
Abstract
Background/Objectives
Infection-associated chronic illnesses are associated with substantial functional impairment that limits participation in traditional in-person research. A fully remote, multicomponent intervention that combines ketogenic metabolic therapy (KMT) with behavioral interventions targets several proposed biological mechanisms underlying these conditions. This study aimed to characterize patient-reported experiences with a fully remote intervention that integrated KMT and thiamine supplementation with behavioral strategies, including circadian entrainment and mindfulness-based resilience coaching.
Methods
In this cross-sectional study, quantitative data were collected via online REDCap surveys. Feasibility and acceptability benchmarks included perceived treatment suitability, relevance, safety, and reported treatment adherence. Optimization items evaluated preferred program duration, dosing, and structure, as well as components that respondents identified as most important for future refinement.
Results
Among an international sample (n=41), all feasibility and acceptability benchmarks were met: 96% reported the intervention was helpful, 96% recommended it, and 75% felt “a lot better” after completion. Respondents provided patient-centered perspectives to optimize the intervention.
Conclusions
Incorporating patient perspectives is essential for guiding the development of safe, acceptable, and effective treatment strategies for infection-associated chronic illness, including Long COVID. Strong indicators of feasibility, acceptability, and perceived benefits support the rationale for larger controlled trials to investigate clinical efficacy and the underlying mechanistic pathways of multicomponent metabolic interventions.
Keywords
Introduction
Infection-associated chronic illnesses (IACIs), including post-viral myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), post-infectious dysautonomia, and Long COVID, affect hundreds of millions of individuals worldwide, and are associated with substantial functional impairment that limits participation in traditional in-person research. Long COVID alone accounts for more than 409 million of these cases, 1 yet there are currently no FDA-approved treatments for this broad category of conditions, and recovery rates remain low. 2 Lived experiences with interventions that are accessible, alleviate symptoms, or improve quality of life represent a critical, yet underutilized, source of evidence. Capturing these patient perspectives is essential for guiding the development of safe, acceptable, and feasible treatment strategies. 3
Ketogenic metabolic therapy (KMT) is a dietary approach that emphasizes low carbohydrate, moderate protein, and high fat intake to shift the host metabolic state from glycolysis to hepatic ketone production, primarily β-hydroxybutyrate. KMT has been shown to modify several candidate mechanisms underlying the development and persistence of IACIs, 4 including increasing mitochondrial energy production, 5 downregulating pro-inflammatory cytokines, 6 providing neuroprotective benefits to support brain health 7 and enhancing immune function. 8 KMT has also shown promise in acute SARS-CoV-2 infections. 9 However, it remains understudied in IACI populations.
Given that many individuals are already pursuing KMT through community programs, understanding patient experiences is essential, not to establish efficacy, but to explore feasibility, acceptability, perceived benefits, and highlight challenges to guide hypothesis generation and inform controlled trial design. To address the functional limitations and mobility barriers common in these populations, this cross-sectional study characterized patient-reported experiences with a fully remote, home-based program integrating KMT and thiamine supplementation with behavioral strategies, including circadian entrainment and mindfulness-based resilience coaching (KMT-LS). Study aims were to 1 : characterize diagnoses that led individuals to enroll in the 12-week program 2 ; assess participant-reported acceptability and feasibility; and 3 identify the modifications necessary to optimize program dosing, duration, and safety protocols.
Methods
Study Design
This cross-sectional study analyzed data from online surveys administered via Using the Research Electronic Data Capture (REDCap) platform. 10 Recruitment emails with survey links were sent to 194 adults who completed the 12-week KMT-LS program between June 2022 and June 2024. Respondents provided electronic informed consent and received a $50 gift card. Partially completed surveys were excluded. The response rate was calculated as the number of completed surveys divided by total emails sent. This study was approved by the **’s Institutional Review Board and all respondents provided informed consent.
Ketogenic Metabolic Therapy and Lifestyle Intervention
Enable Your Healing is a community-based educational program designed for individuals with post-viral dysautonomia, ME/CFS, and Long COVID that combined modified KMT and lifestyle strategies. This virtually delivered telehealth program aimed to educate respondents to consume a specialized form of a ketogenic diet comprised of low-carbohydrate, moderate-protein, and high-fat foods to change their metabolic state from a carbohydrate-dependent glycolytic state to a fat-dependent ketogenic state. Participants were asked to follow a personalized intermittent eating schedule, refrain from consuming foods with any added sugar, and take a synthetic, fat-soluble, S-acyl derivative of thiamine (vitamin B1 Benfotiamine, Life Extension, Fort Lauderdale, Florida), starting with 250 mg/day and titrating up, as tolerated, to 2000 mg/day. Recommended electrolyte support included daily intake of magnesium citrate/malate (3000 mg), potassium citrate (3000 mg), sodium bicarbonate (1200 mg), sodium chloride (1000 mg), with no specific protocol regarding the method of titration for these electrolyte increases.
Circadian entrainment included consistent wake times (7:00 am), immediate morning light exposure, consistent mealtimes, and limiting blue light two hours before sleep. Mindfulness-based practices included mindful eating, 60 minutes of daily meditation, and gratitude exercises. Participants were coached in mindful non-reactivity to reduce cognitive reactivity and enhance emotional regulation. These practices were intended to improve parasympathetic tone and psychological resilience rather than directly treat the underlying disease pathology. If clinically appropriate, gentle recumbent bike riding and hormetic therapies (e.g., cold therapy, heat exposure) were invited.
Delivery of the program was facilitated by a medical nutritionist and health coaches. One weekly online session was led by a medical nutritionist and focused on KMT, nutritional education, and vitamin and electrolyte supplementation. A second weekly session, facilitated by a health coach, emphasized circadian rhythm entrainment and the establishment of consistent daily routines. The third weekly session, also led by a health coach, centered on mindfulness-based practices, mindset, and psychological resilience. Each session lasted at least 60 minutes. Participants were advised to maintain the nutritional and lifestyle strategies for 12-24 months, or until remission of symptoms was achieved.
Data Collection
Acceptability, Feasibility, and Perceived Value of Program Components in the Telehealth-Based KMT-LS Intervention

Notes. Mdn=Median; IQR=Interquartile range; Treatment suitability= all items scored on 1-5 scale, whereas higher scores reflect greater suitability and satisfaction.
Perceived Value of Each Component of the Program= Participants were asked to rate the importance of each program component; 4=Very Important; 3=Moderately Important;2=Slightly Important;1=Unimportant.
Data Analyses
All statistical analyses were performed using IBM SPSS Version 29.0 (Armonk, New York, United States). Descriptive variables were calculated [mean (M), standard deviation (SD), median (Mdn), mode, and interquartile range [IQR]) and inspected for accuracy of input, out-of-range values and outliers, and non-normal variables.
Results
Participant Characteristics
Participant Demographics (n = 41)
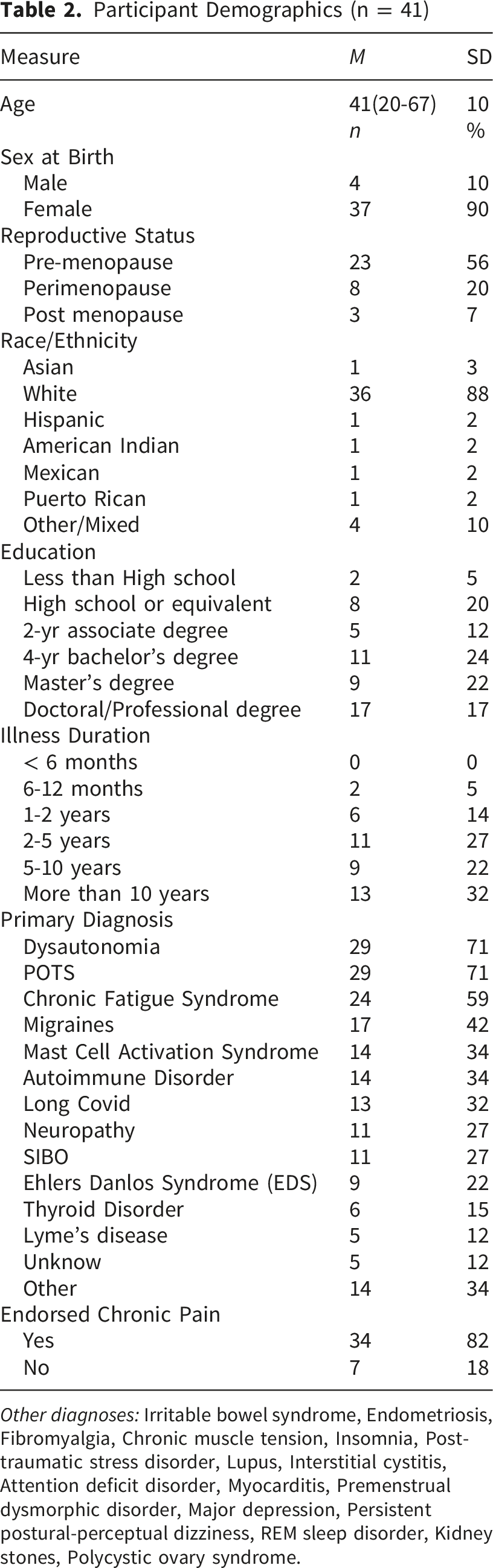
Other diagnoses: Irritable bowel syndrome, Endometriosis, Fibromyalgia, Chronic muscle tension, Insomnia, Post-traumatic stress disorder, Lupus, Interstitial cystitis, Attention deficit disorder, Myocarditis, Premenstrual dysmorphic disorder, Major depression, Persistent postural-perceptual dizziness, REM sleep disorder, Kidney stones, Polycystic ovary syndrome.
Acceptability and Feasibility
According to predetermined criteria, respondents described the 12-week program as both acceptable and feasible (Table 1). Participant satisfaction, measured on a 5-point Likert scale (1 = Not at all, 5 = Extremely), was high: 93% reported being satisfied, with 34% reported being extremely satisfied (n = 14), 44% very satisfied (n = 18), and 15% satisfied (n = 6). The remaining 7% (n = 3) felt somewhat satisfied, with no respondents reporting they were “not at all” satisfied. Regarding utility, 93% found the intervention helpful: 41% reported it extremely helpful (n = 17), 34% very helpful (n = 14), and 17% helpful (n = 7). Two respondents reported lower utility, with one finding it somewhat helpful and one finding it not helpful. Furthermore, 98% rated the program as relevant to their needs, with 59% reporting it as extremely relevant (n = 24); 27% very relevant (n = 11); 12% relevant (n = 5); 2% somewhat relevant (n = 1), and none reported it was “not at all” relevant. Program advocacy was also strong: 95% of respondents would recommend the program to others, two respondents were undecided, and no respondents reported they would not recommend the program. Finally, 100% of respondents reported the ability to maintain and generalize newly learned behaviors, and 100% reported being in ketosis at least some of the time.
No serious or life-threatening adverse events were reported; however, seventy-two percent of respondents reported adverse events across multiple biological systems and included flu-like symptom (i.e., nausea), fatigue and post-exertional malaise (PEM), weight loss, neurological symptoms (i.e., migraines, dizziness, pain, brain fog/cognitive impairment, light/sound intolerance), cardiovascular symptoms (i.e., tachycardia, chest pain), gastrointestinal symptoms (i.e., bloating, stool changes, loss of appetite), an uptick in neuropsychiatric symptoms (i.e., anxiety, depression, irritability), poor sleep, and shortness of breath. These symptoms align with baseline clinical presentation of IACI, as well as the transient “keto flu,” a well-documented constellation of symptoms that can emerge during the early phase of metabolic switching as the body adapts to increased fat oxidation and ketone utilization.
Perceived Benefits
When asked about global improvement following the 12-week intervention, 75% of respondents reported feeling, “A lot better” and 18% reported feeling “A little better.” Approximately 7% reported feeling “About the same” and no participant reported “Not much better.” Of respondents who described a particular symptom at the onset of the program, 85% reported perceived improvement in shortness of breath (n =20), 74% in quality of sleep (n = 35), 65% in gastrointestinal difficulties (n = 32), 63% in chest pain/tightness (n = 22), and 57% in brain fog (n = 33) during or immediately after the 12-week intervention. Respondents reported that symptoms continued to improve for up to 27 months post-intervention, with 100% reporting perceived improvement in shortness of breath (n = 20), 80% in quality of sleep (n = 35), 78% in gastrointestinal difficulties (n = 32), 90% in chest pain/tightness (n = 22), 70% in brain fog (n = 33), 96% in tachycardia (n = 35), 70% in PEM (n = 32), 80% in pain (n = 34), and 60% in fatigue (n = 36).
Optimization of the Intervention
Study respondents reported that the most important elements of the multicomponent intervention were 1 : Nutrition education and vitamin supplementation, 2 Social support, 3 Circadian rhythm entrainment, and 4 Mindfulness and meditation (Table 1); however, 82% of respondents made an unpromoted comment about the importance of the synergistic effects of the multicomponent intervention for symptom resolution. When asked about the duration of the 12-week program, 60% of respondents reported the program was ‘Too short’ and 41% reported the duration was adequate. No participant reported the 12-week program was ‘Too long.’ When queried about dosing, approximately 66% of respondents reported the number of weekly conference calls was “Just right,” 22% reported there were “Too many weekly calls,” and 12% reported there were “Not enough weekly calls.”
Discussion
This study provides a descriptive account of patient experiences with a fully remote, community-based, KMT and lifestyle program. Among respondents, the intervention was perceived as acceptable, feasible, and supportive of symptom improvement. Nearly all respondents endorsed recommending it to others. While the response rate and modest sample size suggest a potential selection bias toward individuals who experienced positive outcomes, these real-world data provide a necessary starting point for identifying responders in a currently underserved population.
The majority of respondents reported clinical presentations and diagnoses concordant with IACIs. Notably, although 70% of the sample experienced illness onset after 2020, only 32% had received a formal diagnosis of Long COVID. This discrepancy likely reflects established barriers to care, including limited access to specialized clinics, suboptimal clinician awareness, and documented diagnostic inequities. These findings align with broader epidemiological trends demonstrating a surge in autonomic dysfunction and ME/CFS following a SARS-CoV-2 infection. Secondary dysautonomia is estimated to affect nearly 80% of individuals with Long COVID. Specifically, monthly diagnoses of POTS have increased five-fold compared to pre-pandemic rates. 11 Similarly, the incidence of new ME/CFS cases has risen 15-fold. 12 The reported illness duration (six months to ten years) highlights a heterogeneous cohort with post-viral syndromes triggered by diverse pathogens. This heterogeneity underscores the necessity for future clinical trials to include a broad spectrum of IACI etiologies to better elucidate shared pathophysiological mechanisms. And while the majority of reported diagnoses are consistent with the IACI framework, it is important to acknowledge that several endorsed conditions, such as Ehlers-Danlos Syndrome and Small Intestinal Bacterial Overgrowth, may not be primarily classified as infection-associated; nonetheless, their inclusion is informative for characterizing the complex, multisystem symptom burden and comorbid landscape often observed in this population.
Regarding intervention acceptability and participant-reported experiences, more than 90% of this study’s sample population reported feeling ‘A lot better’ (75%) or ‘A little better’ (18%) following the intervention. The subjective reports of change spanned multiple physiological systems and symptom clusters. Respondents noted perceptions of change regarding fatigue and PEM, while neurological and cognitive reports included perceived changes in brain fog, sleep quality, and various pain clusters, such as general pain, migraines, and neuropathy. Regarding cardiorespiratory symptoms, respondents reported a perceived decrease in the frequency of tachycardia and shortness of breath; similarly, reported perceptions of change in the gastrointestinal and endocrine systems included those related to digestive difficulties and hormonal regulation.
While the current feasibility study design does not permit an assessment of efficacy or causal effects, these respondent-reported observations align with prior clinical case evidence suggesting that KMT, when combined with lifestyle interventions, may be a viable management strategy for IACI. 13 Notably, these accounts contrast with a recent population-based case-control study of 982 individuals, in which most working-age adults reported little to no change in fatigue, exercise intolerance, or cognitive symptoms during their second year of illness. 2 This discrepancy highlights the potential for multicomponent metabolic interventions to alter the expected clinical trajectory of these conditions.
These findings also support prior research indicating that multicomponent strategies combining dietary and mind-body interventions may produce synergistic benefits in chronic illness that a single-axis approach may miss.14,15 The specific components endorsed in this study align with current mechanistic theories. KMT is proposed to enhance mitochondrial energy, 5 downregulate pro-inflammatory cytokines, reduce oxidative stress, 6 and modulate immune function. 8 High-dose thiamine may reduce the IL-17 response and mitigate intracranial hypertension. 16 Similarly, circadian entrainment may address the autonomic dysregulation frequently observed following viral infection. 17 Mindfulness-based approaches have demonstrated neurobiological effects that support emotional regulation, cognition, and stress resilience, 18 and social support likewise contributes meaningfully to well-being in IAICs. 19 Together, these findings support a shift away from single-axis treatments, toward multicomponent interventions that address multiple biological systems in parallel.14,15
The absence of reported serious adverse events supports the safety of KMT in this population. Yet, the prevalence of transient symptoms during the metabolic transition presents a unique clinical challenge. Because metabolic induction symptoms, such as tachycardia and cognitive difficulties, overlap significantly with the baseline clinical presentation of IACI, investigators must be able to distinguish between transient induction effects and true disease exacerbations. To ensure participant safety and improve tolerability in future larger-scale trials, researchers should integrate comprehensive monitoring frameworks and proactive mitigation strategies directly into the study design. For example, future protocols should consider a phased reduction in carbohydrate intake over 14–21 days, which may mitigate the severity of acute side effects. This gradual approach may be particularly critical for patients with high autonomic sensitivity. Study designs should also consider utilizing daily digital symptom logs or “wearable” health trackers to monitor heart rate variability and tachycardia in real-time. This allows for the early identification of PEM triggers during the metabolic shift, enabling investigators to distinguish between transient induction symptoms and a true clinical relapse. Finally real-time access to clinical guidance may allow for the immediate adjustment of macronutrient ratios or electrolyte intake when moderate adverse events are reported, ensuring that respondents do not prematurely exit the trial due to manageable discomfort. By integrating these mitigation strategies, future trials can better support participant retention and ensure that the therapeutic potential of KMT is not overshadowed by the challenges of the initial metabolic transition. This proactive safety framework is essential for establishing KMT-LS as a feasible and acceptable intervention for the complex IACI populations. By balancing program duration with these proactive safety frameworks, future trials may better preserve the therapeutic potential of KMT for complex IACI populations.
Strengths & Limitations
This study is among the first to evaluate the feasibility and acceptability of a fully remote, multicomponent intervention that combines KMT with behavioral interventions for individuals with IACI, addressing a critical gap in current intervention development.1,3,4,20 The geographic diversity of the sample broadens the representation of patient experiences, and the findings highlight the perceived synergistic effects of multicomponent interventions, a factor directly relevant to the design of future trials.
However, several limitations must be considered. The cross-sectional design and reliance on retrospective self-reporting preclude causal inference and introduce the potential for recall bias. The modest sample size and response rate further suggest a possible selection bias, as individuals who perceived greater change may have been more likely to participate in the survey. Another significant methodological limitation is the lack of disaggregation between nutritional ketosis and high-dose thiamine supplementation. Given that benfotiamine may independently influence mitochondrial function and intracranial pressure, future research should utilize factorial designs to isolate the individual and synergistic effects of these therapeutic elements. Additionally, reported adverse events were common; however, because of the overlap between “keto flu” symptoms and the baseline clinical presentation of IACI, these cannot be attributed with certainty to the intervention versus underlying illness fluctuations. Finally, the absence of a control cohort and objective biomarkers preclude a definitive characterization of the physiological shifts attributable to the intervention. Nonetheless, these findings provide a necessary initial record of patient experiences to guide clinical translation and inform the optimization of future trial designs.
Conclusion
This cross-sectional study demonstrated that a fully remote, multicomponent program integrating ketogenic metabolic therapy, thiamine supplementation, circadian entrainment, and mindfulness-based resilience coaching is acceptable and feasible for individuals with infection-associated chronic illnesses, including post-viral dysautonomia, ME/CFS, and Long COVID. Respondents reported high satisfaction, strong program advocacy, and perceived multisystem symptom improvements sustained for up to 27 months, with no serious adverse events. These patient-reported experiences provide essential hypothesis-generating data to inform the design of future controlled trials. Specifically, these findings support the development of randomized controlled trials employing factorial designs to disentangle the individual and synergistic contributions of KMT, thiamine, and behavioral components; incorporating objective biomarkers, validated outcome measures, and real-time digital monitoring; and implementing phased metabolic induction protocols with proactive safety frameworks tailored to the unique clinical vulnerabilities of IACI populations. In the continued absence of FDA-approved treatments for these conditions, patient-informed feasibility data such as these are critical for accelerating the translational pipeline and ensuring that emerging interventions are safe, acceptable, and responsive to the needs of this substantially underserved population.
Footnotes
Acknowledgments
We thank the research participations who contributed their time, energy, and insight to make this project possible. We also extend our gratitude to the many providers and health coaches. Finally, we thank the millions of patients with infection-associated chronic conditions who continue to advocate, inform, and drive the science forward. Thank you.
Ethical Considerations
Our study was approved by the National University of Natural Medicine Institution Review Board (IRB # HZ102024).
Consent to Participate
All participants provided written informed consent prior to enrollment in the study.
Author Contributions
Dana Dharmakaya Colgan: Conceptualization, data curation, data analyses, visualization, writing, editing; DS: Writing, editing; TG: Data analyses, editing; MR: Intervention, recruitment; TW. Writing and editing; T.D. Writing, editing; HZ: Writing, editing Writing, editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Health for grant funding NIH (AT008924-08).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is available at request.
Discloures
DDC: No disclosures.
LB: No disclosures.
DS: No disclosures.
T.G: No disclosures.
MR: M. R. served as the nutritionist for the community-based program described in this study but had no role in study design, data collection, access to participant data or survey platforms, data analysis, data interpretation, or manuscript drafting. M. R.’s involvement was limited exclusively to providing nutritional guidance within the intervention, and did not extend to any aspect of the research process.
TW: No disclosures.
TD: No disclosures.
HW: No disclosures.
Statement of Human and Animal Rights
There were no procedures involving animals.