
Abstract
Families play essential roles in the intensive care unit (ICU), yet COVID-19 visitor restrictions disrupted patient- and family-centred care (PFCC). This study explored the impact of these restrictions and identified strategies to maintain PFCC when families cannot be physically present in the ICU. We conducted a qualitative descriptive study using semi-structured interviews with patients and loved ones who experienced ICU visitor restrictions during the pandemic. Participants were recruited from across Canada between January 2021 and April 2022. Transcripts were analyzed using inductive content analysis. Sixteen participants (11 loved ones and 5 patients) described significant challenges to PFCC. We identified four themes: 1) circumstances and context shaped lived experiences of visitor restrictions; 2) visitor restrictions disrupted information flow; 3) physical separation hindered loved ones’ roles as care partners; and 4) creative solutions could mitigate negative impacts. Restricted visitation policies significantly affected communication, advocacy, and emotional support. Participant-generated solutions—human-centered, technological, and informational—offer actionable strategies to preserve PFCC during future crises or when bedside presence is limited.
Keywords
Open visitation policies are a cornerstone of patient- and family-centred care (PFCC) in the Intensive Care Unit (ICU). 1 Best practice guidelines for PFCC in the ICU emphasize family presence in the ICU, family support, and effective communication with family members. 2 Adult ICU patients and their family members highlight the following priorities for PFCC in ICU: ongoing dialogue with healthcare providers, care that recognizes the humanity of patients and families, and supporting families to navigate their roles as advocates and supporters of the patient. This support includes the provision of practical aids and resources, preparing families for delirium, and engaging family in the patient’s transition out of ICU. 3 PFCC has been shown to reduce ICU length of stay and associated costs, while improving family satisfaction, patient experience, goal-concordant care, and mental health outcomes for both patients and families. 4 Family participation in bedside care is an essential element for facilitating PFCC. 5
During the early months of the COVID-19 pandemic, hospitals rapidly implemented restrictive visitation policies. By April 2020, hospitals from all provinces and territories had implemented significant restrictions to visitation. 6 These policies were primarily intended to protect patients and staff, and to conserve personal protective equipment. 7 However, organizations such as the Institute for Patient- and Family-Centred Care and the Canadian Foundation for Healthcare Improvement advocated for the elimination of restrictive visitation policies and the recognition of families as essential partners in care.6,8 Healthcare providers also raised serious concerns over hospital policies that prevented families from visiting their loved ones.9,10
Families fill multiple important roles when present in the ICU. 11 Loved ones may provide orientation or memory clues, sensory (vision, hearing) checks, and cognitive and therapeutic stimulation to the patient. 12 Family presence and participation in daily care can increase family satisfaction, improve patient outcomes, and decrease length of ICU stay.4,5,13 Despite these benefits of family presence in the ICU, pandemic visitor restrictions prevented loved ones from being physically present at the bedside and many loved ones reported challenges in maintaining a connection with healthcare teams and maintaining a connection to their loved one in ICU. 14 These challenges are still relevant for many ICU patients when their families cannot be physically present at the bedside.
We sought to understand the effect of restricted visitation policies on PFCC in the ICU by asking the following questions: 1) What do patients and their loved ones perceive to be the impact of visitor restrictions on PFCC in Canadian ICUs during the COVID-19 pandemic? 2) What solutions are identified by patients and families that can inform recommendations for PFCC when families cannot be physically present in the ICU?
Study Design & Methods
We approached the study from a constructivist orientation and conducted a qualitative descriptive study.15,16 A qualitative descriptive approach is characterized by its subjective epistemology, inductive process, acknowledgement of researcher subjectivity, and emic position of the researcher. This study was approved by the institutional research ethics board (University of Saskatchewan; BEH-1955, June 5th, 2020). Interview participants received a written informed consent form in advance and provided verbal audio recorded consent at the time of interview.
Participant Selection and Recruitment
We used purposive sampling to recruit participants who had either been admitted as a patient to a Canadian ICU during a period of visitor restrictions due to the COVID-19 pandemic, or who were the loved one of a patient admitted to a Canadian ICU during that period. To allow for a period of recovery and processing and to align with other research on ICU patient experience, we did not interview patients within the first three months after ICU discharge.
We utilized passive recruitment strategies across Canada from January 2021 to April 2022, to recruit participants who had experienced a variety of restricted visitation policies.
7
Strategies included posters and pamphlets placed in two tertiary ICUs; social media posts on Facebook, Instagram, and Twitter; bulletins in society emails, newsletters, and websites including with the following organizations: • the Canadian Critical Care Society, • the Canadian Foundation for Healthcare Improvement, • the Canadian Patient Safety Initiative, • the Health Authority Patient and Client Experience Program, • the Patient and Family Advisory Council Network, and • the Strategy for Patient Oriented Research Support for People and Patient-Oriented Research and Trials (SPOR SUPPORT) units, • the Provincial and National Associations of Social Workers, and • the Patient Voices Network.
We also asked healthcare providers to distribute posters to patients and their loved ones explaining the study and providing contact information for the study coordinator, and offered prospective recruitment during ICU admission. We provided an honorarium to participants in recognition of their time.
Data Collection and Analysis
A semi-structured interview was conducted by either phone or video chat by a research assistant (FB) (eSupplement - Interview guide). The interview audio was recorded and transcribed verbatim. Transcripts were returned to participants for review, editing, and approval. All participant interviews were included in our analysis.
An inductive content analysis was performed. Primary thematic analysis 17 (SS), and trustworthiness analysis was completed by the entire research team. SS reviewed all transcripts and wrote memos to capture key ideas and insights. An inductive and iterative approach to building a coding framework was then applied by developing codes closely related to participant ideas. Coding rules were established in an inductive manner and were captured in code notes, and a working summary of all codes was created based on the quotes assigned to each code. Codes were then mapped to research questions and reviewed for meaningful patterns or themes. Themes were synthesized with a narrative describing the theme/subtheme using direct quotes from the interview transcripts, and all transcripts were reviewed to ensure the ideas within were represented in the themes. The entire research team also reviewed at least one transcript each and participated in a facilitated group discussion, which was used to refine theme names, definitions, and the narrative description of the research findings.
Results
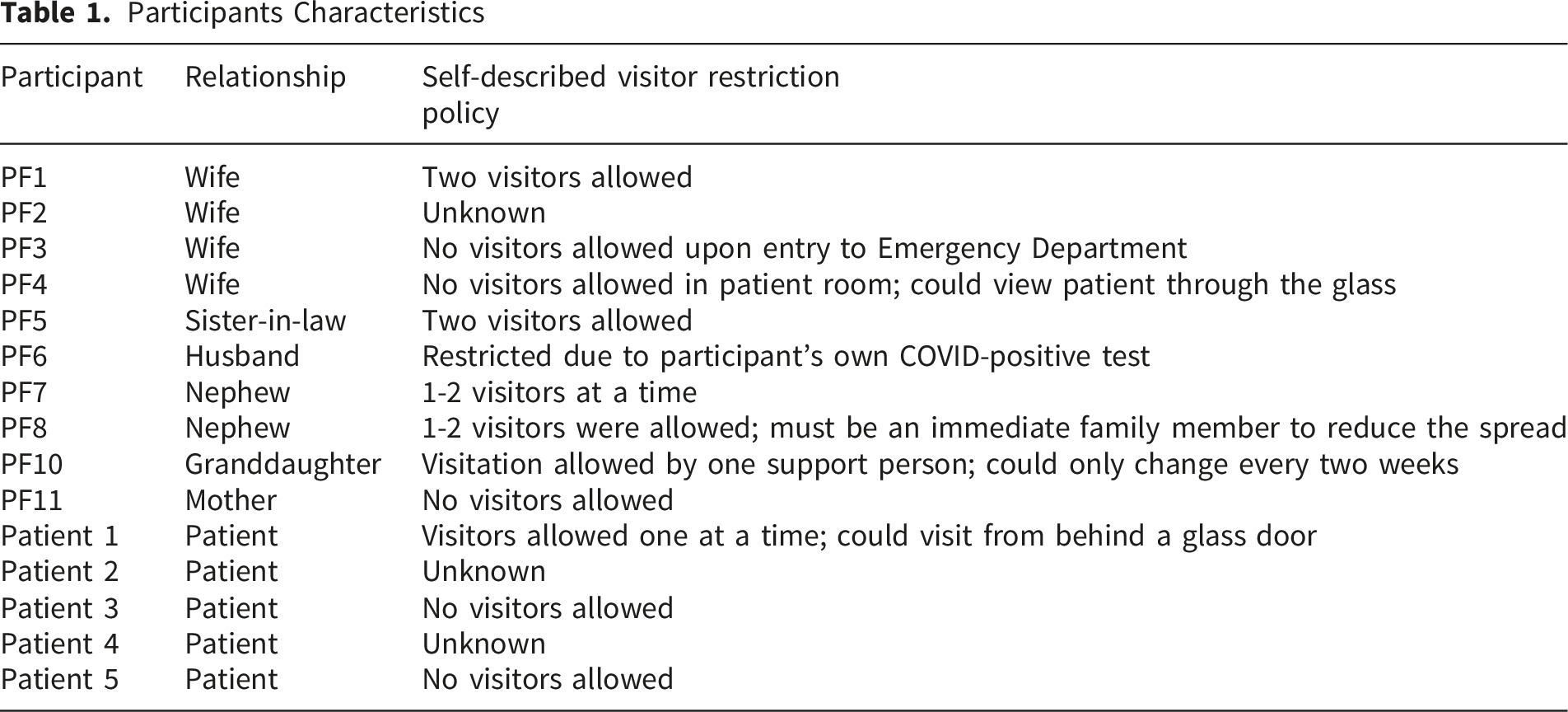
Participants Characteristics
Summary of All Themes and Subthemes

Theme 1: The Importance of Circumstances and Context on the Lived Experience of Visitor Restrictions
We identified three subthemes related to how circumstances and context impacted experiences of visitor restrictions. All participants carefully described how their unique set of personal circumstances, contextual factors, and life outside the hospital impacted their experience of visitor restrictions.
Personal Circumstances
Personal circumstances included how participants’ identity, actions, and other factors impacted their lived experience moving through the ICU. For example, one participant described the intersection of personal privilege and ability to advocate for visitation when the patient was a physician who worked for over 30 years in the hospital where he was admitted: “…because we were able to go in there each day, I didn’t really tell a lot of people that, because I didn’t know what other people could do, right? And I didn’t know if our family was just getting a little bit of extra care… I think being educated…we come from a medical family, we knew we could ask questions and we did. I think our experience might’ve been different than other peoples.” (Patient Loved One 4, Spouse)
Contextual Factors
Participants also expressed how the specific contextual factors related to the hospital environment (i.e. admission, visiting policies, physical environment, human resources) also impacted their lived experiences of visitor restrictions in the ICU. For example, one participant described their loved one’s challenges with navigating hospital human resources: “My husband would say that he struggled. He tried to call every day. He said, ‘I tried to be polite, to be understanding. Knowing that staff are run off their feet and they are extended beyond belief. I know that. I appreciate that. Are there certain times that I could call? Late, late at night? That just might be a better time to just have a conversation with someone?’” (Patient 5)
Another participant shared how the physical structures of the hospital made the visitor restrictions more challenging to navigate: “…my husband was very, very ill, and there was no private place where he [the physician] could talk to me…I had to be in the lobby, outside of the waiting room, and he had to come out there to me…then he realized that what he was gonna have to tell me, we really should be in a private place… he said, “I’ll come back and get you when we have a place to sit”…it wasn’t that private. There was still people wandering through there. It was just a space, an inside space, instead of being out in the lobby. So I was actually in somebody’s office space…so it wasn’t totally private.” (Patient Loved One 3, Spouse)
Life Continued Outside the Hospital
Several participants also emphasized how life outside of the hospital contributed to their experience of visitor restrictions. These experiences included major life events experienced without their loved one, feelings of profound isolation at home, and their own COVID-19 diagnosis while their loved one was hospitalized. For example, one participant described profound feelings of isolation without the patient at home: “…the impact on me was complete isolation, it’s just the two of us live together, so he wasn’t here, and …all of the sudden… I was supposed to be working from home, and then I was by myself, and then we were on physical isolation, you know nobody could go and see anybody, so I was just alone, so I ended up leaving, and going to [hometown], and staying there…” (Patient Loved One 1, Spouse)
Theme 2: Visitor Restrictions Disrupted the Flow of Information
All participants described how the COVID-19 visitor restrictions disrupted the flow of information between patients, their loved ones, and the healthcare team. Some participants highlighted how disruptions to the flow of information resulted in a perception of incomplete, inadequate, or incorrect information being shared. For example, a patient’s spouse stated “…knowledge is power right. Because if you have the knowledge, you can deal with it, it is the unknown” to illustrate the impact of incomplete information (Patient Loved One 2, Spouse).
‘Communication loops’ describe how information flowed naturally between parties. These were defined patterns of communication whereby information, updates, reassurances, or comfort were expressed and shared between members of the patient’s care team, which included patients, loved ones, and the healthcare team (Figure 1A). Information flowing (or not flowing) via communication loops* and communication circuits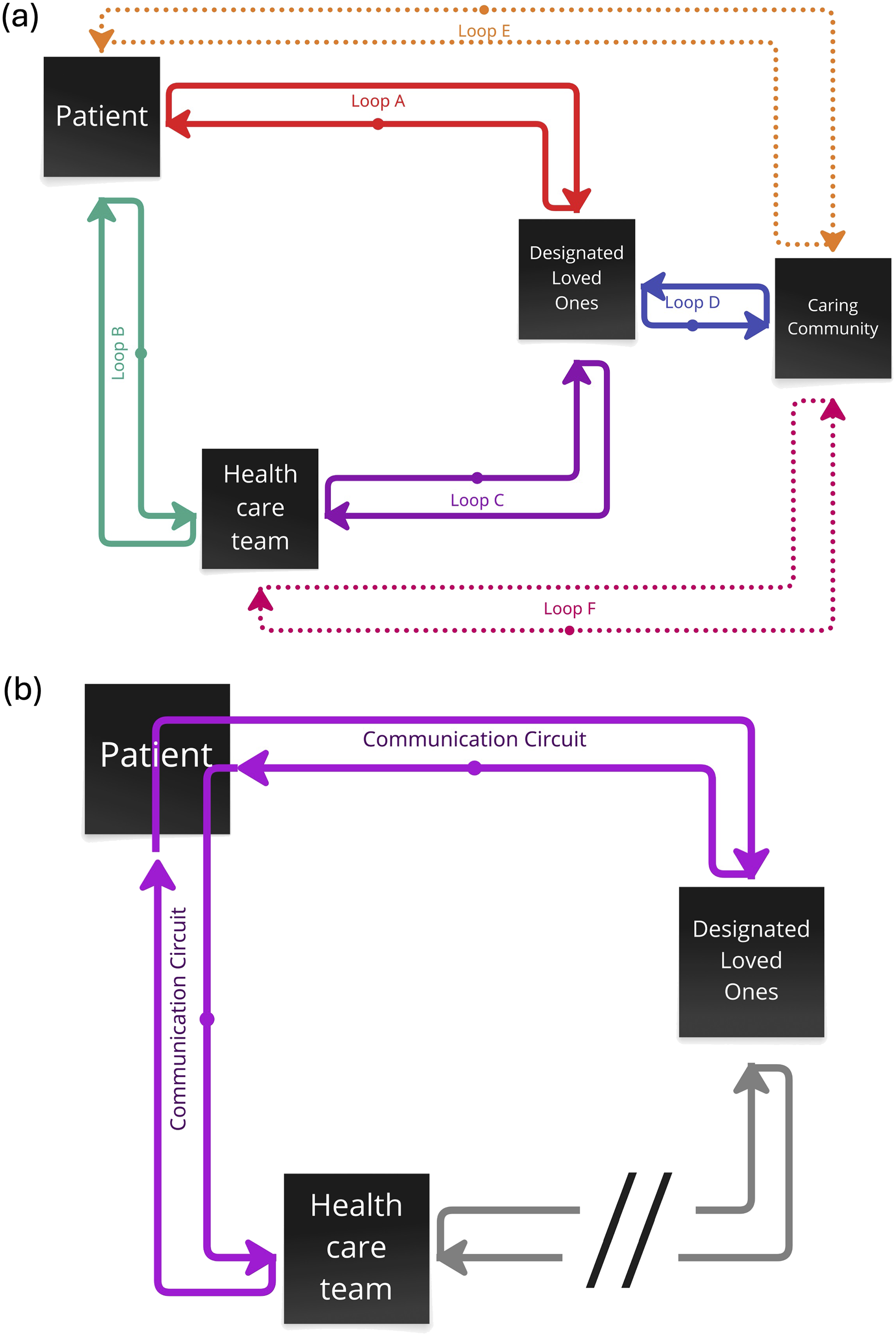
Participants distinguished two different groups of loved ones, described as ‘designated loved ones’ (i.e., the 1-2 individuals who were permitted by the healthcare system to visit the patient and/or receive information) and the 'caring community’ (i.e. everyone else; including additional family members not designated, family support networks, friends, religious groups, and others). Some loved ones expressed frustration with the limited number of permitted designated loved ones, as they self-described as being closely bonded to the patient, even though they were not ‘next of kin’ or ‘immediate family.’ For example, a niece described not being given the opportunity to visit at the bedside with their uncle, because they were not considered an immediate family member, “…we’re the extended family, but we used to live together have grown beside him as a dad too…they should consider the fact that despite the name that is just an uncle, they should just look beyond that.” (Patient Loved One 8, Niece)
‘Communication circuits’ emerged when communication loops were disrupted, as a way of fulfilling an unmet communication need (Figure 1B). For example, one spouse was not successful in getting satisfactory information from the healthcare team directly, so she worked to get answers to her questions by creating a list with her hospitalized spouse, and then asking him to call her with the answers. Patient Loved One 3 went on to reflect upon how the visitor restrictions necessitated this communication circuit, ““…I shouldn’t’ve had to put my husband in the middle. If I’d been available there, I wouldn’t’ve put him in the middle like that…”
Theme 3: Visitor Restrictions Interfered With the Role of Loved Ones as Care-partners by Hindering Physical Proximity
All participants described the impact of physical presence, or a lack thereof, on their experience and their ability to be part of the healthcare team and advocate for the patient. Participants described three levels of physical presence: at the bedside, distanced within the hospital, and distanced outside the hospital (Figure 2). Levels of proximity during COVID-19 visitor restrictions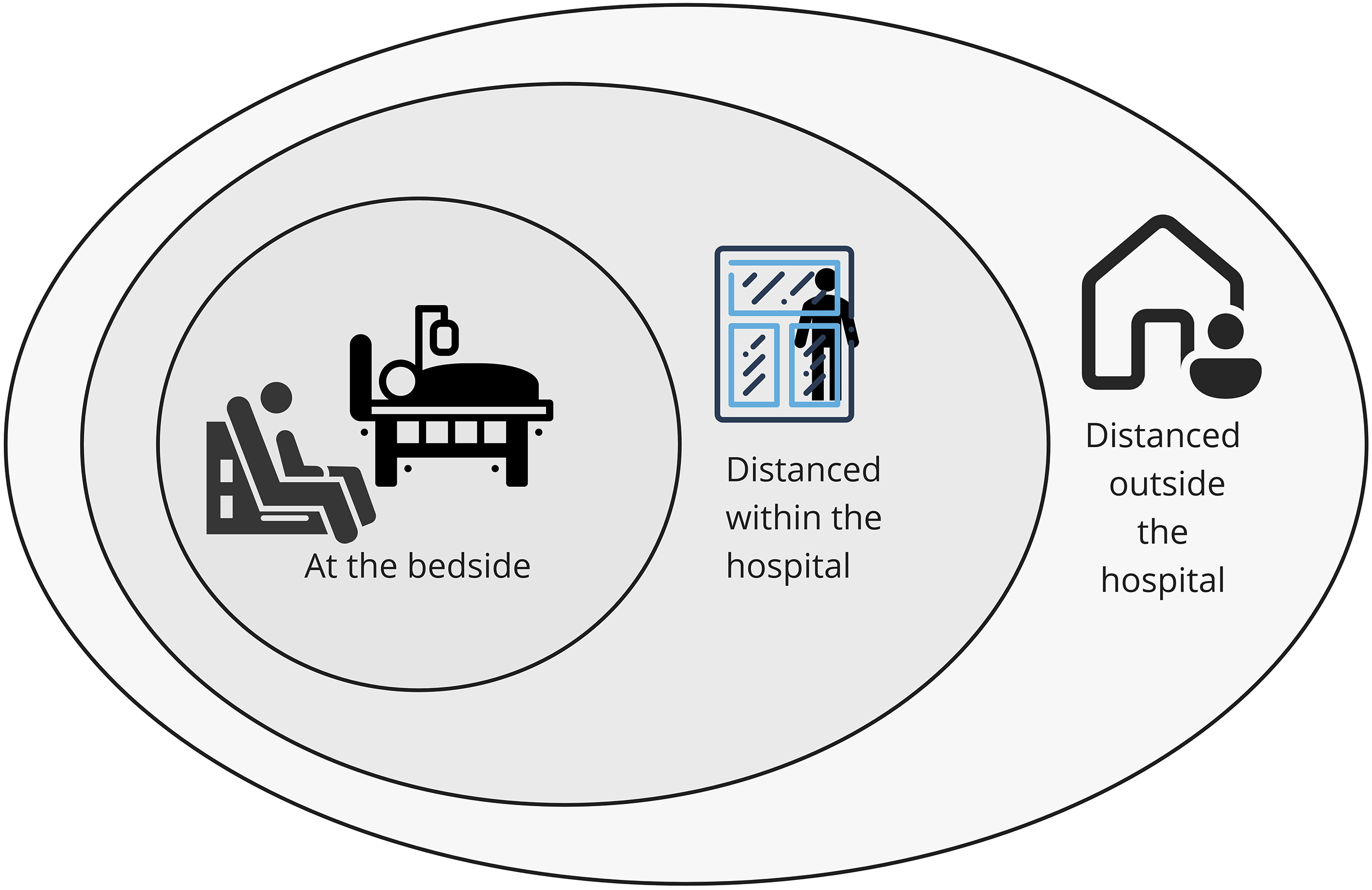
Loved Ones at the Bedside
Only a small group of participants was able to be physically present at the bedside during the patient’s ICU admission. Some participants highlighted the roles loved ones fill when they are permitted to be physically present (e.g. shower, other basic hygiene, change bed sheets, provide comfort during delirium).
Participants also described the importance of physical touch, for both patients and their loved ones, as a form of connection, an emotional support tool, and a method of caregiving. Others highlighted the importance of supplemental physical care provided by family members, including the burden on nursing staff when it wasn’t provided. Conversely, some participants described experiencing burnout, as they were unable to share the high burden of physical and emotional care with other, non-designated family members.
Loved Ones Distanced Within the Hospital
Several participants described a scenario where they were able to go to the hospital, but were not permitted to enter the patient room. They described being able to see the patient through glass walls, doors, or windows, and in some cases donning full PPE to be present outside the room. Participants in this scenario highlighted the communication challenges associated with this form of visitation, including physical distance, presence of barriers (such as doors, windows, or PPE). For example, Patient 2 described her frustration during her visual visitation with her son and mother: …They let the door open just a tiny crack, but I couldn’t hear anything I had the oxygen on…I found it very frustrating, not them being there but the circumstances, I was like ‘what’s the point.’ …I was glad that they came, it was nice to see them, but it was hard because you couldn’t talk to them…
Patient status (particularly delirium) posed a barrier to this form of visitation and several patients expressed confusion or frustration about why their loved ones weren’t coming directly to their bedside. For example, Patient 1 described his feelings as he emerged from his sedation, while his spouse was outside the room: …I know she was there for me… she was outside the room behind glass ….I felt resentful…I felt emotionally I felt that I was being confined and trapped against my will…I want out. Over time I became I guess a bit paranoid or suspicious ‘why isn’t my family getting me out of here?’
Loved Ones Distanced Outside the Hospital
Due to visitor restrictions, isolation requirements for family members, physical distance from the hospital, or being a non-designated family member; many participants were not allowed to enter the hospital. In these situations, they described using communications technology (e.g. phone, text, video chat) to remain connected, but explained that this was not always possible or feasible. Patients often required assistance to use devices and needed to rely on the healthcare team to facilitate this connection, and many loved ones described the emotional toll it took on them to not be able to see or touch their loved ones. Patients also described the emotional impact of not having family at the bedside, particularly noting that their loved ones would have been able to provide additional emotional care and alleviate anxiety. Participants highlighted how challenging it was to understand the status of the patient and/or make significant care decisions (e.g. code status) without being able to see them, and others emphasized the emotional impact of hearing these conversations between the healthcare team and patient without being there for support. For example, a patient’s spouse stated: “…it was just this absolutely helpless unknown, like should I be here and waiting, but yet I can’t go there, and just trying to make that decision, on what’s best, and then only being able to talk to doctors and nurses…people that don’t know you and don’t know him, and that’s the only information you can get, you can never really lay eyes on him…”(Patient Loved One 1, Spouse)
Theme 4: Creative Solutions Could Help Mitigate the Negative Impacts of Visitor Restrictions
Creative Solutions That Could Mitigate the Negative Impacts of Visitor Restrictions

Human-Centred Solutions
These included creating new roles and/or leveraging human resources in new ways to address some of the needs created by visitor restrictions policies. Participants suggested human centred solutions such as the creation of a Restrictions Coordinator position that could consider personal and local hospital circumstances, a ‘buddy system’ for loved ones to share experiences and ideas for navigating the ICU, volunteers or care assistants to support patients with communication technology, and spiritual leaders trained in contact precautions to visit patients at the bedside. For example, Patient 5 described the potential for personnel support “…someone that took care of … some of these personal things, like, ‘Is your phone charged today? Can I charge it and make sure that I come back and unplug it and bring it to you once it’s charged?’…And honestly, just to offer some encouragement, and even just to sit and have a conversation for a few minutes.”
Technology Solutions
Participants described technology-based solutions to support loved ones’ attendance at rounds and/or huddles with the healthcare team, communicating with the patient, and offering comfort through touch. These solutions included adapting existing technology such as phone or videoconference to support communication with the healthcare team and patient, and secure monitoring systems using a camera in the patient’s room for loved ones to view the patient on demand. Other participants suggested innovating new technology to address some of the communication and connection needs created by visitor restriction policies. For example, Patient 3 suggested technology to simulate the sensation of touch: “…you can put your hand on the screen and touch fingers, you know? Maybe have warm points on it… so you can feel touch.”
Informational Solutions
Some participants suggested information solutions to support loved ones in navigating the unknowns of the ICU environment. These included blogging to share the lived experiences of other loved ones in similar situations, which could include practical information such as the best times to call, and public information sessions about advanced care directives. Patient Loved One 6, a husband, described a desire for “…a road map…pre-emptive information that the hospital can give to family members to say this is where we are at, this is what we expect to see… If I could have a 5-page booklet… laying some of that out …to have an idea of what’s coming.”
Discussion
In this qualitative study, we describe the impact of pandemic-related visitor restrictions on PFCC in the ICU as perceived by patients and their loved ones, summarized as four themes: the importance of circumstances and context on lived experiences of visitor restrictions; visitor restrictions disrupted the flow of information; visitor restrictions interfered with the role of loved ones as care partners by hindering physical proximity; and creative solutions proposed by patients and their loved ones that could help mitigate the negative impacts of visitor restrictions on PFCC.
The findings of our study help clinicians and policy-makers contextualize and understand the rationale for preserving and enhancing PFCC principles in the ICU, both in pandemic and non-pandemic situations. Particularly, participants articulated the importance of communication with the ICU team and bedside presence with their critically ill loved one. In this study, we describe “communication loops” as an emerging concept. These “communication loops” help facilitate the flow of information between designated loved ones and the ICU team, but can break down and may not include everyone who is important to the patient. When communication was inadequate or prevented, loved ones experienced significant distress and went through great lengths to obtain necessary information. While technological solutions can bridge some communication gaps, both patients and loved ones identified the lack of bedside presence as a source of isolation, frustration and worry. Participants identified how delirium might exacerbate patient distress when alone, and the importance of seeing the patient in person in order to understand their medical condition. Together, the interrupted communication and bedside absence of loved ones in the ICU prevented loved ones from fulfilling their role as caregivers, advocates, and decision-makers. 18 In the ICU environment, where most patients cannot speak for themselves, shared decision-making is fundamental to good medical care. 19 This good medical care is therefore at risk when loved ones are prevented, by systems, structures, or policies, from participating in the ICU environment.
Our study also points to important contextual factors that could exacerbate existing power dynamics, or situations in which positional privilege can be used to mitigate communication issues with the ICU team. Additional contextual factors from the literature include limited access to care due to geographic or social factors, and the ways in which the physical ICU environment facilitates or limits family presence.2,4,5 Our team has previously demonstrated that consideration, or lack of consideration, for patients and loved ones’ diverse intersectional identities can build or break communication and trust in the ICU. Public health inequities were clearly exacerbated during the COVID-19 pandemic 20 ; however, the current study adds to the body of literature suggesting that these disparities need to be addressed holistically, rather than on a medical basis alone.
Patient and family-centered care in the ICU depends on the foundational ability of the healthcare team to meaningfully communicate with the patient and their loved ones. Strategies suggested by the literature, including flexible visitation policies, family support, and family engagement in the ICU all assume an ability to communicate and interact.2,5 During the COVID-19 pandemic, typical in-person communication was halted, and recommendations were developed to guide future visitor restriction policies so as to mitigate the effect of these policies on PFCC. 21 Participants in our qualitative study provided solutions that mirror a number of these recommendations, including personalized visitation policies (i.e. consideration of exceptional circumstances), the use of technology to facilitate communication, and the need for human connection with ICU patients that is often provided by families. Solutions and recommendations such as these require resources, planning, and structure in order to be actioned, as ad hoc solutioning can overburden individual healthcare providers.10,20,22 Our findings provide a depth of understanding and rationale for investing in these solutions; namely, to uphold best medical care in the ICU. Without a clear understanding of the potential harms of insufficient connection between ICU teams and families, policies that require additional resourcing can become de-prioritized in austere healthcare environments.
Strengths, Limitations, and Future Directions
Our work extends prior qualitative research on COVID-19 visitor restrictions 21 by narrowing our focus to patients’ and their loved ones’ perceptions of the specific impact of restricted visitation policies on PFCC, and offering comprehensive recommendations for situations in which families cannot be physically present at the bedside. Many of the points brought forward by participants have been previously discussed in the PFCC literature, and demonstrate the importance of physical presence to multiple elements of PFCC.2,22 Limitations of this study include the small sample, potential for selection bias in a non-representative sample from Canadian ICUs, limited demographic detail to support assessments of transferability, and variation in policies across time and settings. 7 We acknowledge that participants’ suggested solutions vary in terms of their feasibility.
The specific challenges and solutions described by our participants offer an opportunity to adapt future instances of visitor restrictions to a PFCC model and provide the actionable element of our study. While one objective of our study was to understand solutions from the patient and family perspective, the format of our study did not allow for robust, dedicated co-creation of solutions. We will use these findings as a starting point to develop feasible solutions with diverse patients, loved ones, and ICU healthcare providers.
Conclusions
In summary, we described the impact of COVID-19 visitor restriction policies on patients and their loved ones in the ICU as significantly interrupting communication flow and preventing loved ones from fulfilling their role as caregivers. Participants brainstormed solutions that align with robust recommendations from the literature, 22 and highlighted contextual considerations that point to the need for intentional consideration of equity in the development of future policies. This study provides a strong rationale for the importance of facilitating patient and family-centered care in pandemic situations and beyond.
Supplemental Material
Supplemental material - Impact of Visitor Restrictions on Patient and Family Perceptions of Care in Canadian ICUs During the COVID-19 Pandemic: A Qualitative Descriptive Study
Supplemental material for Impact of Visitor Restrictions on Patient and Family Perceptions of Care in Canadian ICUs During the COVID-19 Pandemic: A Qualitative Descriptive Study by Christine Patterson, Jennifer M. O’Brien, Salima Suleman, Faith A. Bae, Eileen Reimche, Candace A. Abramyk, Caitlyn Kitts, Sana Mohamad, Yolanda Palmer-Clarke, Joann Kawchuk, Sabira Valiani in Journal of Patient Experience
Supplemental Material
Supplemental material - Impact of Visitor Restrictions on Patient and Family Perceptions of Care in Canadian ICUs During the COVID-19 Pandemic: A Qualitative Descriptive Study
Supplemental material for Impact of Visitor Restrictions on Patient and Family Perceptions of Care in Canadian ICUs During the COVID-19 Pandemic: A Qualitative Descriptive Study by Christine Patterson, Jennifer M. O’Brien, Salima Suleman, Faith A. Bae, Eileen Reimche, Candace A. Abramyk, Caitlyn Kitts, Sana Mohamad, Yolanda Palmer-Clarke, Joann Kawchuk, Sabira Valiani in Journal of Patient Experience
Footnotes
Acknowledgements
We gratefully acknowledge the patients and loved ones who were generous in sharing their experience of COVID-19 visitor restrictions, as well as the support of the Saskatchewan Health Authority. We received funding from the Saskatchewan Centre for Patient Oriented Research and the College of Medicine, University of Saskatchewan.
Ethical Considerations
This project was approved by the University of Saskatchewan Behavioral Research Ethics Board in May 2020. Participants received a written informed consent form in advance and provided verbal audio recorded consent at the time of interview.
Author Contributions
All authors made substantial contributions to this work. All authors contributed to study design and were responsible for data analysis, data interpretation, and drafting the manuscript. All authors critically revised successive versions of the manuscript and approved the final version for submission.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We gratefully acknowledge funding from the Saskatchewan Center for Patient Oriented Research (SCPOR) Traineeship, the University of Saskatchewan College of Medicine CoMRAD Award (424092), and the Student Trainee Engagement with Patients (STEP) funding. Dr. Christine Patterson was funded through the Saskatchewan Center for Patient Oriented Research (SCPOR) PGME Traineeship. Eileen Reimche and Candace Abramyk, Patient Partners, received honoraria through the Student Trainee Engagement with Patients (STEP) funding from SCPOR.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The qualitative interview data generated and analyzed during this study are not publicly available due to privacy and confidentiality agreements with participants.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.