
Abstract
Language access significantly affects patient-provider communication, patient safety, and healthcare outcomes. Eliminating language barriers improves care quality. As a result, the use of professional interpreters or language concordant care is recommended. Yet, persistent barriers remain. We conducted a policy-oriented narrative review of peer-reviewed studies, federal regulations and professional guidelines published between 2004 and 2025 on language access, interpreter services, and U.S. Health System reform. We found there is a solid foundation in place to support several needed steps to strengthen language supports for non-English-preferring patients in the United States. We recommend practical, evidence-based strategies for healthcare organizations, state and federal polices, and joint multi-stakeholder initiatives. To drive meaningful change, both federal and state initiatives that financially incentivize improved language supports are needed, alongside enhanced regulatory and enforcement mechanisms to penalize underperforming providers. Healthcare systems must prioritize professional interpretation, develop systematic methods to assess and utilize the language skills of bilingual providers, and ensure consistent availability of professional high-quality language services. Integrating language access and supports into technology standards is also crucial for effectively mitigating language barriers. Substantial changes are necessary to enhance healthcare experiences and outcomes for patients who communicate in languages other than English.
Introduction
Over 68 million Americans speak a language other than English at home, with Spanish-preferring individuals comprising 62% of this population. 1 The Hispanic population, representing the majority of Spanish-preferring Americans, is the largest and fastest-growing group in the United States, with projections of 111 million by 2060. 2 Many patients with limited English proficiency (LEP)—a legal and regulatory classification used to identify individuals who have limited ability to communicate in English in a given setting—experience communication challenges that contribute to disparities in care quality, patient safety, and health outcomes.
This paper presents a policy-oriented narrative review of peer-reviewed studies, federal regulations, and professional guidelines published between 2004 and 2025 focused on language access, interpreter services, and health system reform in the United States. It synthesizes evidence-based strategies to improve patient experience through professional medical interpretation and language-concordant care, providing actionable recommendations for healthcare organizations and policymakers committed to advancing health equity.
The Patient Impact: Why Language Matters
Language barriers—including LEP, dialects, accents, and cultural expressions—create substantial challenges for patients that extend far beyond simple miscommunication.3,4 Patients without language concordant-providers or professional interpreters report difficulty understanding medical instructions, 5 impeded shared decision-making, 6 longer wait times, lack of care continuity, reduced understanding of diagnoses and treatment options, 7 and increased risk of medical errors 8 regardless of patient health literacy. Research also demonstrates language barriers are associated with increased medical complexity, 8 higher rates of multimorbidity, 9 worse chronic disease control, longer hospital stays, and higher risk of inpatient adverse events. 10
Professional medical interpreters are individuals demonstrating proficiency in both languages who complete formal training and adhere to confidentiality standards. 11 Professional interpreters significantly improve patient understanding and experiences compared to using informal interpreters such as family members or staff. They facilitate accurate communication, maintain patient confidentiality, and serve as cultural liaisons. 12 Access to effective communication through professional interpretation significantly enhances patient understanding, adherence to treatment plans, and care experiences 13 and is consistently associated with reduced medical errors and improved patient safety.12,14
Actionable Insights: Evidence and Barriers to Implementation
Language-Concordant Care
Language-concordant care—care delivered by a provider in the patient's preferred language—substantially enhances patient experience and clinical outcomes. Patients receiving language-concordant care report greater trust in their provider, improved comprehension of medical information, more comprehensive health discussions, stronger therapeutic relationships, and increased comfort disclosing sensitive health and social information. Spanish-preferring patients receiving language-concordant care appreciate comprehensive discussions of health concerns and report greater trust in their providers, though some feel rushed during visits. 15 Direct communication in the patient's language leads to improved patient experience, improved care quality, and reduced risk of adverse events.12,16
Randomized and observational studies demonstrate that language-concordant care for non-English-preferring patients improves chronic disease management and shortens hospital stays. 12 Patients with language-concordant providers experience improved glycemic control and medication adherence. 17 Importantly, frail hospitalized patients with language-concordant care experience fewer adverse events and lower in-hospital mortality. 18 These findings highlight that language-concordant care is not only a communication strategy, but also a measurable determinant of clinical quality and safety.
However, language-concordant care effectiveness critically depends on provider language proficiency, which is rarely formally assessed in clinical practice. 16 Clinicians who use limited language skills instead of professional interpreters increase risk of miscommunication, poor health outcomes and possible adverse events. 19 Despite strong evidence that language-concordant care is most effective at reducing medical complexity and improving outcomes in non-English-preferring patients, insufficient financial and institutional incentives exist to expand recruitment, training, evaluation, or retention of language-concordant providers and staff.20,21
Professional Interpretation
Professional interpreters bridge critical communication gaps when language-concordant care is unavailable—which remains the reality in most healthcare settings. Benefits of professional interpretation include improved patient understanding and treatment adherence, reduced medical errors, enhanced patient experience compared to informal interpretation, cultural brokering supporting shared decision-making, and maintained confidentiality and patient privacy.12,13 Professional interpreters can be utilized in-person, by video, or by telephone, offering flexibility and accessibility in how language services are accessed across healthcare settings.
Patient perspectives reveal that while professional interpretation improves understanding of medical information, 15 some patients describe communication through interpreters as less personal or more transactional than direct communication with providers. 15 Many patients maintain strong relationships with established English-speaking providers despite language barriers due to continuity and established rapport, 15 suggesting that provider relationships are heavily weighted in patient experience and healthcare decisions.
Professional interpreters themselves identify factors affecting interpretation complexity and patient experience, including clinical topics, patient characteristics, family presence, and provider language proficiency. 22 They often act as advocates—helping patients remain calm, clarifying clinical explanations, and ensuring essential details are conveyed accurately. This advocacy role highlights how professional interpreters contribute to patient experience beyond simple translation. Interpreters also emphasize that patient experience improves substantially with provider training on effective interpreter use, including proper placement of video devices and allowing adequate time for consecutive interpretation. Consistent institutional support, including clear procedures for interpreter breaks and call transfers, and periodic reassessment of policies further enhance interpretation quality and patient experience.22
Current Barriers to Language Access
Table 1 outlines common barriers to language access and support.
Barriers & Solutions to Language Access and Support in Healthcare Settings.
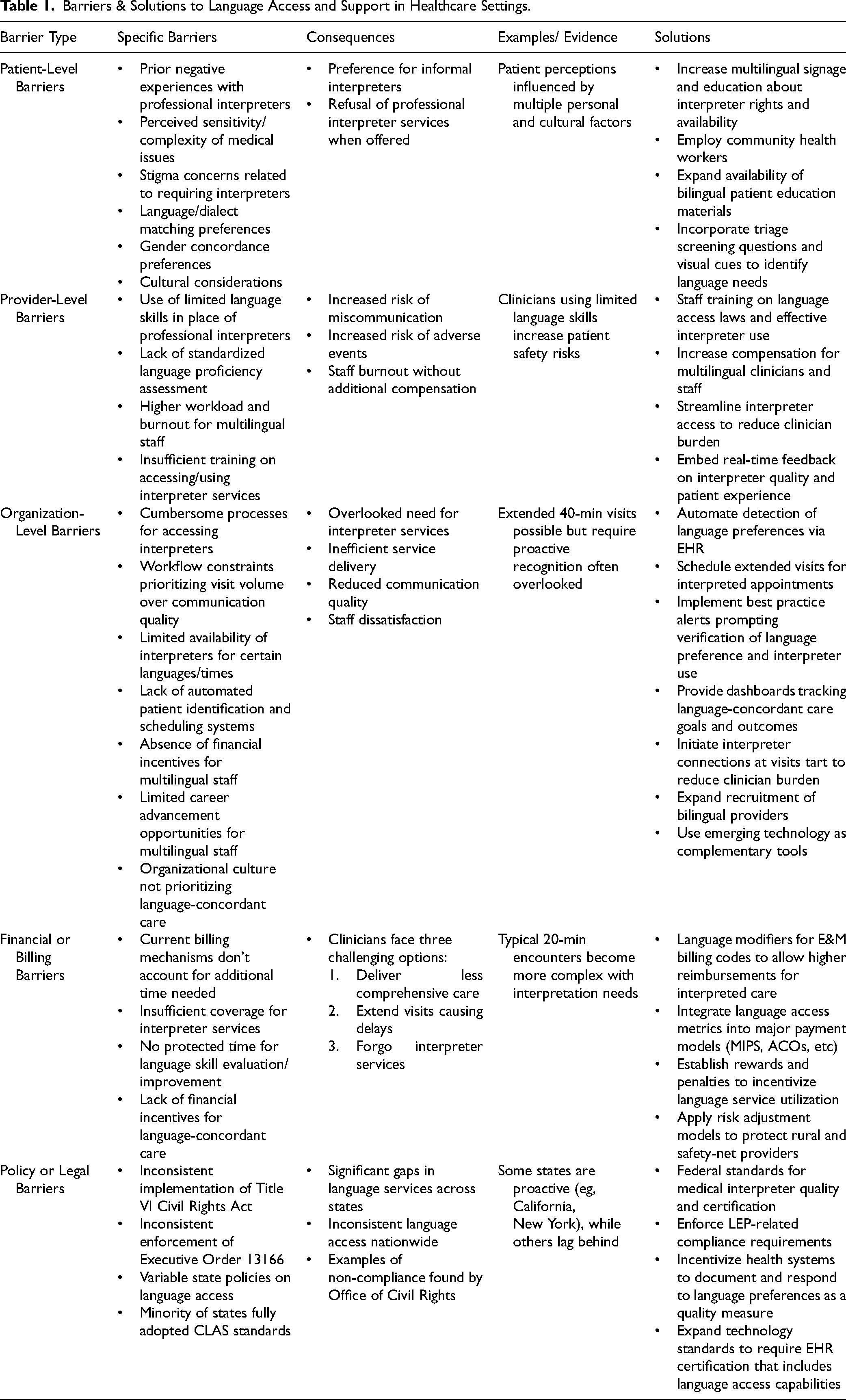
Patient-Level Barriers
Prior negative experiences with interpreters, concerns about privacy and stigma related to requiring interpretation services, cultural preferences for informal interpreters, and desire for gender- or culturally-matched providers all influence whether patients accept professional interpretation.23–25 These factors collectively create barriers to professional interpreter utilization. Many patients express preference for informal interpreters and forgo professional services despite evidence of superior outcomes. 15 System-wide informational campaigns, policy changes, site-specific outreach, and leadership champions can reduce use of informal interpreters and reinforce the importance of professional interpretation. 26 However, financial and institutional incentives are needed to standardize these outreach and education strategies nationwide.
Provider and Organizational Barriers
Cumbersome and inefficient processes for accessing interpreters, 27 insufficient clinician and staff training on how to access and effectively use interpreters, 28 workflow constraints that prioritize visit volume over communication quality, 27 and limited availability of interpreters for certain languages or at specific times 28 contribute to inconsistent interpretation service delivery. Many healthcare settings lack automated systems to identify language preferences and schedule appropriate interpreter services. Clinicians and staff using limited language skills instead of professional interpreters increase risk of miscommunication and adverse events, 19 yet face few barriers preventing this unsafe practice. Additionally, multilingual providers and staff may experience higher workload and burnout,20,29 resulting from frequent requests for assistance with interpretation, often without additional compensation or organizational support.
Financial Barriers
Current billing mechanisms inadequately account for the additional time required for effective interpreter-facilitated communication. A typical clinical encounter lasting 20 min becomes substantially longer when interpretation is required, forcing clinicians to choose between delivering less comprehensive care within standard timeframes, extending visits and causing delays for subsequent patients, or forgoing interpreter services entirely. The reimbursement code for interpretation (CPT code T-1013) often proves inadequate given actual time requirements. Some clinical settings allow extended 40-min visits for patients needing interpreters, but identifying these patients and adjusting appointment times is not automated and requires proactive recognition by clinicians and staff. Health systems often do not provide financial incentives or protected time for language skill evaluation and improvement.29,30
Policy and Enforcement Barriers
While language preference drives quality improvement, LEP remains the legal and regulatory framework governing language access obligations. Yet, implementation and enforcement of legal frameworks like Title VI of the Civil Rights Act and/or Executive Order 13166 remain inconsistent,31,32 creating significant service gaps across different states and healthcare settings. State policies on language access vary widely.33,34 California implemented progressive language access laws, including threshold policies mandating language assistance for Medicaid enrollees whose primary language is not English once population size reaches designated levels.33,34 This policy increased mental health service use among non-English speaking populations. New York implemented comprehensive approaches including translated prescription labels 35 and community health worker programs, improving language and cultural-concordance.36,37 However, a minority of states fully adopted National CLAS Standards (Culturally and Linguistically Appropriate Services in Healthcare),38,39 contributing to inconsistent language access across the US.
Practical Recommendations
Improving language access requires coordinated action across technology, workforce, and policy domains. This section summarizes practical strategies that healthcare organizations and federal policymakers can implement to embed language access into routine care delivery. Digital tools—including electronic health records (EHR), telehealth platforms, and other integrated communication technologies—can serve as unifying mechanisms to connect these efforts and standardize language access practices.
Digital Tools and EHR Integration
Optimized EHR integration can: 1) automate detection of language preferences during patient registration or visit rooming, 2) schedule extended visits for interpreted appointments, 3) create best practice alerts prompting clinician verification of language preference and interpreter use, 4) provide dashboards tracking language-concordant care goals and outcomes, and 5) reduce clinician burden in connecting with interpreters by initiating connections at visit start. 40
Beyond EHR optimization, staff education is essential to ensure providers and support teams understand language access laws and best practices for using and engaging with professional interpreters. Embedding real-time feedback on interpreter quality and patient experience, streamlining interpreter access, and incorporating triage screening questions and visual cues into workflows can further increase interpreter utilization. 40 Complementary strategies include expanding recruitment of bilingual providers, offering training on effective interpreter use, tracking provider ratings of interpreter quality and cultural competency, and increasing the availability and dissemination of bilingual patient materials. 40
Finally, while emerging technologies such as machine translation and generative AI can enhance accessibility and efficiency, they should serve only as complementary tools—not replacements—for professional interpreters, particularly in high-risk, complex, or vulnerable clinical settings where accuracy, confidentiality, and cultural nuance are critical.
Recommendations for Healthcare Organizations
Healthcare organizations should increase multilingual signage and patient education about interpreter availability and patient rights, 26 adapt EHR tools for improved language access, 40 provide comprehensive staff training on language access laws and effective interpreter use, 16 increase compensation for multilingual clinicians and staff,30,41 provide extended appointment times for patients requiring interpretation, and employ community health workers who reflect community cultural and linguistic characteristics.42,43
Recommendations for Federal Policy
Federal agencies should establish standards for medical interpreter quality and certification, ensuring consistent high-quality interpretation regardless of healthcare setting, state, or language. 44 Policies should continue to enforce LEP-related compliance requirements, while also incentivizing health systems to document and respond to patients’ language preferences as a quality measure. Federal policymakers should incorporate language modifiers into Evaluation and Management billing codes, allowing higher reimbursements reflecting extended appointment times required for interpreted care. Language access metrics need to be integrated into major payment models (eg, Merit-based Incentive Payment System (MIPS), Accountable Care Organization (ACO) models), so that it is possible to establish rewards for facilities implementing strong language services and penalties for non-compliance. To ensure equitable implementation, financial incentives and sanctions should be accompanied by risk-adjustment models that account for clinic resource constraints, patient complexity, and geographic variation—particularly to protect rural and safety-net providers serving high-need populations. Also, technology standards need to be expanded to require EHR certification that includes language access capabilities.
Why This Matters Now
In 2025, the Center for Medicare and Medicaid Innovation released “Strategy to Make America Healthy Again” 45 identifying the following three pillars for improving healthcare quality while reducing costs: promoting evidence-based prevention, empowering people to achieve their health goals, and driving choice and competition. Language access directly supports all three pillars. Language-concordance enhances lifestyle counseling on diet and exercise, improves communication, and fosters shared decision-making critical for primary prevention. 22 Language access interventions boost medication adherence, increase patient engagement, and improve uptake of recommended screenings.17,46 Access reduces misunderstandings and medical errors, improving treatment adherence, decreasing complications, and improving disease control. 12 One hospital study found that convenient interpreter access reduced 30-day readmissions and generated estimated cost savings after accounting for interpretation costs. 47 Per-patient interpretation costs remain modest compared to overall care costs. 48 Furthermore, national initiatives including EHR adoption through the HITECH Act, 49 Patient-Centered Medical Home models established in 2011, 50 and rapid telehealth expansion during COVID-19 51 created needed infrastructure and provided a solid foundation for scaling language access improvements nationally.
Limitations
Although this review primarily focuses on Spanish-speaking populations to align with the largest group of patients with limited English proficiency in the United States, discussion of other language groups remains an important area for future research and policy change. Additionally, future research should examine how these challenges intersect with other social and structural determinants—such as age, immigration status, disability, and socioeconomic context—to more fully understand and address compound vulnerabilities in healthcare communication.
Conclusion
Language barriers significantly compromise healthcare quality and patient experience for 68 million Americans preferring languages other than English. Evidence demonstrates that professional interpreters and language-concordant care substantially improve patient understanding, experience, and safety.13,16,52 Yet, persistent barriers prevent consistent access to evidence-based language services across healthcare settings and geographic regions. Meaningful change requires coordinated multi-stakeholder action: healthcare organizations must prioritize professional interpretation and develop systematic methods for assessing and utilizing qualified bilingual providers 22 ; federal policy must establish interpreter quality standards and create financial incentives for language-concordant care; and multi-stakeholder efforts must improve measurement and enforcement while strengthening support for professional interpretation. Importantly, distinguishing between LEP (a legal and safety imperative) and language preference (a quality and experience imperative) is essential for designing effective policy and practice interventions. Overall, achieving meaningful progress will require substantial systemic changes to enhance healthcare experiences and outcomes for patients communicating in languages other than English, vital for improving our nation's health outcomes and advancing health equity.
Footnotes
Consent to Participate
No subjects were asked to participate in this work.
Consent for Publication
No subjects were asked to consent publication for this work.
CRediT Statement
Conceptualization: DDQ
Methodology: DDQ, GP, ZP
Investigation: DDQ, GP, ZP
Writing—original draft: GP, ZP
Writing—review and editing: DDQ, GP, ZP, DS, NQ
Project administration: DS, NQ
Data Availability
Data sharing is not applicable for this article.
Declaration of Conflicting Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations
Ethical and human subjects protection committee approval was not necessary for this work.
Funding
This study was funded by a cooperative agreement from the Agency for Healthcare and Research Quality (AHRQ)[Contract number U18HS029321].
Informed Consent Statement
No subjects were included in this work so there was no informed consent.