
Abstract
Introduction. Experiential learning activities, such as simulations, strengthen student learning by allowing students to apply didactic knowledge to real-world settings. Moreover, simulation-based interprofessional education supports teamwork and skill development as outlined in accreditation standards for many health and health-related academic programs. The purpose of this article is to describe the role of interprofessional simulation in enhancing student knowledge and promoting collaborative practice for disaster management. Method. Multiple data sources were used to assess a simulated EF-5 tornado disaster event including an observational protocol, a disaster simulation survey, and a survey from the Office of Interprofessional Simulation for Innovative Clinical Practice. Results. Students reported increased satisfaction and knowledge with applying skills associated with interprofessional practice, including communication, teamwork, and collaboration. Additionally, students identified skills that could be broadly applied to a range of work settings on graduation such as seeking role clarity, utilizing job action sheets, and responding to a complex situation. Notably, students reported increased levels of knowledge gain of the incident command structure after applying knowledge from didactic sessions to the simulation. Conclusion. Simulation is an innovative strategy for integrating theory and practice to best prepare graduates for the dynamic world in which they live and work. Experiential learning opportunities appeal to the assumptions of adult learning, promote the skills that employers value, and bridge the competencies of multiple academic disciplines that frequently operate in silos. Institutional leaders should view experiential learning as a critical component of student learning and an investment in workforce development.
In an effort to increase the workforce readiness of students in health professions, the University of Alabama at Birmingham (UAB) Schools of Public Health and Health Professions coordinated with the UAB Office of Interprofessional Simulation for Innovative Clinical Practice (OIPS) to create a discussion-based tabletop exercise for health administration and public health students. Emergency Management Services International (2018) defined a tabletop exercise as an activity designed to generate discussion of various issues regarding a hypothetical simulated emergency. Graduates in public health and health professions are frequently expected to work collaboratively to care for individuals and communities; therefore, academic programs are encouraged to promote interprofessional education (IPE) opportunities as part of curricular offerings (Robert Wood Johnson Foundation, 2015). Simulation is one evidence-based strategy to implement IPE (Costello et al., 2017).
The collaborative nature of disaster management requires a more active, learning-centered environment than the traditional lecture style of instruction that is predominantly offered at the postsecondary level in the United States (McSweeney-Feld et al., 2017; Prosser & Trigwell, 1999). Through simulation-based IPE, students develop competencies of interprofessional practice outlined by the IPE collaborative, including values/ethics for interprofessional practice, roles/responsibilities, interprofessional communication, and teams/teamwork (Interprofessional Education Collaborative, 2016). Moreover, simulation-based IPE supports skills development as outlined in accreditation standards for many health and health-related academic programs (Zorek & Raehl, 2013). The purpose of this article is to describe the role of interprofessional simulation in enhancing student knowledge and promoting collaborative practice for disaster management.
Background
For the past 2 years, the Masters of Science in Healthcare Administration (MSHA) program in the School of Health Professions at the UAB has hosted a disaster preparedness week to increase student awareness of the challenges they may face while working as future health care administrators during a disaster. Disaster preparedness week was developed and implemented after the MSHA program received feedback from alumni that disaster preparedness and management needed to be incorporated into the curriculum to better prepare students for future roles in hospitals and health care settings. Following the first year, the MSHA program contacted colleagues from the School of Public Health who had expertise in the Incident Command System (ICS). Over the next 6 months, representatives from OIPS, public health, and the MSHA program met regularly to plan the simulation and modify existing disaster simulation materials from the Centers for Disease Control and Prevention.
The culminating event of disaster week is a discussion-based simulation that models an unfolding disaster event. In fall 2019, the simulated disaster was an EF-5 tornado that touched down in “Anytown, USA.” In the simulation, graduate MSHA and undergraduate public health students were provided the disaster scenario and assigned key roles within the ICS of two simulated hospitals and a simulated health department. Public health students acted as public health officials while health administration students simulated roles of the ICS, including incident commander, public information officer, liaison officer, safety officer, operations section chief, planning section chief, logistics section chief, and finance and administration section chief. In whole group discussions, students collaborated across disciplines to make high-level decisions necessary to respond to the simulated disaster.
In light of the global pandemic (COVID-19), the need for a skilled workforce to manage adjusted operations in health care and public health is greater than ever. Graduates of these programs will face unprecedented challenges in responding to operational, political, and financial constraints that affect the public health and health care response. New and emerging crises will require individuals to work interprofessionally to address the political, economic, sociocultural, environmental, and other external factors endemic to the 21st century.
Theoretical Framework and Literature Review
We framed this simulation through the lens of andragogy and experiential learning theory. Andragogy, or adult learning theory, describes five basic assumptions of adult learning: self-concept, experience, readiness to learn, orientation to learning, and motivation. Experiential learning is a process of learning in which “knowledge is created through the transformation of experience” (Kolb, 1984, p. 38). Knowles (1980) emphasized the use of experiential methods such as simulation to engage adult learners and build on their life and professional experiences.
Simulations are also used to familiarize students with the concept of IPE and have been endorsed by the World Health Organization (WHO, 2013) as an effective method of teaching students across health-related disciplines how to effectively work in teams. According to the WHO (2010), “Interprofessional education occurs when students from two or more professions learn about, from and with each other to enable effective collaboration and improve health outcomes” (p. 7). Recently, literature has begun to emerge describing the use of simulations among students in public health and health administration (Barrett et al., 2017; Livingston et al., 2016), although less has been written about students in these disciplines as compared to students preparing to provide direct patient care.
Simulation Design and Implementation
Incorporating evidence-based practices into the simulation was a priority during the design phase. Content experts in health administration, public health, emergency management, and simulation met regularly to develop mutual objectives and discuss the details of the scenario. The goal of the simulation was to encourage learners to apply what they had learned throughout their didactic education on disasters and ICS. To ensure learners had a full understanding of ICS prior to the simulation and could apply their new knowledge, students participated in multiple classroom lectures, expert panels, and online trainings through the Emergency Management Institute (Federal Emergency Management Agency, 2015).
Thirty three health administration and seven public health students participated in the simulation, which was facilitated by practicing public health professionals and content experts. Facilitators had expertise in health care, public health, and the ICS and acted as a simulated emergency management agency. Practice partners from UAB Medicine and Health System and a local health department were embedded in the simulation to help guide the scenario and provide timely information.
The simulation occurred during one (3.5 hour) session and began with a (30-minute) prebrief and orientation followed by four (30 minute) simulated rounds. Predebriefing sets the stage for a psychologically safe environment in which learners can practice to the limits of their expertise by promoting buy-in from students, establishing confidentiality, clarifying roles and expectations, and conveying a commitment to respecting the learners (Rudolph et al., 2014).
For each round, students were presented with a news report/scenario update. In small groups (two hospitals [MHA students] and one public health department [PH students]), students were tasked with reviewing the information provided, exploring available resources, determining priorities for their organization based on didactic sessions, and completing their role’s job action sheet. Job action sheets are essentially job descriptions; they tell disaster response personnel “what they are going to do; when they are going to do it; and, who they will report it to after they have done it” (Health Emergency Incident Command System, 2020, p. 1). After internal discussions, the assigned incident commander from each organization summarized their team’s priorities and decisions for each round of the simulation. Similar to a real disaster, incident commanders were responsible for all aspects of their organization’s response. Following reports, facilitators led a short in-sim group debriefing.
Essential learning occurs during the debriefing (Levett-Jones & Lapkin, 2014); therefore, after the simulation (60 minutes), a whole group, learner-centered, structured debriefing with good judgment approach (Rudolph et al., 2006) was utilized to explore the following topics: (1) challenges associated with roles within the Hospital Incident Command System, a standardized approach to managing complex incidents in health care environments; (2) management of information and documentation throughout the simulation; and (3) coordination of services and resources during the disaster. The “debriefing with good judgment” approach allows debriefers to explore the frames of the learners and share their expertise while avoiding merely correcting a student’s decision without promoting reflection or “sugar-coating” errors. This approach allows for open dialogue between students and debriefers. It creates a space in which students can make errors and through inquiry and reflection debriefers and content experts can foster deep learning with the students. At the end of the simulation, students were able to demonstrate their organization’s response to the disaster based on completed job action sheets. However, simulation designers regarded the greatest deliverables from the event as student engagement with peers from other disciplines, improved understanding of role clarity and scope of practice of HA and PH professionals, increased knowledge of the ICS, and greater awareness of the interprofessional nature of disaster management. The session concluded with evaluations and wrap-up. An overview of the simulation by rounds can be found in Figure 1.
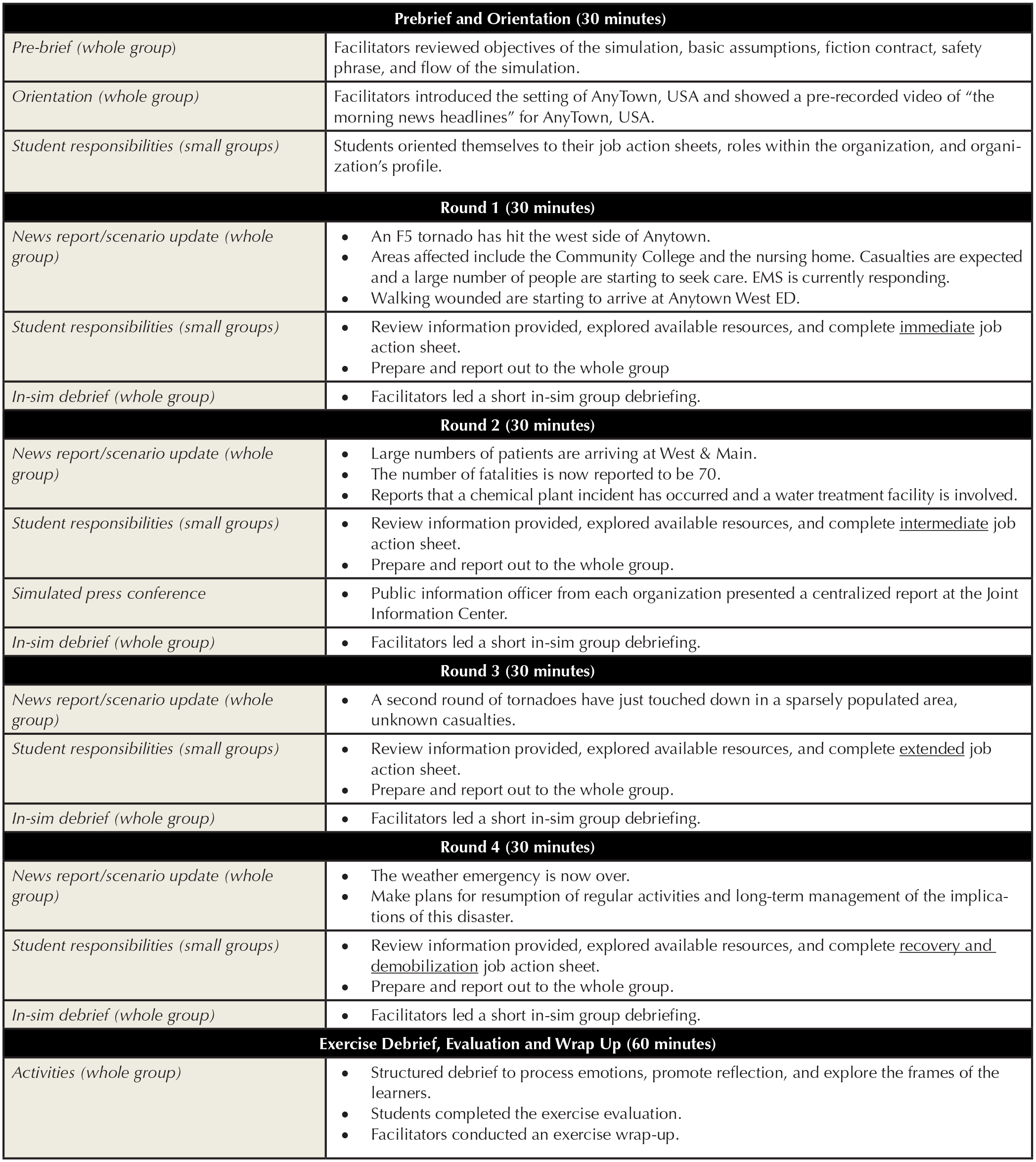
Overview of simulation.
Method
Our research team used multiple data sources to assess the simulated EF-5 disaster event including an observational protocol, a Disaster Simulation survey, and a general survey from UAB OIPS. The Disaster Simulation survey was distributed electronically via Qualtrics, a web-based survey platform. The OIPS survey was distributed via paper-and-pencil at the conclusion of the simulation. All data were anonymous. This research was classified as exempt by the UAB institutional review board (IRB-300005320).
Disaster Simulation Survey
The Disaster Simulation survey was composed of three questions. The first two questions captured student knowledge before and after the simulated activity regarding the following domains: (1) ICS sections and roles, (2) job action sheets to perform necessary actions, and (3) coordination of services to respond to a disaster. The third, open-ended question asked students to identify the “most important thing” they learned about disaster preparedness/response from the simulation. This survey was distributed on the same day as the disaster simulation, immediately following the activity. Questions were developed by the simulation planning team based on learning objectives.
Office of Interprofessional Simulation Survey
All simulations through UAB OIPS are evaluated using a standardized, 11-question survey. For the purpose of this research, the most salient questions focused on teamwork, communication, and IPE, as well as one open-ended question related to learning. Since the simulation was focused on these broad concepts, learning outcomes were not differentiated between undergraduate and graduate students.
Observation Protocol
The observation protocol included discrete sections to record notes for each “location” (i.e., hospitals, health department) as well as overall impressions. Additionally, the observation protocol provided space to summarize notes from the final debrief discussion with facilitators, controllers, subject matter experts, and students. The disaster simulation planning committee developed the observation protocol and an undergraduate public health student intern used it to record the day’s events.
Data Analysis
Pre- and postknowledge questions on the Disaster Simulation survey were based on mean averages with differences calculated between scores. The UAB OIPS instrument recorded mean scores and standard deviations. For all qualitative data, the research team reviewed student statements line-by-line to develop emergent themes. Team members discussed disagreements of coding until consensus was reach. Consistent with best practices in qualitative methodology, we used multiple methods of verification to ensure trustworthiness of the data, including peer debriefing, internal memoing, and an audit trail (Creswell, 2007).
Results
Observation Protocol
According to the student observer, participants experienced initial confusion at the beginning of the simulation as they familiarized themselves with their respective roles and assignments, “Everyone was talking loud and scrambling to find information as fast as possible.” Participants assigned to the health department also appeared to struggle with issues related to prioritizing decisions and utilizing the chain of command to deliver a unified message due to incomplete information. The observer suggested that individuals gained confidence as the simulation continued, as demonstrated by streamlined communication and delegation of tasks to small work groups.
At the conclusion of the simulation, students reported feeling a sense of “relief” that the crisis was over. They commented on the value of structure and clear lines of communication to coordinate resources and suggested that “team huddles” after each update increased their situational awareness, thereby improving their ability to coordinate services and care. Multiple students described the value of simulation as a form of experiential learning. For example, one student stated, I really appreciated the simulation because as a student . . . we learn things in the classroom, but by practicing and getting out in the simulated field we are able to really apply the things that we learned in the classroom.
Another student commented on the design of the simulation, “I also thought it was very important to work in an interdisciplinary (group) because that’s what these disasters take.” There was consensus among participants that engaging in simulations like this one will better prepare them both personally and professional for a real-life emergency situation.
Disaster Simulation Survey
Results from the Disaster Simulation survey demonstrated that student knowledge increased in all three knowledge domains. Prior to the simulation, students described their level of knowledge as “low” regarding incident command roles and responsibilities and associated tools for managing a disaster response. After the simulation, self-reported scores demonstrated “moderate to high” levels of knowledge, with the greatest gains made in student understanding of the job action sheet to perform necessary actions (+1.55; see Table 1).
Average Pre- and Postassessment of Disaster Simulation Knowledge.

Note. Scoring rubric: 1 = None, 2 = Low, 3 = Moderate, 4 = High.
A review of open-ended comments in the Disaster Simulation survey yielded four primary themes: role clarity (n = 8), communication and collaboration (n = 6), value of practice (n = 5), and facts and documentation (n = 4). Key quotes are provided to illustrate each theme. Students identified roles and role clarity as critical to effectively managing the situation. For example, one student described their most important learning as “understanding everyone’s respective roles and what they aimed to accomplish in each step of incident command.” Similarly, students expressed the importance of communicating and collaborating with members of their team. Students observed that individuals engaged in team huddles to communicate “needs and actions between the different sectors . . . responding to a disaster.”
Like all tabletop exercises, this disaster simulation was designed as a low stakes activity in which students could experience the realities of a disaster response without facing the real-world consequences of injury and loss of life. One student captured this lesson, stating, “I learned that practice is so important.” Another simply wrote, “Practice, practice, practice.” As an evolving situation, students noted that they were inundated with information and had to keep up with the latest developments. One student reported, “The most important thing I learned is that factual flow of information is important to making the right decision in a timely manner.” Facts included both decisions that were made as well as documentation for the purpose of reimbursement.
OIPS Survey
Results of the OIPS survey indicated a high level of agreement among participants regarding statements of program components including objectives, learning, debriefing, and future performance as well as their willingness to recommend the program to others. Taken together, these statements represent a composite of student satisfaction (see Table 2).
Overall Satisfaction.
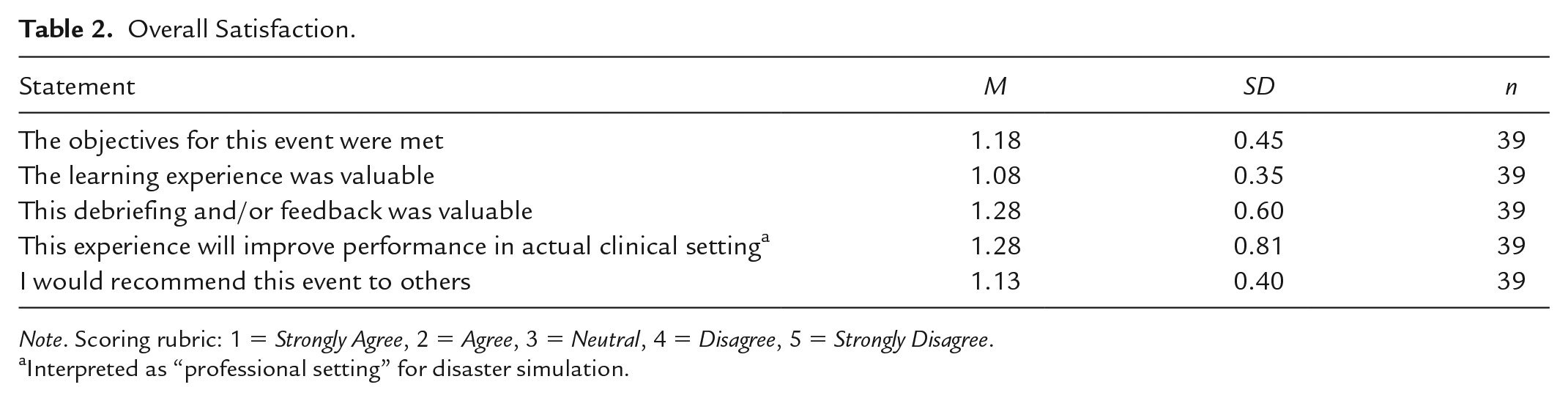
Note. Scoring rubric: 1 = Strongly Agree, 2 = Agree, 3 = Neutral, 4 = Disagree, 5 = Strongly Disagree.
Interpreted as “professional setting” for disaster simulation.
The OIPS survey also assessed student experiences with teamwork and communication. Once again, there was consensus among participants that these objectives were met and their skills improved based on the experience (see Table 3).
Teamwork and Communication.

Note. Scoring rubric: 1 = Strongly Agree, 2 = Agree, 3 = Neutral, 4 = Disagree, 5 = Strongly Disagree.
In response to the two things they “liked/learned” from the experience, students identified the importance of communication (n = 5), the structure of the ICS (n = 5), and the complexity of disaster response (n = 4). Students commented on the necessity of clear and consistent communication between local and state partners as well as with the general public. One student wrote, “Communication and coordination between staff and the community is key.” Several students commented on the invaluable knowledge they gained regarding the ICS for consistent crisis reporting as well as understanding the different roles involved in disaster response. One student stated, “I gained a better understanding of roles of (the) incident command system. I learned how to collaborate and pull together a unified message.” Students also acknowledged the complexity of dealing with an emerging crisis, especially in a health care setting and the value of “working with outside resources to improve/manage care.”
Discussion
In fall 2019, graduate and undergraduate students in Health Administration and Public Health at the UAB engaged in a tabletop disaster simulation to address the emergent community and health care needs after an EF-5 tornado stuck “Anytown USA.” Students assumed key roles as hospital administrators and public health officials in an ICS and were tasked with collecting and interpreting incoming data, prioritizing decisions, and communicating messages to multiple stakeholder groups. Consistent with best practices in experiential learning, experts were available to help students process the experience through large and small group reflective debriefings (Moon, 2004).
Across academic disciplines, students reported increased satisfaction and knowledge with applying skills associated with interprofessional practice, including communication, teamwork, and collaboration (Interprofessional Education Collaborative, 2016). Additionally, students identified skills that could be broadly applied to a range of work settings on graduation such as seeking role clarity, utilizing job action sheets, and responding to a complex situation. Both survey and open-ended responses indicated that students developed a greater understanding of the ICS and the importance of coordinating services in response to a disaster. Despite the limitations of self-reported data, knowledge gain of the ICS occurred after students completed multiple didactic and online Federal Emergency Management Agency training modules, which demonstrates the power of experiential learning as students applied their previous knowledge within a low-stakes environment (Kolb, 1984).
Limitations
Findings were based on a small yet purposeful set of students who participated in this tabletop disaster simulation. Findings cannot be generalized beyond the context in which the research was conducted. Due to the small sample size, we were limited in our ability to interpret results of the quantitative data beyond practical utility and program improvement. Moreover, scores represented self-reported data by students, which introduces the potential for social desirability bias (Grimm, 2000). Finally, data reflected only the first two levels of Kirkpatrick’s training evaluation model (reactions and learning; Kirkpatrick & Kirkpatrick, 2006).
Implications
Increasingly, academic programs are requiring IPE in their curricula to satisfy changes in accreditation requirements (Zorek & Raehl, 2013). This shift toward practice-based learning is in response to employer expectations for new graduates to possess the skills necessary to work as effective team members, regardless of their academic preparation (Archer & Davison, 2008). As a research team, we see simulation as an innovative strategy for integrating theory and practice to best prepare our graduates for the dynamic world in which they live and work (Brashers et al., 2015). Moreover, we advocate for more academic programs to work across disciplines to provide students with rich and meaningful learning opportunities in applied settings. However, we also recognize that certain institutional changes would need to be made for programs to effectively heed this call to action.
To prioritize IPE through simulations, institutional leaders would need to address issues related to scheduling, faculty training, and resources. Like many institutions, there are currently no blocks of time at the UAB that are solely dedicated to bringing together different academic disciplines and programs to plan and execute IPE offerings. Developing this tabletop exercise required extensive planning and coordination among professionals in multiple disciplines whose schedules were frequently filled with competing demands. Moreover, student participation in this disaster simulation occurred outside of posted class meeting times and required students to rearrange their schedules to engage in this simulated learning activity. Common planning times for innovative course offerings and activities would likely foster greater collaboration within and across academic programs and departments and promote student participation in IPE.
An institutional commitment to faculty development in the area experiential learning would need to be made to transform curricular offerings from largely lecture-style didactic sessions to more interactive, applied learning activities. Furthermore, the vast majority of simulations in the research literature addresses the clinical needs of emerging health care professionals in medicine, nursing, and allied professions. To effectively meet the needs of students in health administration, public health, and nonclinical programs, resources would need to be created or modified.
Conclusion
Experiential learning activities, such as simulations, strengthen student learning by allowing students to apply didactic knowledge to real-world settings. As such, experiential learning opportunities appeal to the assumptions of adult learning, promote the skills that employers value, and bridge the competencies of multiple academic disciplines that frequently operate in silos. As accreditation standards continue to shift to reflect the expectation that graduates possess both theoretical and practical knowledge, institutional leaders should view experiential learning as a critical component of student learning and an investment in workforce development.
Footnotes
Acknowledgements
The authors thank the following people for their vital contributions to the design and implementation of the simulation: Marjorie Lee White and Andres Viles from the Office of Interprofessional Simulation from Innovative Clinical Practice, Sarah Nafziger from UAB Emergency Medicine, Bill Mayfield and Stacey Benson from UAB Medicine Emergency Management Department, Julie Cobb from the Jefferson County Department of Health, and James Spann from ABC 33/40.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.