
Abstract
Competency-based education (CBE) is an outcome-oriented instructional approach that ensures students master essential skills before advancing. In public health education, CBE aligns with professional competencies set by several accrediting bodies to prepare graduates for workforce demands. This repeated measure quasi-experimental study evaluates student self-efficacy in applying professional skills within a restructured Master of Public Health program designed under a CBE framework. A 2-year pilot assessment guided the program’s redesign, focusing on competency alignment, curriculum mapping, and skill development. Initial evaluations identified gaps in applied learning, prompting course restructuring to emphasize hands-on experience and higher-order cognitive skills. The redesigned program introduced a cohort-based model, service-learning integration, and a boot camp to ensure foundational knowledge consistency. A culminating Graduate Student Symposium provided students with an opportunity to showcase their applied skills to industry professionals. By examining student self-efficacy within this framework, this study highlights the impact of CBE on professional preparedness. Findings contribute to ongoing discussions on best practices in graduate public health education and provide insights for educators and policymakers seeking to enhance training models. This study underscores the significance of CBE in fostering confidence and competence in public health professionals, ultimately strengthening workforce readiness.
Keywords
Background
Competency-based education (CBE) is an outcome-oriented instructional approach that focuses on the mastery of specific skills and knowledge, as compared to traditional time-based progression (Harden, 2002; Morcke et al., 2013). In such a model, students advance upon demonstrating proficiency in clearly defined competencies, which align with professional standards and relevant workforce needs. Today, CBE is widely utilized across various disciplines, including in health professions education, to ensure graduates acquire the essential skills required for effective practice (Calhoun et al., 2005, 2011). Accrediting bodies, such as the Council on Education for Public Health (2025), National Center for Healthcare Leadership (2025), the Accreditation Council for Graduate Medical Education (2025), among others, emphasize competency-based frameworks to assess educational quality and student preparedness.
Furthermore, CBE’s emphasis on applied knowledge, adaptability, and continuous assessment has gained traction due to its ability to enhance workforce readiness, accountability, and educational outcomes in fields requiring specialized expertise (Anderson, 2018; Mursalin et al., n.d; Williams, 2013). For example, a study evaluating the efficacy of competency-based global health education (GHE) program for medical students found improvement in students’ global competence, citizenship, and health-related knowledge compared to a control group. Students also showed increased interest in global health careers and recognition of GHE’s importance (Kim et al., 2024). Likewise, in engineering, there has been a call for CBE, due to its emphasis on student-centered, outcome-driven model that promotes lifelong learners equipped for real-world application of skills (Malhotra et al. (2023).
Furthermore, self-efficacy, a key psychological construct introduced by Bandura (Bandura, 1997) refers to an individual’s belief in their ability to perform tasks and achieve goals. In educational settings, self-efficacy influences motivation, persistence, and overall academic success. Students with higher self-efficacy are more likely to engage in learning, seek challenges, and persist through difficulties, making it a crucial factor in professional education (Basileo et al., 2024; Honicke et al., 2023; Schunk & DiBenedetto, 2022; Zimmerman, 2000). Within CBE frameworks, the emphasis on mastery and repeated opportunities for skill application (Gagnon, 2023; Henri et al., 2017) can further enhance self-efficacy by providing students with tangible evidence of their capabilities.
As such, by assessing the effectiveness of a CBE model in graduate public health education on students’ self-efficacy in applying their knowledge, this study aims to contribute to the ongoing discussion on best practices in public health education. The findings may offer valuable insights for educators and educational policymakers seeking to enhance graduate-level training programs to better prepare students for the evolving demands of the public health workforce.
Methods
Study Design
This study employed a repeated measure quasi-experimental design to assess the impact of a redesigned, competency-based Master of Public Health (MPH) curriculum on student self-efficacy in professional skills over a 2-year period. The program redesign served as the intervention, and student self-efficacy was evaluated through multiple survey assessments administered at key points throughout the program.
Specifically, the program design was also implemented to ensure alignment with the accreditation standards of the Council on Education for Public Health (CEPH), which accredits public health schools and programs. Its competency framework includes foundational and cross-cutting areas such as data analysis, leadership, communication, and systems thinking. The accreditation process involves a self-study, a site visit by peer reviewers, and routine reviews to ensure continued alignment with public health workforce needs (Council on Education for Public Health, n.d.); and further guided the work presented in this study as well.
The study is organized into two overarching phases. Phase I focused on the curriculum redesign and intervention development. During Phase I.a, faculty conducted a comprehensive review and restructuring of the curriculum to align course content and learning outcomes with established public health competencies. This included identifying gaps, eliminating redundancy, and creating skill-based, applied learning experiences. In Phase I.b, several intervention components were developed and implemented, including a cohort-based course sequence, a foundational boot camp, integration of a 2-year service-learning project, and the establishment of a formal advisory board to ensure alignment with workforce needs.
Phase II involved the evaluation of the redesigned program’s impact on student self-efficacy. This was achieved through a series of structured surveys administered at four time points (pre-program, a mid-program, end-of-program, and an alumni survey).
Phase I: Curriculum Redesign and Intervention Development
Phase I.a: Curriculum Redesign
This study was part of an ongoing 2-year pilot assessment strategy designed to evaluate the effectiveness of a newly restructured MPH program, which was developed based on the CBE framework. The goal of this evaluation was to obtain first-time accreditation for the program from CEPH, while ensuring that the curriculum effectively prepared students with the skills and competencies needed to meet evolving workforce demands in the public health field.
The first step in this process involved deconstructing and categorizing each required competency, as outlined by the accreditation body, into distinct skill-based domains. These categories included areas such as data analytics, disease investigation, program planning, and other essential public health skills. Once these categories were established, courses from the previous iteration of the MPH program were mapped onto them. This was done primarily to identify gaps in the curriculum. Through this analysis, several key deficiencies were identified, including the need for additional courses focused on public health policy, health behavior, grant writing, and interprofessional skills.
Following this, an in-depth review of past syllabi from all existing courses was conducted to assess both the content covered and the extent to which it aligned with the newly established skill-based competencies. It became evident that nearly all courses required a complete redesign as they were found to be primarily structured around knowledge dissemination, often repeating content from undergraduate coursework rather than fostering skill development. For example, students in biostatistics were learning descriptive and bivariate statistics, as well as the use of z-tables (all of which are covered in undergraduate level), with assessments focused on rote memorization rather than the application of this learned knowledge to demonstrated skills in data analysis, interpretation, data-driven decision-making, or any advanced data analytic skills.
As a result, program competencies were leveraged to define key, skill-driven course-level learning outcomes, ensuring that content was intentionally designed to build applied skills rather than solely impart theoretical knowledge. This approach aligned with Bloom’s Taxonomy (Flinders & Uhrmacher, 2012) by emphasizing higher-order cognitive skills, such as analysis, evaluation, and creation, rather than focusing solely on lower-order skills like recall and comprehension (Supplemental File 1). The final curriculum, further resulted in courses, matched to program learning objectives, which were then matched with overall competencies (Supplemental File 2).
Phase I.b: Intervention Development
The original program allowed students to enroll in courses in any sequence, with each course operating independently. This often led to content overlap, contradictions, and inconsistencies in the development of knowledge and skills. Additionally, as noted earlier, several courses duplicated undergraduate material, limiting students’ exposure to new knowledge and skills. Given that admission requirements included undergraduate-level public health training, students frequently repeated content rather than acquiring new learning.
In response, the redesigned program incorporated key changes, such as cohort-based approach, boot camp, integration of service-learning throughout the entire 2-year program, and establishment of a formal advisory board. This allowed courses to build upon the content and skills developed in previous coursework. Other key changes included the implementation of a boot camp and the establishment of the first advisory board to ensure stakeholder feedback.
Cohort approach: To ensure the scaffolding of mastery throughout the curriculum, the program was restructured into a cohort-based model. Under this model, students followed a predetermined sequence of courses over the 2-year period, ensuring a logical and progressive development of competencies. During their final term, students were given the opportunity to select electives tailored to their interests. This structured approach ensured that students developed key public health skills in a stepwise manner, culminating in a high-impact inaugural symposium (Graduate Student Symposium) where they showcased the results of their 2 years of service-learning project. This event was attended by key stakeholders, including county public health leaders, the university Provost, guest speakers, and other professionals in the field, providing students with the opportunity to present their work to those actively shaping the public health workforce. Such stakeholders were recruited by active electronic communications through network listservs, community meetings, as well as through internship sites.
Boot camp: The boot camp was designed to ensure that all students began at the same level. It covered foundational undergraduate content in epidemiology, biostatistics, and human subject research. Since an undergraduate background in public health or a related discipline was a prerequisite for admission, the boot camp served as a refresher rather than a repetition of previously covered material. Access to bootcamp content was provided to all students during program orientation. Next, each class, such as graduate level epidemiology, biostatistics, and evaluation/research methods included assignment credit to allow students to receive points for completing the bootcamp by the first week of the respective course.
Service-learning: The 2-year service-learning project was established in collaboration with key campus partners to enable students to apply theoretical concepts in practice. For example, in their first term, students in the public health administration course learned the fundamentals of market versus social justice theories in public health decision-making, community needs assessment, and stakeholder engagement. As part of this process, students engaged with partners such as the student health center and the campus food pantry to conduct needs assessments. Based on these assessments and partner feedback, students developed Instagram teasers proposing health education interventions to address the most pressing needs. These teasers were evaluated by partners, and students’ grades were partially based on this feedback. This approach helped students integrate stakeholder input into program development rather than relying solely on course grading rubrics, thereby ensuring practical workforce experience.
Building on this foundation, students applied partner feedback and concepts from their health behavior course in the following term to develop full health education intervention programs. Simultaneously, in their research methods course, students learned how to design and pilot test survey questionnaires. During their epidemiology course, these interventions were implemented, allowing students to apply theories related to experimental studies, data collection procedures, and strategies for addressing attrition. At the end of the year, students analyzed pre- and post-intervention data in their biostatistics course, gaining skills in data cleaning, de-identification, data protection, and data-driven decision-making. These findings were then presented to partners, further reinforcing their practical application. The inaugural Graduate Research Symposium was established to provide students with an opportunity to present the results of their 2-year project to stakeholders.
Advisory board: To ensure the program aligned with workforce needs and strengthened interprofessional skill development, a formal advisory board was created. This board included leadership from other graduate programs, community leaders, as well as student and alumni representatives, all of whom provided valuable input to ensure the curriculum met the evolving demands of the public health field. Additionally, the board guided students through their 2-year service-learning projects, offering strategic insights to enhance workforce readiness. At a minimum, the board included five members, representing both internal and external stakeholders.
Phase II: Evaluation
Once all necessary approvals for the program curriculum were finalized, electronic surveys were developed to assess the effectiveness of the newly implemented competency-based program. The surveys were structured into four stages: a pre-program survey, a mid-program student satisfaction survey, an end-of-program exit survey, and an alumni survey. The pre-program survey was administered at the start of the 2-year program during orientation, while the mid-program survey was conducted at the end of the first year. The exit survey was distributed during the final term, and the alumni survey gathered feedback 6 months post-graduation. These assessments were also integrated into the overall graduation checklist to ensure comprehensive program evaluation. The Likert-style survey questions were developed in collaboration with external advisory board and validated by expert opinion. The questions were based on the competencies in the program (Supplemental File 3).
This study presents findings on the first cohort’s (n = 28) self-efficacy in professional development skills from pre-, mid- to end-of-program surveys. All de-identified data were imported and analyzed in SPSS version 28 (IBM Corp.). First, descriptive statistics were used to assess responses to each survey questions. Next, bivariate analyses (Fisher’s Exact test) were used to assess the difference from pre- to mid-program and mid- to post-program. A chi-square linear by linear association test was utilized to obtain p for trend, comparing pre-, mid- and end-of-program changes in self-efficacy for skills.
Ethical Approval
For the purposes of this study, Institutional Review Board (IRB) approval was obtained, and only data from participants who provided informed consent were analyzed and presented in this study. Students were given consent forms noting their right to opt from providing consent for their program data to be used for research. All other data were used exclusively for internal program assessment and accreditation compliance reports. Although data for internal assessment were collected with respondents’ names, all such responses were de-identified for this study.
Results
As available from the self-study (contact corresponding author for a copy), a majority of the cohort students were females (79%), and a higher percent self-identified as Hispanic (58.8%), followed by white (17.7%).
Table 1 provides data on students’ self-reported efficacy regarding professional skills before the start of a public health program. The results show varying levels of confidence in different skills. For instance, a majority of the students (81.4%) felt confident (reported agree or strongly agree) about describing a population health problem using the core parameters of magnitude, person, time, and place. Similarly, 77.7% of students felt proficient in using information techniques, such as databases and statistical software. When assessing students’ self-efficacy in applying the health law-making and rule-making processes at federal, state, and local levels to provide public health solutions, 14.8% reported that they did not feel confident, 66.7% were neutral, and a total of 18.5% reported they agreed or strongly agreed to feeling confident.
Student’s Self-Efficacy on Professional Skills, Pre-Program.
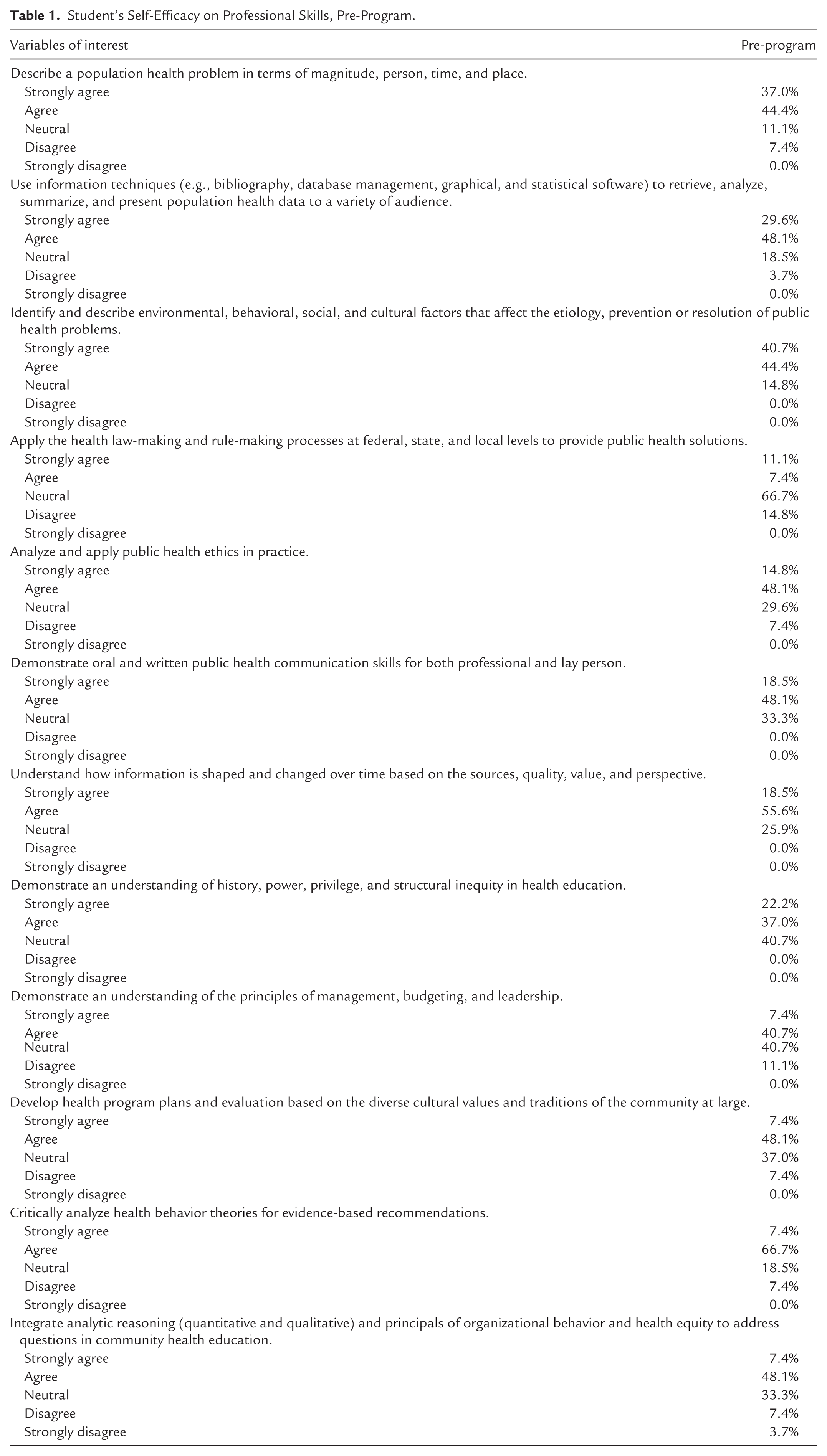
In areas such as public health communication and ethics, most students agreed or strongly agreed that they had the necessary skills (66.6% and 62.9%, respectively). This table sets the baseline for students’ initial self-assessment before further development during the program.
Table 2 compares students’ self-efficacy in various professional skills between the pre-program and mid-program stages, highlighting areas of improvement. The data indicates growth in many areas, although not all reached statistical significance. For example, the ability to analyze public health law-making processes showed statistically significant (p < .001) growth, with the percentage of students agreeing strongly increasing from 11.1% to 23.1%, and those agreeing rising to 50%. Likewise improvements were seen in the ability to demonstrate public health communication skills, with an increase from 18.5% pre-program to 69.2% mid-program.
Student’s Self-Efficacy on Professional Skills, Pre-and Mid-Program Comparison.
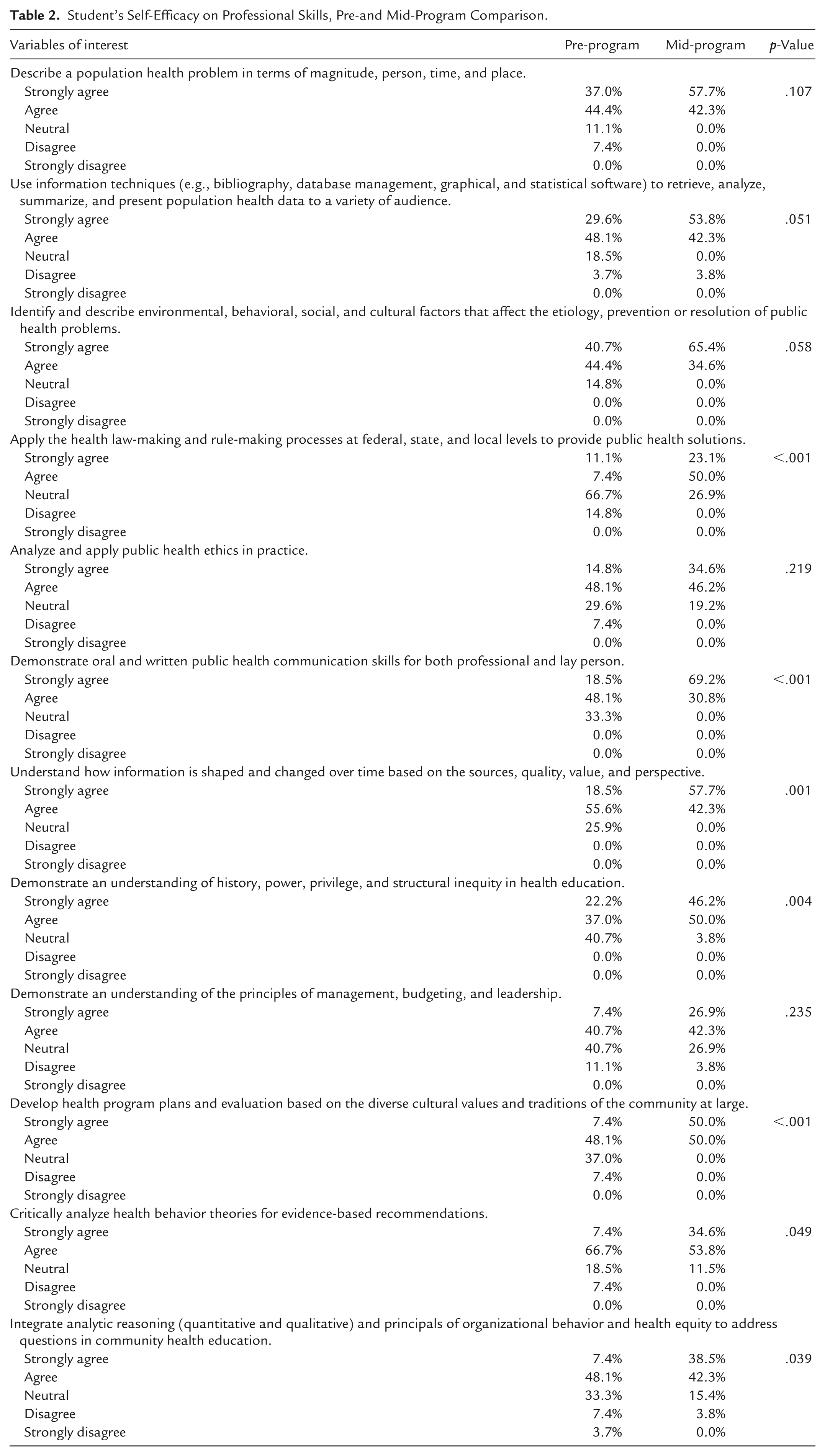
Additional gains were also seen in developing culturally responsive health program plans and evaluations (Strongly Agree rose from 7.4% to 50.0%, p < .001). Statistically significant improvements were also found in understanding how information evolves across sources (p = .001), recognizing history, power, and structural inequity in health education (p = .004), critically analyzing health behavior theories (p = .049), and integrating analytic reasoning with organizational behavior and health equity (p = .039).
Table 2, however, further shows several areas where the students did not demonstrate statistically significant changes in their self-efficacy from pre-program to mid-program. For example, in the skill of describing a population health problem in terms of magnitude, person, time, and place, the percentage of students who strongly agreed with this statement increased from 37% to 57.7%. However, there was a shift in the neutral responses from 11.1% to 0%, and the group that disagreed dropped from 7.4% to 0%. Despite these changes, the overall shift was not statistically significant. Similarly, when considering the use of information techniques (e.g., bibliography, database management, and graphical/statistical software), there was an increase in those strongly agreeing, from 29.6% to 53.8%, but also a notable shift in neutral responses (18.5%–0%), and a small decrease in those agreeing (48.1%–42.3%). Again, although this showed improvement, it did not reach statistical significance. Further, in the area of applying public health ethics in practice, students’ responses did not show statistically significant change. For instance, percentage of students who strongly agreed went from 14.8% to 34.6%, and the neutral responses decreased from 29.6% to 19.2%.
Table 3 shows further development in students’ self-efficacy as they progress through the program, from mid-program to the end of the program. Students demonstrated statistically significant growth in several professional skills from mid- to end-of-program. Specifically, their ability to describe a population health problem in terms of magnitude, person, time, and place improved from 57.7% to 88.0% for strongly agreeing (p = .009). Their capacity to use information techniques to analyze and present health data rose from 53.8% to 84.0% for strongly agreeing (p = .022). Statistically significant increases were also observed in applying the health law- and rule-making processes (23.1%–56.0%; p = .004), analyzing and applying public health ethics in practice (34.6%–76.0%; p = .015), critically analyzing health behavior theories for evidence-based recommendations (34.6%–80.0%; p = .003), and integrating analytic reasoning with organizational behavior and health equity (38.5%–80.0%; p = .014).
Student’s Self-Efficacy on Professional Skills, Mid- and End-of-Program Program Comparison.
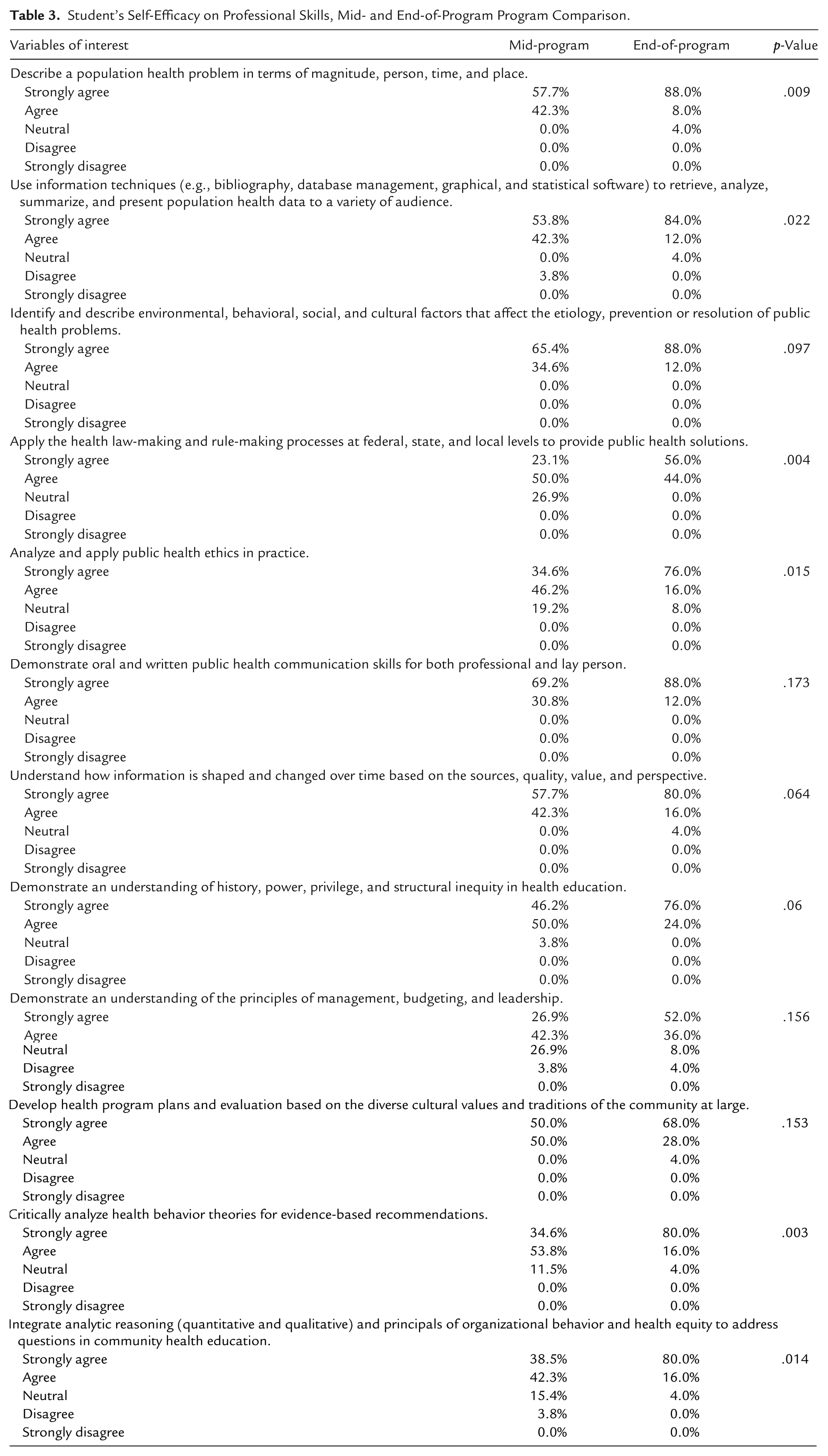
Other skills showed improvements, though they did not reach statistical significance. For example, the proportion strongly agreeing they could identify environmental and social determinants of health increased from 65.4% to 88.0%. Similarly, confidence in public health communication skills grew from 69.2% to 88.0%, and in understanding how information evolves across sources from 57.7% to 80.0%. The percentage strongly agreeing they could recognize history, power, privilege, and structural inequity rose from 46.2% to 76.0%. Gains were also seen in management, budgeting, and leadership (26.9%–52.0%) and in developing culturally responsive health program plans (50.0%–68.0%). These trends suggest consistent growth, even where statistical significance was not reached.
Next, Table 4 presents students’ self-efficacy on various professional skills across three time points: pre-program, mid-program, and end-of-program. Overall, there were statistically significant improvements in self-reported abilities across all skills, with all skills showing a p-value for trend analysis showing less than .001. For example, the ability to describe a population health problem in terms of magnitude, person, time, and place saw a substantial increase, with 37% of students strongly agreeing pre-program, compared to 88% by the end. Similarly, students’ self-efficacy in using information techniques to retrieve, analyze, and present population health data also improved, with 29.6% strongly agreeing pre-program, rising to 84% by the program’s end.
Student’s Self-Efficacy on Professional Skills, Three Time Point Comparison.
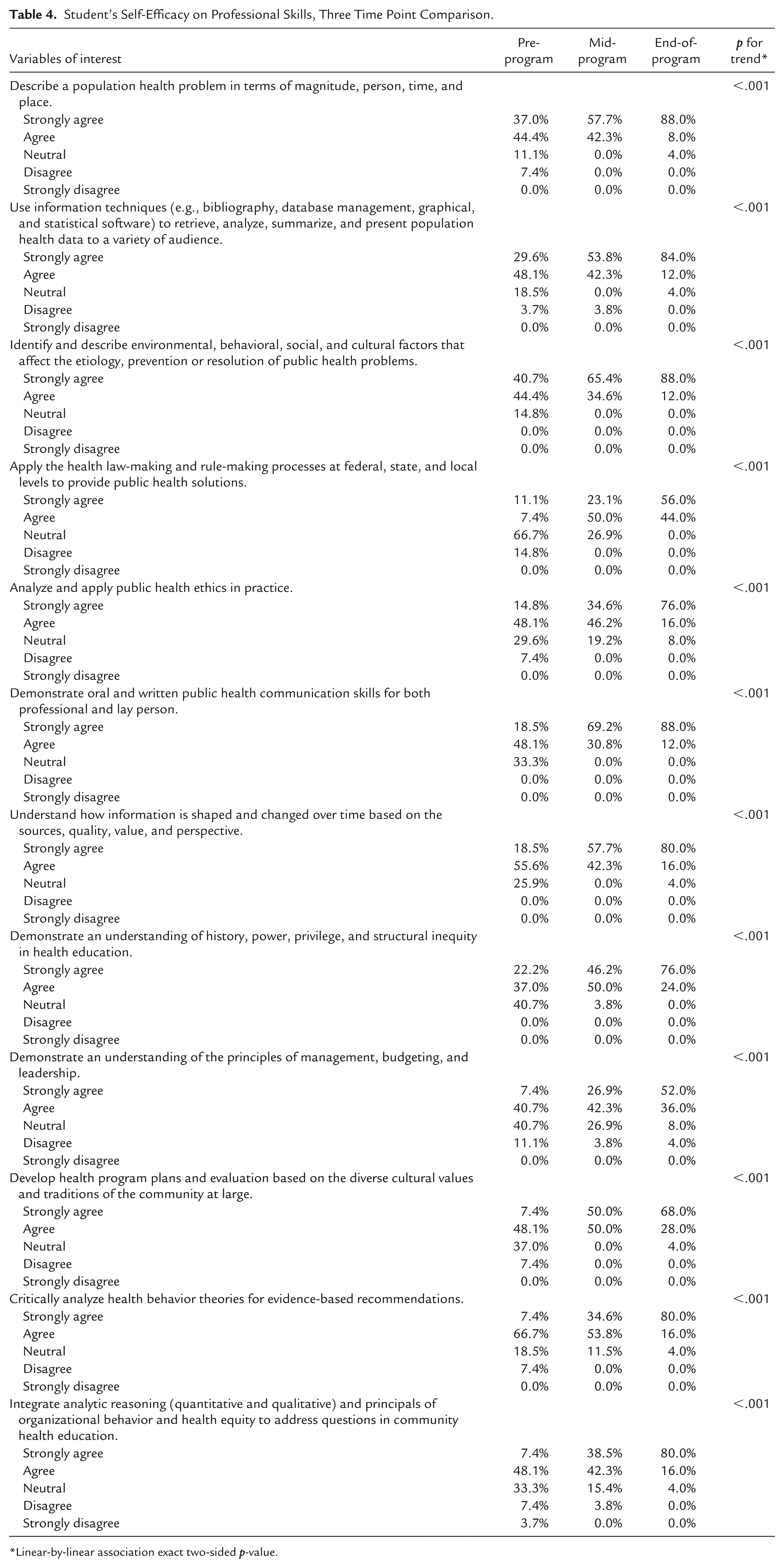
Linear-by-linear association exact two-sided p-value.
In other areas, such as identifying and describing environmental, behavioral, social, and cultural factors impacting public health, 40.7% of students strongly agreed pre-program, growing to 88% by the end. Students also reported a notable increase in their ability to apply health law-making and rule-making processes, with 11.1% strongly agreeing pre-program, compared to 56.0% at the end. A similar trend was observed in public health ethics, with 14.8% of students strongly agreeing at the start of the program and 76% strongly agreeing by the end.
Students also reported strong gains in public health communication skills, jumping from 18.5% strongly agreeing pre-program to 88% by the end. Self-efficacy in understanding how information is shaped by sources and perspectives increased with statistical significance, with 18.5% strongly agreeing at the beginning, compared to 80% by the program’s conclusion. The ability to demonstrate an understanding of history, power, privilege, and structural inequity in health education also saw substantial progress, with 22.2% strongly agreeing pre-program and 76% by the end.
Additionally, students’ confidence in understanding management, budgeting, and leadership principles grew, with 7.4% strongly agreeing pre-program and 52% at the end. Students also showed statistically significant improvement in developing health program plans based on cultural values, from 7.4% to 68%. Finally, critical analysis of health behavior theories saw a dramatic increase, with 7.4% strongly agreeing at the start and 80% by the end.
Discussion
This study aimed to evaluate the impact of a redesigned, competency-based graduate public health curriculum on students’ self-efficacy in applying relevant professional skills. Using a quasi-experimental, repeated measures design, we assessed self-efficacy at three time points: pre-program, mid-program, and end-of-program. Results demonstrated overall improvements in students’ perceived confidence across nearly all assessed domains. Notably, public health communication and data analysis skills showed early gains, while areas such as ethics, structural inequity, and health law exhibited more gradual improvements, often accelerating in the second year of the program. These trends suggest that while some competencies can be strengthened early through foundational instruction and structured opportunities for practice, others may require extended experiential learning and repeated application over time to foster meaningful development.
One key observation is that areas where students showed no significant change from pre-program to mid-program but later exhibited notable improvements by the end of the program, seem to reflect skills that require a longer time for mastery or deeper integration. For example, self-efficacy related to public health ethics showed graduate improvement, suggesting that the complexities of applying ethics in real-world public health scenarios may require more time to fully grasp and internalize. A similar pattern was noted for self-efficacy in applying health law-making processes, putatively attributed to the integration of applied learning skills in the second year. For example, students were required to write their own ethical approval guidelines for collecting data as part of their service-learning project. This task required them to ensure confidentiality or anonymity requirements, follow ethical guidelines on reporting, and apply the knowledge they gained in their first year. In their first year, students received human subjects research training and certifications, which primarily provided theoretical knowledge. However, in the second year, they had to apply this knowledge in practical, real-world scenarios. The shift from knowledge-based learning to applied learning likely contributed to the significant increase in their self-efficacy regarding public health ethics, as evidenced by the gain in self-efficacy.
This gradual growth in learning is supported by several educational theories often emphasize the importance of establishing a strong foundation of knowledge before applying it in practical settings (Wrenn & Wrenn, 2009). Bloom’s Taxonomy (Flinders & Uhrmacher, 2012), for instance, suggests that learning progresses through hierarchical steps, starting with foundational knowledge at the base. Similarly, Andragogy (Knowles, 1984), the art and science of helping adults learn, emphasizes making learning relevant, meaningful, and practical, acknowledging that adults are more goal-oriented and motivated by practical application. As such, our results highlight that while foundational knowledge can be acquired quickly, the practical application of that knowledge, especially in complex and sensitive areas such as ethics, takes more time and is often where the most significant growth occurs.
On the other hand, public health communication skills exhibited the significant growth from pre-program to mid-program, but only a modest increase from mid-program to end-of-program. This pattern suggests that while students experienced dramatic improvements early in the program, their confidence leveled off as they became proficient in the skill. The initial surge in confidence may have been driven by opportunities to practice communication skills in class-based presentations, which were a core component of their learning experience. However, by the end of the program, students’ growth in this area stabilized, as they had mastered the basic communication techniques.
This shift may reflect the challenge of achieving further growth in public health communication once students have acquired the foundational skills. The symposium, being a major public speaking event outside of academia, provided a unique opportunity for students to practice their skills in a more authentic setting. Still, additional experiences in public speaking outside the academic environment, particularly in engaging with broader, non-academic audiences, are likely necessary for further refinement. This has been shown to be effective in the literature as well. For example, McNatt noted that service-learning projects positively impacted management students’ public speaking self-efficacy, as well as played a role in reducing anxiety and improving public speaking competence and performance; especially among those who initially reported lower public speaking self-efficacy (McNatt, 2019).
An intriguing trend emerged in areas where students showed significant improvement from pre-program to end-of-program, but no significant difference between mid-program and end-of-program. For instance, the ability to describe a population health problem substantially increased from pre-program to the end, but not from pre- to mid-program; highlighting that some skills, such as describing health problems, demonstrate rapid early gains followed by more gradual improvement as students reach proficiency.
This could be attributed to the fact that foundational skills, such as, describing population health problems, were heavily emphasized in the first year of the program but were less focused on during the second year. As students progressed to more complex and applied topics in their second year, these basic skills may not be revisited as frequently, which could contribute to the observed plateau. To ensure continued growth and the integration of these foundational concepts into practical applications, more opportunities for assessment are needed. As part of larger formative summative assessment strategies (OECD Education Working Papers, 2011), integrating opportunities for students to actively apply their first-year knowledge to real-world situations throughout the program are needed. One potential strategy to maintain skill development could be incorporating more case-based learning scenarios where students must analyze and apply foundational knowledge to complex, evolving public health problems could help bridge the gap between knowledge and practical application. Literature suggests that ongoing, applied assessments throughout a program are crucial for skill retention and mastery and thus, may prevent the stagnation observed in this study (Ofstead et al., 2023).
When assessing self-efficacy related to information techniques (e.g., databases, statistical software), results showed gradual improvement from pre-program to mid-program, followed by a sharp rise by the end. This may be due to the nature of the skill, students likely need time to master technical tools, and their proficiency may increase progressively as they engage with the tools in coursework and practice. The sharp rise by the end of the program is likely due to the hands-on experience students gained during their second year, where they collected, analyzed, and cleaned their own data as part of their service-learning projects. This applied work, which involved not only analyzing data but also presenting their findings to the public (rather than just within an academic setting), could have played a significant role in boosting their confidence and proficiency. Presenting to a broader audience may have provided a more practical, real-world context for using information techniques, further enhancing their skills and solidifying their learning.
The understanding of history, power, privilege, and structural inequity in health education followed a similar trajectory. While there was a gradual increase by the end of the program, the change between the mid-program and end-of-program assessments was not statistically significant. This may indicate that students’ understanding of these social determinants deepened gradually over the course of the program, with the final phase reinforcing the concepts. However, the time required to fully internalize these complex and nuanced ideas likely contributed to the more gradual improvements, as students may have needed more continued experiential learning (Kent State University, n.d.; Kolb, 1993) opportunities to apply learned concepts to real-world scenarios.
A key factor in this process is likely the integration of service learning, which allowed students to apply theoretical knowledge to practice right away. However, in this cohort, service learning was primarily limited to campus-based partnerships, which may have restricted students’ exposure to broader community contexts. To better facilitate a deeper understanding of these issues, it is important to expand opportunities for students to engage with community partners earlier in their studies. Exposure to diverse community settings and partnerships enhances students’ understanding of how history, power, privilege, and structural inequities manifest in real-world public health challenges, thereby improving their capacity to address these issues in their future careers (The Aspen Institute, n.d.).
Limitations and Strengths
This study is not without its limitations. This study does not account for external factors, such as personal or professional experiences, that may influence skill development. Some areas, such as public health law and ethics, showed slower improvement, suggesting that mastery of these concepts may require more extended practical exposure beyond the program’s structure. Reliance on self-reported can also lead to social desirability bias. Finally, we did not compare the present results to long-term retainment as collected in the alumni survey (due to institutional limitations and lack of identifiers) to evaluate if the change in self-efficacy continued 6-months post-graduation.
Notwithstanding such limitations, there are several strengths. The study effectively tracks students’ self-reported efficacy in professional skills over time, providing clear evidence of skill development throughout the program. The inclusion of three time points (pre-program, mid-program, and end-of-program) allows for a comprehensive assessment of changes in confidence, highlighting areas of significant improvement. The data also reflect the positive impact of applied learning experiences, particularly in public health communication and using information techniques, which align with real-world applications.
Implications for Public Health Practice
Public health professionals, across the globe, are increasingly called upon to address urgent and multifaceted and cross-border problems, including pandemic preparedness, climate-related health impacts, and structural health inequities. For example, a qualitative study of public health consultants in England found that while many had begun addressing climate change, they were often uncertain about their role, felt isolated in their efforts, and experienced a variety of barriers, such as, limited resources, communication tools, expertise, and even competing priorities (van Hove et al., 2024). A similar pattern of limited resources and expertise was noted when assessing public health preparedness in responding to the COVID-19 pandemic as well (Lee et al., 2023). Further, a recent commentary reviewing the WHO-ASPHER public health competency framework through the lens of the COVID-19 pandemic identified five critical competency areas needed in times of crisis: adaptability, motivation, communication, ethics, research literacy, epidemiology, and preparedness. The authors emphasized that building public health workforce resilience requires embedding these competencies not only within public health training programs but across all levels of the healthcare system (Czabanowska & Kuhlmann, 2021).
These findings underscore the urgent need to equip and support the public health workforce to engage more fully in their responses. By emphasizing experiential and competency-based education, the program evaluated in this study contributes to this global call for a more adaptable, ethically grounded, and interdisciplinary workforce prepared to lead in future health emergencies.
Conclusion
Overall, results of this study suggest that certain public health skills, particularly those involving technical knowledge or ethical considerations, require more time for students to fully develop. Early gains may occur rapidly due to exposure to new concepts or tools, while more profound changes in application, especially in complex areas like communication, law, and ethics, often require ongoing reinforcement and real-world practice. These findings support the notion that the development of professional skills in public health is a gradual process that builds upon foundational knowledge and experiences, with greater improvement observed in later stages of a program.
Supplemental Material
sj-docx-1-php-10.1177_23733799251395184 – Supplemental material for A Quasi-Experimental Assessment of Student Self-Efficacy in Professional Skills Following a Competency-Based Graduate Program Redesign
Supplemental material, sj-docx-1-php-10.1177_23733799251395184 for A Quasi-Experimental Assessment of Student Self-Efficacy in Professional Skills Following a Competency-Based Graduate Program Redesign by Monideepa B. Becerra, Salome K. Mshigeni, Marwa Ahmad and Robert M. Avina in Pedagogy in Health Promotion
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.