
Abstract
Patients with sickle cell disease (SCD) experience multisystem complications, with sickle cell nephropathy being a major contributor to chronic kidney disease and kidney failure (KF). Despite the high burden of SCD-associated KF, little is known about how patients experience and cope with this unique multimorbidity. We conducted a dual-center qualitative study using face-to-face semistructured interviews, recruited 10 patients, and performed thematic analysis. Interviews were conducted in Arabic, transcribed verbatim, and translated into English by bilingual nephrologists. Data were coded iteratively using inductive coding. We identified 4 themes that describe patients’ lived experiences with SCD and KF: (1) adjustment to KF; (2) pain, fatigue, and crisis management; (3) knowledge, education, and awareness; and (4) fragmented care and systemic barriers. Religious faith, family support, and resilience emerged as important coping mechanisms, while patients reported feeling unprepared for dialysis and inadequately informed about modality choices. These findings highlight the need for multidisciplinary, patient-centered services, structured education on dialysis options, and improved interprofessional coordination, providing insights to inform future interventions.
Keywords
Introduction
Living with chronic multimorbidity requires ongoing psychological and social adjustment.1,2 Research on chronic illness adjustment highlights how individuals continually renegotiate identity, roles, emotional responses, and self-management behaviors in response to evolving illness burden, extending beyond the biomedical framework of disease management.2–4 In conditions associated with an unpredictable disease course, chronic pain, and functional limitation, patients often rely on complex coping strategies shaped by personal beliefs, social relationships, and cultural context.2,5
Sickle cell disease (SCD) is the most common monogenic disorder, characterized by chronic hemolysis, recurrent vaso-occlusion, and multiorgan involvement leading to multimorbidity.1,6 Sickle cell nephropathy is a major complication that can often progress to kidney failure (KF), requiring kidney replacement therapy at a young age. 7 This multidisease burden can worsen the physical and mental health of patients, negatively affecting their quality of life. 8 Understanding how patients cope with this multimorbid burden can give healthcare providers deeper insights into the challenges faced by this unique population.
Despite this, most research has focused on clinical outcomes, with little attention to the lived experiences and coping strategies of patients living with both SCD and KF.9,10 A recent systematic review of 59 qualitative studies describing the lived experiences of people with chronic kidney disease (CKD) undergoing maintenance dialysis showed that none included SCD patients and only 5 were conducted in the Middle East, 11 highlighting a critical gap in the literature. Given the importance of family ties in Middle Eastern cultures and the way faith is considered a way of life,12–14 exploring how cultural values and context shape coping and adjustment in this population is particularly important.
This study aims to address this gap by exploring the lived experiences of adults with SCD and KF and how they cope with this multimorbidity. By understanding their emotional, physical, and social challenges and coping strategies, we seek to inform patient-centered care and guide the development of tailored interventions to improve clinical care and enhance psychological support.
Methods
This was part of a dual-center qualitative study to investigate distinct but related research questions: the lived experiences of patients with SCD and KF, and the barriers to and facilitators of kidney transplantation among them. It utilized a shared cohort, but separate interview guides and thematic analyses were conducted separately for each research focus. The study was approved by the local Institutional Boards (approval number: QCH-SREC0 53/2023), and all participants provided written informed consent.
Participants and Setting
All patients with SCD and CKD with an estimated glomerular filtration rate of <15 mL/min/1.73 m2 who were receiving care at the participating centers were invited to participate in the study. We used the electronic health system to identify eligible patients and excluded patients with communication barriers preventing them from providing informed consent. All individuals identified meeting the study criteria were approached and agreed to participate in the study. Participants included patients in the pre-dialysis phase and those receiving hemodialysis or peritoneal dialysis. They were either approached during a routine clinic visit or dialysis treatment, and interviews were conducted in a private setting. Recruitment continued until thematic saturation was reached, meaning no new concepts emerged in later interviews. 15
Qualitative Interviews
We developed a semistructured interview guide that examined the psychosocial and physical impacts of living with SCD and KF, and reported our findings following the Consolidated Criteria for Reporting Qualitative Research guidelines. 16 Investigators EA (female dialysis resident) and MA (male nephrologist and medical educator) conducted semistructured face-to-face interviews. Their interest in the research topic arose from repeated clinical encounters with patients experiencing significant psychosocial burden alongside complex medical care. Both investigators completed an online course in qualitative research methodology and were trained to conduct their interviews using open-ended questioning and the interview guide. Both investigators cared for the participants as healthcare providers, each at their center, which could have facilitated rapport-building 17 but could also have influenced how participants expressed their experiences. Participants may have been inclined to moderate their healthcare criticism or emphasize certain concerns due to their existing therapeutic relationship. However, the participants were reassured that their care would not be affected by expressing any negative or positive experiences. Reflexivity discussions were held regularly within the research team to review the data collection and analysis, in examining assumptions, interpretations, and biases. Participants were informed of the study's purpose and were free to withdraw their consent at any time. The interviews lasted between 15 and 35 min and took place between February and November 2024. The interview guide was reviewed and refined after completing 3 interviews to ensure clarity and relevance. The interviews were conducted in Arabic, recorded, transcribed verbatim by HA, and then reviewed by MA. The transcripts were subsequently translated into English by HA and reviewed by MA to ensure correct transcription, accurate translation, and preservation of meaning. Both investigators were bilingual nephrologists and well-versed in the local Arabic dialect. Discrepancies were resolved through discussion and consensus, resulting in the final merged transcript. No interviews were repeated, and the transcripts were not provided to the participants for review.
Coding and Data Analysis
We conducted an inductive thematic analysis of the interview transcripts, allowing themes to emerge iteratively from the data. This flexible interpretive approach is consistent with qualitative methods used in health research to explore lived experience. 18 We employed an iterative inductive coding approach until we reached data saturation. 19 Two investigators (HA and MA) conducted the coding using the cloud-based software Tagutte. 20 Initially, both investigators independently coded the first 2 interviews to generate codes and then discussed their findings to ensure consistency in the coding process. Discrepancies were identified, and differences were reconciled through consensus. Following this, each investigator coded 3 additional interviews, bringing the total to 8. A preliminary analysis of these 8 interviews was conducted by deriving descriptive codes from the data, grouping them into categories, and organizing them into themes after identifying recurrent patterns. Codes were compared across transcripts, iteratively reviewed, merged, and refined through team discussion, and then organized into higher-order categories and overarching themes. At this stage, data saturation was felt to have been reached, as no new thematic categories have emerged from the data. 19 Two additional interviews were subsequently conducted and analyzed to confirm this assessment. These interviews did not generate new themes or modify the existing thematic structure, and recruitment was therefore concluded.
Results
Ten patients (80% male), aged between 39 and 65, met our eligibility criteria and were recruited for the study. All interviews were completed in person. Demographic characteristics of the participants are presented in Table 1. We identified 4 main themes from the analysis: (1) adjustment to kidney failure; (2) pain, fatigue, and crisis management; (3) knowledge, education, and awareness; and (4) fragmented care and systemic barriers (Figure 1). Selected illustrative quotations are provided in Table 2.
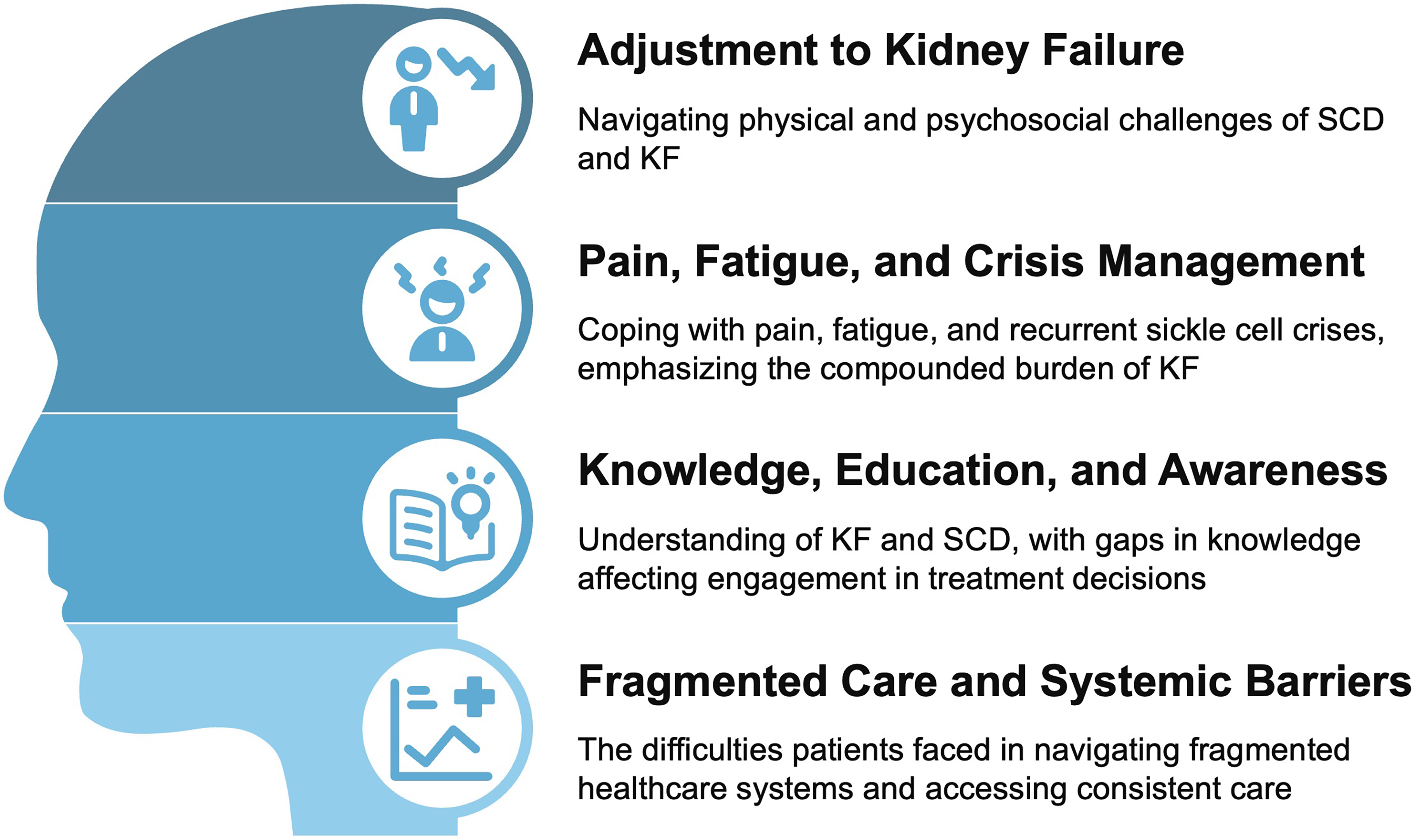
Thematic schema.
Baseline Participant Characteristics.

sickle cell disease.
Selected Illustrative Quotations for Each Theme.
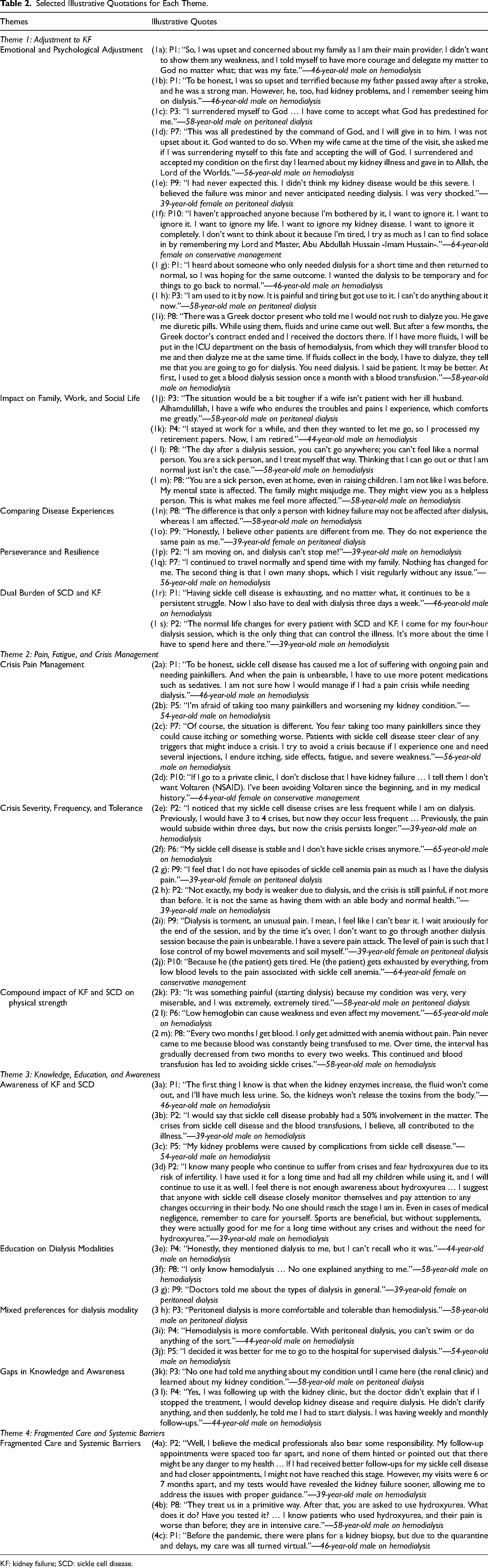
KF: kidney failure; SCD: sickle cell disease.
Theme 1: Adjustment to Kidney Failure
A strong theme emerged about how patients make sense of their KF diagnosis and navigate the physical, emotional, and social challenges and adjustments required to integrate dialysis in their lives, with a particular focus on the emotional and psychological burden.
Subtheme: Emotional and Psychological Adjustment
There was a notable focus on religion and spirituality, which served as an important source of emotional strength, supporting their capacity to endure illness-related challenges and helping them accept their diagnosis. Many were initially taken aback by the sudden realization that they needed kidney replacement therapy, expressing fear, and anger about how this diagnosis impacted their life plans. (1e) P9: “I had never expected this. I didn't think my kidney disease would be this severe. I believed the failure was minor and never anticipated needing dialysis. I was very shocked.” (39-year-old female on peritoneal dialysis) (1g) P1: “I heard about someone who only needed dialysis for a short time and then returned to normal, so I was hoping for the same outcome. I wanted the dialysis to be temporary and for things to go back to normal.” (46-year-old male on hemodialysis)
Subtheme: Impact on Family, Work, and Social Life
Participants reported that dialysis placed significant social restrictions on them. They could no longer engage in social events as they once did due to postdialysis fatigue, the dialysis schedule, and dietary limitations. The KF diagnosis also impacted their professional lives, notably limiting their options and causing some to leave the workforce at a younger age. It further affected their self-perception and how others viewed them as parents and caregivers within their families. Spousal support was essential in helping patients adapt to their illness (Table 2, Quotes 1j-m). (1l) P8: “The day after a dialysis session, you can't go anywhere; you can't feel like a normal person. You are a sick person, and I treat myself that way. Thinking that I can go out or that I am normal just isn't the case.” (58-year-old male on hemodialysis)
Subtheme: Comparing Disease Experiences
Some participants observed differences between patients with SCD and KF in contrast to those with only KF, while others felt they were similar. Pain and postdialysis fatigue were the most frequently reported (Table 2, Quotes 1n-o). P9: “Honestly, I believe other patients are different from me. They do not experience the same pain as me.” (39-year-old female on peritoneal dialysis)
Subtheme: Perseverance and Resilience
While faith served as a foundation for resilience for some patients, others drew resilience from different sources, including personal coping strategies, life experience, and social support. Many participants described efforts to live as normally as possible despite their illness. They expressed acceptance of their diagnosis and a deliberate commitment to maintaining a positive outlook, emphasizing that their condition should not disrupt their daily activities or social relationships. Several participants continued to work on nondialysis days, which they described as important for preserving a sense of normalcy and personal identity (Table 2, Quotes 1p-q). (1q) P7: “I continued to travel normally and spend time with my family. Nothing has changed for me. The second thing is that I own many shops, which I visit regularly without any issue.” (56-year-old male on hemodialysis)
Subtheme: Dual Burden of SCD and KF
The coexistence of SCD and KF presents a unique set of challenges on various levels. SCD imposes both physical and mental burdens, and when the need for dialysis is added, it becomes even more exhausting (Table 2, Quotes 1r-s). P1: “Having sickle cell disease is exhausting, and no matter what, it continues to be a persistent struggle. Now I also have to deal with dialysis three days a week.” (46-year-old male on hemodialysis)
Theme 2: Pain, Fatigue, and Crisis Management
This theme illustrates the pervasive physical burden of living with both SCD and KF and how patients coped with pain, fatigue, and recurrent sickle cell crises, emphasizing the compounded burden of KF.
Subtheme: Crisis Pain Management
The management of SCD crises has become more complex due to the presence of KF, which causes significant pain and necessitates frequent use of analgesics with more limited options. Analgesia was sometimes required at higher doses, presumably due to increased clearance from dialysis treatment and potentially due to a changing pain threshold. However, the side effect profile also became more challenging to control. Additionally, participants expressed concern that the ongoing use of analgesia could worsen kidney function at the predialysis stage (Table 2, Quotes 2a-d). (2c) P7: “Of course, the situation is different. You fear taking too many painkillers since they could cause itching or something worse. Patients with sickle cell disease steer clear of any triggers that might induce a crisis. I try to avoid a crisis because if I experience one and need several injections, I endure itching, side effects, fatigue, and severe weakness.” (56-year-old male on hemodialysis)
Subtheme: Crisis Severity, Frequency, and Tolerance
Several participants reported a decrease in the frequency of painful crises after starting dialysis; however, despite this reported reduction, some indicated that the crises became more severe (Table 2, Quotes 2e-g). (2e) P2: “I noticed that my sickle cell disease crises are less frequent while I am on dialysis. Previously, I would have 3 to 4 crises, but now they occur less frequent … Previously, the pain would subside within three days, but now the crisis persists longer.” (39-year-old male on hemodialysis) (2i) P9: “Dialysis is torment, an unusual pain. I mean, I feel like I can't bear it. I wait anxiously for the end of the session, and by the time it's over, I don't want to go through another dialysis session because the pain is unbearable. I have a severe pain attack. The level of pain is such that I lose control of my bowel movements and soil myself.” (39-year-old female on peritoneal dialysis)
Subtheme: Compound Impact of KF and SCD on Physical Strength
KF significantly impacted the participants’ stamina and physical endurance. They reported feelings of frailty and weakness due to the combined effects of their dual disease morbidity. Anemia was challenging to manage and intensified the fatigue experienced after dialysis. Some patients were resistant to treatment, necessitating frequent blood transfusions, which could potentially have limited the other adverse effects of SCD (Table 2, Quotes 2k-m). (2k) P3: “It was something painful (starting dialysis) because my condition was very, very miserable, and I was extremely, extremely tired.” (58-year-old male on peritoneal dialysis)
Theme 3: Knowledge, Education, and Awareness
This theme reflected participants’ understanding of KF and SCD, with knowledge gaps shaping how they engage with care, make decisions, and cope with kidney failure.
Subtheme: Awareness of KF and SCD
Patients reported a reasonable baseline understanding of KF symptoms and their development. Fluid retention and reduced clearance were most frequently noted as the natural progression of KF. A small subset of participants highlighted their proactive efforts in disease management through lifestyle changes and medication adherence (Table 2, Quotes 3a-d). (3a) P1: “The first thing I know is that when the kidney enzymes increase, the fluid won’t come out, and I’ll have much less urine. So, the kidneys won’t release the toxins from the body.” (46-year-old male on hemodialysis)
Subtheme: Education on Dialysis Modalities
Participants reported receiving general education about the different modalities of kidney replacement therapy. Knowledge of peritoneal dialysis was limited, and some individuals were unaware of an alternative to hemodialysis (Table 2, Quotes 3e-g). (3f) P8: “I only know hemodialysis. No one explained anything to me.” (58-year-old male on hemodialysis)
Subtheme: Mixed Preferences for Dialysis Modality
Few participants experienced both hemodialysis and peritoneal dialysis, and many were unaware of the existence of these two modalities. Some participants preferred hemodialysis over peritoneal dialysis due to the nature of directly supervised sessions and the ability to enjoy a shower or bath without worrying about the catheter (Table 2, Quotes 3h-j). (3i) P4: “Hemodialysis is more comfortable. With peritoneal dialysis, you can’t swim or do anything of the sort.” (44-year-old male on hemodialysis)
Subtheme: Gaps in Knowledge and Awareness
While some patients reported a good understanding of KF symptoms, for others, this awareness came late in their disease progression. Moreover, others did not fully understand the seriousness of their illness and the importance of following their management plan (Table 2, Quotes 3k-l). (3k) P3: “No one had told me anything about my condition until I came here (the renal clinic) and learned about my kidney condition”. (58-year-old male on peritoneal dialysis)
Theme 4: Fragmented Care and Systemic Barriers
This theme highlights that patients often experience delays and challenges in receiving coordinated care, causing fragmentation in their management plans. The COVID-19 pandemic further disrupted healthcare access, leading to longer wait times and missed routine follow-ups. Ultimately, this led to increased mistrust in the healthcare system and providers (Table 2, Quotes 4a-c). P2: “Well, I believe the medical professionals also bear some responsibility. My follow-up appointments were spaced too far apart, and none of them hinted or pointed out that there might be any danger to my health … If I had received better follow-ups for my sickle cell disease and had closer appointments, I might not have reached this stage. However, my visits were 6 or 7 months apart, and my tests would have revealed the kidney failure sooner, allowing me to address the issues with proper guidance.” (39-year-old male on hemodialysis)
Discussion
Our study highlights the profound psychological, emotional, and social burden of living with the combined diagnoses of SCD and KF. Beyond the physical aspects of their diseases, participants described their emotional distress, uncertainty about the future disruption to their identity, which affected their family and social roles, and the ongoing difficulties in integrating dialysis into their daily lives. Participants had limited knowledge of KF and its treatment options, which influenced their willingness to engage with care and their perceptions of the healthcare system, adding another layer of complexity to the management of their pain, fatigue, and SCD crises. These findings underscore how coping with SCD and KF multimorbidity is not merely biomedical but deeply embedded in emotional regulation, social relationships, and meaning-making.
The coexistence of SCD and KF led to a compounded burden, with chronic pain, fatigue, and unpredictable crises significantly reducing patients’ quality of life. Pain in SCD is multifactorial and worsened by chronic hemolysis, anemia, and systemic inflammation, 21 while CKD is associated with chronic pain with limited relief options and contributes to fatigue through anemia and chronic inflammation.22,23 The overlap of these conditions left patients struggling to manage symptoms that were persistent, unpredictable, and draining, which aligns with prior literature showing reduced quality of life in both SCD and CKD individually.24,25
Our study has shown how patients with SCD and KF used various coping mechanisms to manage the psychological toll of their multimorbidity. Many demonstrated emotional resilience, particularly after overcoming the initial denial and shock of their KF diagnosis. Religious beliefs and a sense of predestination provided comfort, fostering acceptance of their circumstances. Social interactions with family and close community members also helped patients normalize their situation and find support. Conversely, others reported maladaptive coping mechanisms, including avoidance, social withdrawal, anxiety, and frustration. These identified patterns reflect the nature of coping with chronic illness, where adaptive and maladaptive coping strategies may coexist,26,27 and emotional regulation can be developed. 2 This suggests that structured psychosocial support could help patients adopt more constructive strategies, as evidenced by participants who reflected positively on their social support.
The central role of faith in participants’ adjustment aligns with existing literature on the importance of spirituality in coping with chronic illness. 28 Faith is increasingly recognized as an important aspect of holistic patient care, with emphasis on understanding people's strengths, beliefs, relationships, and life context as individuals.29,30 In our study, participants reported that their religious beliefs provided meaning, peace, and emotional stability, helping them accept the uncertainty and hardships associated with their multimorbidity. Similar findings have been reported in prior research across diverse religious backgrounds, where spirituality plays an important role in psychological adjustment.30,31
Similarly, the importance of family and supportive social networks in buffering psychological distress and improving adaptation to chronic disease has been well-described in the literature. 32 In our study, participants described challenges related to identity and shifting family roles, with family support being central in helping cope and adapt to their chronic illness, providing reassurance and motivation to persist with dialysis. This support collectively helped shape participants’ resilience and their efforts to preserve normalcy.
Participants often described fragmented and disjointed care, which has led to mistrust and frustration in the healthcare system. This highlights well-documented issues in multimorbidity care, where poor care coordination is common, often resulting in significant gaps in care delivery, such as medication errors, redundant testing, and frequent reliance on urgent care.33–35 Managing multimorbidity by healthcare providers requires skilled coordination and a multidisciplinary approach to ensure holistic care. 36 The absence of an integrated care pathway made it difficult for patients to navigate the healthcare system, underscoring the need for structured collaboration among all relevant healthcare providers managing this complex multimorbidity.
Many of our patients expressed surprise at their diagnosis of KF and the imminent need for kidney replacement therapy. While some recalled receiving education about their condition, others reported a lack of information, contributing to initial resistance to dialysis. Unplanned dialysis start is a well-documented issue in KF, 37 often leading to the use of suboptimal vascular access and worse clinical outcomes. 38 Additionally, it can limit patients’ autonomy in choosing a dialysis modality and is associated with lower quality of life. 39 Our findings suggest that this lack of preparedness could have added to KF's psychological burden. Structured and early dialysis education, provided through predialysis clinics, is suggested as a promising solution to assist patients in the decision-making process and improve their clinical outcomes.40,41
Fatigue, pain management, and crisis tolerance have emerged as central concerns for participants, limiting their daily activities and adding a sense of dependence. Anemia associated with KF is more pronounced in patients with SCD with resistance to erythropoietin-stimulating agents (ESA),42,43 a challenge echoed by the participants, with some reporting frequent blood transfusions. The interplay of chronic hemolysis, systemic inflammation, cumulative frailty, and ongoing pain likely exacerbates this increased burden. While our study was not designed to quantify transfusion needs or ESA response, the accounts illustrate how the biological overlap of both conditions intensifies the lived burden of fatigue and pain.
Limitations
Our study had several limitations. First, even though this was a dual-center study, the sample size was small, reflecting the rarity of the dual diagnosis of SCD and KF; however, thematic saturation was achieved, and the findings provide novel insights into this unique population. Second, most of our patients were male (80%) from a single cultural background, which may limit the generalizability of our findings. Third, our study predominantly included patients receiving in-center hemodialysis, and the challenges faced by those receiving peritoneal dialysis may not have been adequately addressed. Fourth, while transcripts were audio-recorded, transcribed, and cross-validated by 2 investigators to ensure accuracy, we did not perform participant transcript review, which may have restricted respondent validation. Fifth, given that the interviewers were also clinicians involved in participants’ care, the potential for interviewer bias exists, although this was mitigated through interviewer training, adherence to a semistructured guide, and team-based coding with consensus building. Sixth, interviews were conducted in Arabic and translated into English; although bilingual nephrologists reviewed the translations, some cultural nuances may have been lost. Finally, due to the nature of being a cross-sectional qualitative study, there is a potential for recall bias, which may have influenced patients’ recollections of their healthcare experiences. Despite these limitations, our study provides rich, in-depth accounts of an underexplored patient population and offers insights to inform future care models, and can guide more empathetic and responsive care.
Practice Implications
Our findings have important implications for psychosocial support, patient education, clinical communication, and clinical practice. Integrating routine psychosocial assessment and access to counseling services may help alleviate the emotional distress, uncertainty, and identity disruption described by participants, particularly through earlier detection and management of these challenges.44,45 Educational strategies should emphasize the earlier introduction of KF concepts and kidney replacement options, alongside explicit support for coping with uncertainty, treatment-related fear, and role changes.
Addressing the complex needs of patients living with SCD and KF requires multidisciplinary, patient-centered care. Clinical communications should acknowledge the emotional and social dimensions of illness rather than focusing solely on biomedical management. Patients may also benefit from following up within multidisciplinary services led by nephrologists and hematologists, with integrated access to psychological support. Similar care models have shown success, including integrated clinics for diabetes-related kidney disease, where diabetologists collaborate with nephrologists 46 ; multidisciplinary CKD clinics 47 ; and structured transition programs for young patients moving to adult care. 48 Adapting such care models for SCD and KF could enhance patient-centered care and improve clinical outcomes.
Patient empowerment and self-management support are additional areas for intervention. Patients with SCD already navigate a chronic, debilitating illness that requires the development of self-management behaviors over time. However, the onset of kidney disease introduces new demands that can disrupt these established routines. Recognizing the emergence of multimorbidity with KF and its significant impact on their lives requires healthcare providers to support their patients in improving self-regulation and self-care practices to address this new multimorbidity. Many of our patients expressed frustration about how KF affected their ability to fulfill familial and social roles, underscoring the need for structured interventions that empower them to manage their condition more effectively.
Conclusion
Patients with SCD and CKD face a multiphysical and psychosocial disease burden. Our study expands understanding of coping in chronic illness and underscores the need for a comprehensive approach to managing these patients, emphasizing tailored healthcare interventions, improved patient education, and strengthened clinical communication and relationships among providers and between providers and patients. Patients coping with this unique combination of multimorbidity face an increased disease burden that hinders their self-regulation, necessitating a new path of disease acceptance and adjustment, compounded by pain, fatigue, and social repercussions. This is further complicated by fragmented healthcare and insufficient education and guidance. Future studies and clinical practice should focus on evaluating the prevalence of the identified themes and on interventions that address these challenges and alleviate their emotional and physical toll.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735261439469 - Supplemental material for Lived Experiences of Patients With Sickle Cell Disease and Kidney Failure: Insights From a Qualitative Study
Supplemental material, sj-docx-1-jpx-10.1177_23743735261439469 for Lived Experiences of Patients With Sickle Cell Disease and Kidney Failure: Insights From a Qualitative Study by Husam Alzayer, Eman Alabbad, Basil Alnasrallah, Abduallah Alqawain and Manaf Aljishi in Journal of Patient Experience
Footnotes
Abbreviations
Authors’ Contributions
HA and MA completed the research protocol. HA, EA, and AA designed and updated the interview guide. EA and MA conducted the interviews. AA, HA, and MA transcribed and translated the interviews. BA, HA, and MA analyzed the data and wrote the final manuscript. All authors participated in the design of the study, and read and approved the final manuscript for submission and publication.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Considerations
The study was approved by the Qatif Central Hospital's ethical committee (QCH-SREC0 53/2023), and the Saudi German Hospital extended its approval for recruiting patients at its center.
Informed Consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Statement of Human and Animal Rights
The study was conducted in accordance with the Declaration of Helsinki guidelines and written informed consent was obtained from all participants.
Supplemental Material
Supplemental material for this article is available online.