused nonprofit group. Pursuant to the ACA regulations (Centers for Medicare & Medicaid Services, 2013b), the duties of a navigator include the following:
Offering expertise and education on eligibility, enrollment, and coverage details for each health insurance plan.
Facilitation of the enrollment process.
Provision of culturally and linguistically appropriate services.
Provision of referrals for conflict resolution for enrollees and complaints or concerns.
Navigator Policy Decisions in Illinois
In Illinois, public officials were very clear in their guidance to navigators that the role was intended to be one involving significant external community interaction, centered on reaching uninsured individuals and families to educate them regarding new insurance options (Illinois Department of Health Care and Family Services, 2013). The navigator grant selection process reflected this mandate: The state administered a competitive grant request for proposals for organizations hoping to participate and ultimately selected 44 organizations with demonstrated experience successfully serving communities with historically high uninsurance rates (Office of the Governor of Illinois, 2013). These state grantees supplemented the 11 federally funded navigator organizations operating in Illinois in 2013-2014 (Centers for Medicare & Medicaid Services, 2013a).
The state of Illinois also passed a statute requiring a rigorous certification process for all navigator grantees that significantly exceeded the federal requirements (Illinois General Assembly, 2013). In response, four health policy and administration faculty members from the University of Illinois–Chicago School of Public Health, joined by a team of four community partners spanning the legal, social work, and public policy professions, were hired to develop a training program that was considered to be among the most robust in the country (Benshoof et al., 2014). The University of Illinois–Chicago group was the sole provider of the training to over 1,700 individuals in the first rollout year (2013-2014), thereby creating a cohesive and consistent approach throughout the state.
Illinois Navigator Training Framework
The overriding goal of the training program was to enable navigators to become effective educators and community leaders regarding the Medicaid- and Marketplace-specific insurance provisions of the ACA as they pertained to low-income individuals and families. A key pillar of the program was the provision of a 2-day, in-person training. Between 2013 and 2014, 30 in-person navigator trainings occurred in a variety of settings, including university campuses, government buildings, and community centers. The training team described above, in partnership with state government officials, was also responsible for curriculum design. Training team members had considerable prior expertise in the design and delivery of health promotion continuing education curricula guided by adult learning principles, and the current training was motivated by the foundational adult learning theoretical frameworks pioneered by Knowles (1995). Per best practice, the team involved members of the learner community in all aspects of the learning cycle, from planning through evaluation (Bryan, Kreuter, & Brownson, 2009; Thompson, 2009). Moreover, the training approach focused on providing highly targeted, applied knowledge with immediate relevance to the participants’ new professional roles in the community. The in-person sessions employed a variety of learning modalities, including lectures, discussions, small-group breakout discussions, and an integrative “Jeopardy” game. The subsequent deployment of a navigator follow-up survey allowed the team to immediately design ongoing continuing education materials and areas of continuing technical assistance.
Training Structure and Objectives
The final curriculum encompassed 16 hours of in-person training preceded by 1 day (8 hours) of online state-based training. Topic areas covered during training are displayed in Table 1. The majority of the modules pertained to public and private insurance basics, including public insurance eligibility criteria, the mathematics of cost sharing in private plans, and postenrollment issues such as special enrollment periods triggered by qualifying life events. The training also focused on communication, outreach, and community engagement. Ethics and health literacy were also covered. Each navigator candidate was required to complete an online pretest prior to training initiation; the same instrument was subsequently administered as a posttest after training completion. A score of 80 was required to pass the posttest.
Illinois State Marketplace Assister Training Curriculum.

Another unique component of the community-based training program was the provision of significant follow-up support and engagement with the navigator population. The first follow-up training module was the provision of guidance on the particulars of using the Marketplace website, which, due to technical delays, went live after the in-person trainings. As mentioned above, the training team also fielded a follow-up survey that informed ongoing training and support efforts. Posttraining support included access to electronic training manual updates, online continuing education modules as required by the certification statute, access to an online resource repository, and the launch and stewardship of HelpHub. Unique to the state of Illinois, HelpHub is an online trainer- and peer-supported chat room and social platform designed to encourage troubleshooting and idea sharing for Illinois navigators. Given the breadth of material covered in a compressed time frame in the in-person curriculum, these wrap-around materials provided critical ongoing reinforcements and supplements to the training itself (Vargas, 2016).
Methods
We analyzed data reflecting pretraining and posttraining knowledge of the learning objectives displayed in Table 1, as assessed by the certification test created by the training team in conjunction with state officials. Of the 1,799 individuals who participated in the training, the test score sample (subsequently also referred to as “navigators” and/or “navigator sample”) included all 1,516 navigator candidates who completed the full certification process. There were a number of individuals including state employees, call center employees, and navigator organization program directors that attended training but were not required to complete the testing process. During the training enrollment process, self-reported data on sociodemographic and employment information were collected. Self-reported data were merged with the test score data to characterize differences in scores across sociodemographic categories for the navigator sample.
We also present data from a navigator follow-up survey fielded during the initial open enrollment period (February to April 2014), about 1 month after the final training had been conducted. The survey was administered to all certified navigators who completed the training and certification process, and were still in their roles as of survey administration (n = 1,116). The response rate was 69.5% (n = 776). This group is subsequently referred to as the “survey sample.” All data collection activities were submitted to the University of Illinois–Chicago institutional review board, which deemed them exempt from further human subjects review. Analyses were conducted using Stata software (version 15). The primary statistical methodology was descriptive in nature, including frequencies and measures of central tendency. Multivariate regression was also used to estimate independent associations among sociodemographic attributes and test score performance.
Results
Performance on Pre- and Posttraining Certification Exam
Table 2 contains descriptive statistics of the test score sample. Notably, the navigators exhibited considerable diversity across all sociodemographic characteristics except gender. Over three quarters (80.6%) of navigators were female. In contrast, no single race, education, or age group comprised a majority of individuals. A total of 41.3% of navigators identified as White, non-Hispanic, while 19.7% identified as Black and 25.5% identified as Hispanic. Having some college experience or a college degree were the most frequent education categories (31.0% and 30.4%, respectively), and more than one quarter (28.4%) of navigators had completed post-collegiate levels of education. The navigators’ ages ranged widely, with approximately one quarter younger than 30 years and approximately one third age 50 years or older. A plurality (44.4%) of navigators were employed by community organizations, with 23.9% employed by health care providers, 18.7% by the government (e.g., local public health agencies), and 13% by other types of organizations. Examples falling into this “Other” category include the following: faith-based, insurance agency, or broker, legal, and bank. While a majority (57.2%) of navigators obtained their own personal insurance through an employer-based policy, sizeable percentages were insured by public programs (11.8%) or were uninsured (13.1%). The average score on the pretest was approximately 9 points below the passing rate (mean of 71.0).
Navigator Summary Statistics.
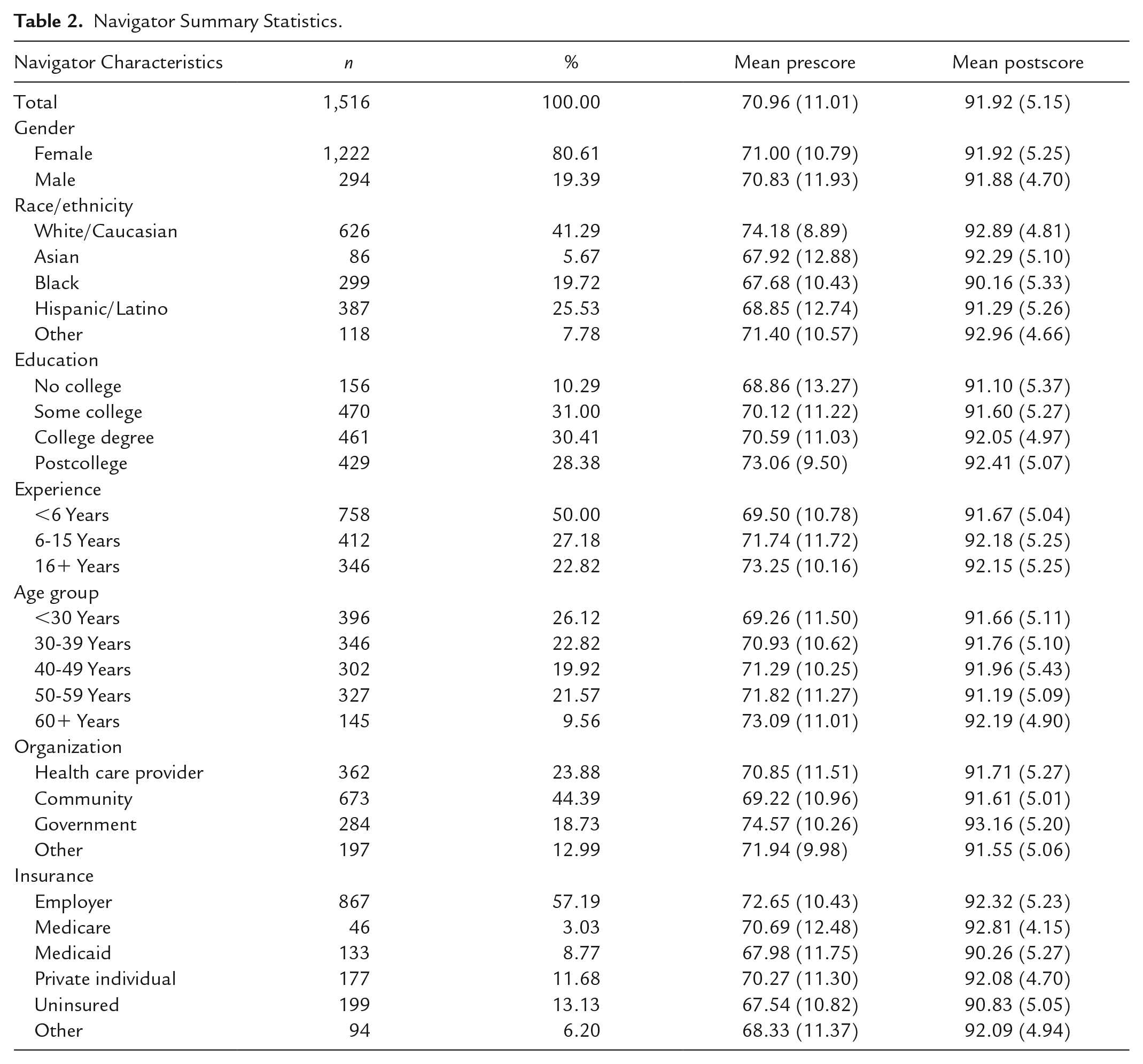
While there was distinct heterogeneity in pretest scores across all sociodemographic groups except gender, no individual group had an average score above the passing rate. Among race/ethnicity groups, Whites had the highest average pretest score (mean of 74.2), and Blacks and Asians had the lowest (mean of 68.0 for both groups). In keeping with other types of patient navigator training programs, both education and experience were positively correlated with higher pretest scores (Calhoun et al., 2008). Older navigators had higher pretest scores on average relative to their younger peers, and government employees had the highest pretest scores across organization type. Insurance coverage was also associated with pretest scores. Navigators covered by employer-sponsored health insurance coverage scored the highest across insurance categories (mean of 72.7). Navigators covered by Medicaid or Other coverage (e.g., parent, VA, university program/student insurance, Tricare), and those without insurance coverage scored the lowest (mean of 68.0).
Posttest scores across sociodemographic subgroups were higher than pretest scores across the navigator sample by an average of 21.0 points, with a mean posttest score of 92.0 points, well above the 80-point passing threshold. While some sociodemographic differences remained in the posttest scores, these differences were considerably smaller than those seen among the pretest scores. This resulted from the fact that the navigator subgroups with the lowest pretest scores achieved the highest gains in test scores. All subgroups experienced appreciable gains. The smallest gain across subgroups was 18.7 points (for the White, postcollege, 16+ years of experience, and government employee subgroups). Higher gains, on the order of 22 to 24 points, were achieved for the groups with weaker pretest performance.
The multivariate regression results in Table 3 demonstrate the independent associations between each sociodemographic variable and pre- and posttest scores. The largest independent associations for pretest scores were seen among race/ethnicity groups. Black navigators and Asian navigators scored an average of 5.2 points and 4.5 points lower than White navigators, holding all other sociodemographic characteristics constant. Large independent associations were also seen for education levels and insurance status. Lacking any college experience was associated with a 3.4 point decrease in pretest score relative to having a postcollege degree; having some college or a college degree was associated with a 2.6 and 2.3 decrease, respectively. Lacking coverage and having other coverage were independently associated with a decrease of 2.6 and 2.7 points, respectively, relative to having employer-sponsored coverage. While the independent associations between having Medicaid or Medicare with pretest scores were negative, they did not reach statistical significance. No statistically significant independent associations arose for experience or age group, moreover, none of the point estimates for these associations were of meaningful magnitude. The independent associations between sociodemographic groups and posttest scores demonstrate markedly greater concordance relative to those derived from the pretest regression. Alternatively stated, there were many fewer independent associations that were statistically significant and/or clinically significant. Illustratively, the largest independent association of 2.4 points (Blacks vs. Whites) was less than half the magnitude of its analog in the pretest regression (5.2 points). In synthesis, the independent associations between sociodemographic groups and pretest scores were either greatly reduced or completely gone when examining posttest scores.
Summary of Regression Analysis for Navigator Assessment Performance (N = 1,516).
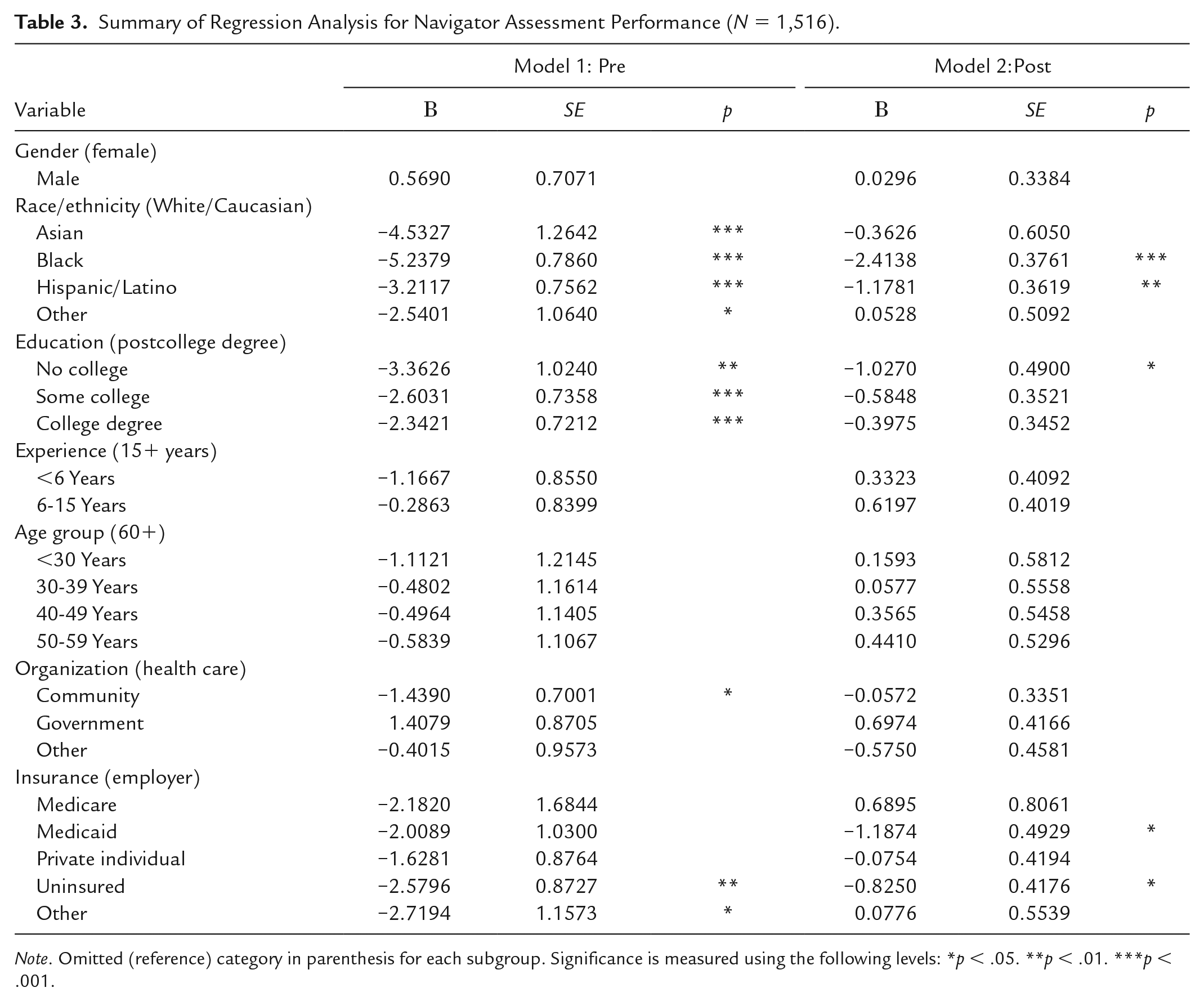
Note. Omitted (reference) category in parenthesis for each subgroup. Significance is measured using the following levels: *p < .05. **p < .01. ***p < .001.
Navigator Evaluation of Training and Support Needs
The navigator survey asked for respondents’ self-reported future training needs. In Table 4, for each domain, a vast majority of respondents indicated that the domain was at minimum “somewhat important” to cover in future initiatives. Across domains, there was appreciable heterogeneity in reported importance. Training domains focused on technical knowledge about Medicaid and the Marketplace were considered to be the most important; over three quarters of the survey sample indicated these domains as “very important” for future training. Eligibility issues (e.g., income, tax filing status) also had high scores, with over two thirds of sample respondents reporting these modules as “very important.” While the domains pertaining to navigating the online enrollment systems did not score as high as the technical knowledge domains, a majority of navigators considered them to be “very important” topics for future training. Less than half of sample respondents reported that outreach, organizational skills, and communication/interpersonal skills were “very important” for future training. Similarly, lower levels of importance were reported for tailored knowledge about special populations.
Respondents’ Self-Reported Future Training Needs (N = 703).
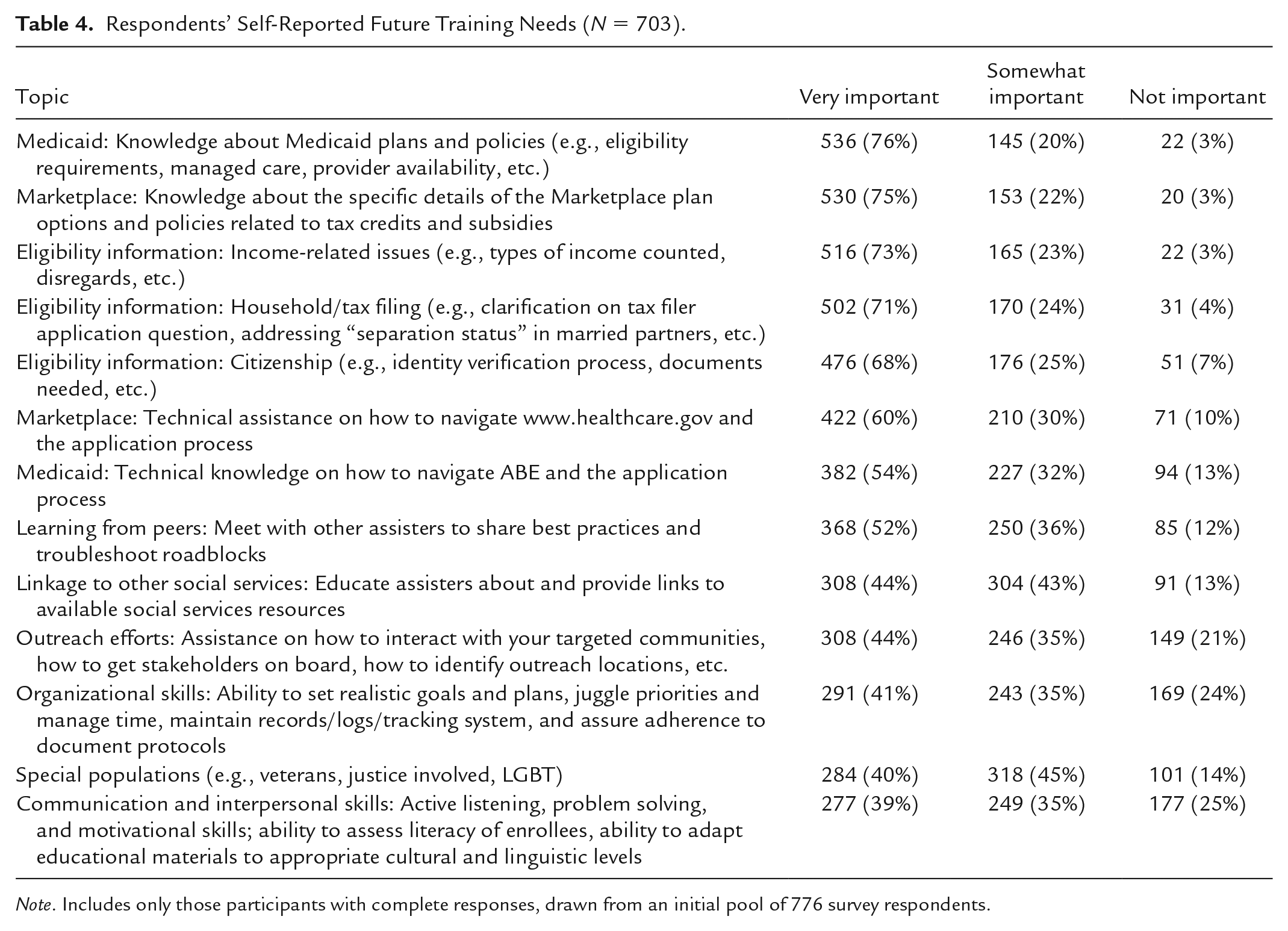
Note. Includes only those participants with complete responses, drawn from an initial pool of 776 survey respondents.
Finally, we examined results (available on request) providing insight into the navigators’ reports of the usefulness of various resources in doing their job. The support of coworkers was ranked highest (74.1% responded affirmatively), and the initial binder of training materials ranked second highest (63.4% responded affirmatively). No other type of resource—including the variety of online tools and supports such as webinars, general self-guided internet searches, state-provided resource repositories, required continuing education modules, and the use of HelpHub—earned a majority of affirmative response. The lowest ranked source of support was the federal Marketplace staff; with only 28.7% of navigators indicating that Marketplace staff was a useful source of support.
Discussion
Although the material was initially unfamiliar and the population heterogeneous, the training program brought all identified subgroups from a below passing mean score (71.0%) on a pretest up to above proficiency in a posttest assessment—indicating a highly accessible training program across sociodemographic groups. The community-based training program in Illinois gave the diverse navigator population a strong foundation to educate, enroll, and guide the previously uninsured to obtaining health insurance coverage.
A posttraining follow-up survey revealed ongoing need for additional technical knowledge. Navigators highlighted Medicaid and Marketplace plan and policy information as the most important domains for continuing education. These domains remain complex and important, as the implementation of related ACA provisions continues to change rapidly. Although the IATP material was comprehensive, given the complexity of the ACA, it was common for navigators to encounter consumer questions they were unable to answer easily. The Kaiser Family Foundation reported that 89% of ACA assisters throughout the country worked with consumers who had questions that were not easily answered by the Marketplace website, with over 40% of them stating that this happened either “often” or “always” (Pollitz et al., 2014). The IATP provided a number of posttraining, online-based supplemental resources to assist the navigator workforce with these difficult questions or scenarios, including virtual access to the trainers via HelpHub. Notably, even though state- and federal-navigator programs have matured since the IATP, the associated complexity of consumer questions has remained high, requiring navigators to continue to gather and triage information from a wide variety of sources (Pollitz, Tolbert, & Semanskee, 2016).
In keeping with related research, there are important limitations to consider. First, there could be some concern of test–retest bias on the knowledge-based examination. We acknowledge this concern, but emphasize that it does not account for the dramatically reduced variance in scores across subgroups in the postperiod relative to the preperiod. In addition, for the follow-up survey we should be concerned about response bias—and whether our sample represents the broader population studied. In comparing our baseline sociodemographics between the responders and nonresponders, we find very few significant differences. However, White navigators are slightly overrepresented and Black navigators slightly underrepresented. We also recognize that this study is limited to navigators in the state of Illinois, and may not be generalizable to dissimilar geographies. Finally, the IATP was a relatively well-funded, intensive effort, and its apparent successes may not generalize to “lighter touch” training programs.
Conclusion
The ongoing reduction in federal funding for insurance-related consumer outreach and education continues to shift related responsibilities to states and local communities. Meeting these responsibilities requires the development of sound competency- and community-based training that is accessible for an evolving and diverse workforce. The IATP provides a promising model for future efforts, having achieved success using a community–academic partnership model grounded in adult learning principles. Importantly, the program built in meaningful opportunities for ongoing feedback from the newly trained workforce and continuous improvement of the material and supportive structures. Future evaluations of how training directly links to insurance enrollment are needed; however, we believe that our results are instructive both for planning future insurance outreach efforts, as well as ongoing workforce training/patient navigation training efforts seeking to target other domains of health promotion. This study’s results highlight that the public health workforce, when tasked with promoting complex and novel initiatives like the ACA insurance provisions, can be brought to competency when provided with face-to-face training, ongoing follow-up education, and the use of new media tools and virtual social platforms to engage with topic area experts. Each of these resources requires investment to provide and maintain, but are critical if we intend to continue progress toward reducing the uninsurance rates throughout our communities.
Footnotes
Acknowledgements
We are grateful for the training and curriculum contributions of our former colleagues and community partners. Special thanks goes to Stephanie Altman, Stephanie Becker, John Coburn, Jon Dopkeen, Brian Gorman, Kristin Hartshaw, Jennifer Koehler, Jennifer McGowan, and Kathryn Nelson.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interests with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a community training grant from the State of Illinois Department of Insurance to support ACA Navigator implementation (Grant Number 2013-0664).