
Abstract
Gulf War Illness (GWI) affects many U.S. Veterans of the 1990-1991 Persian Gulf War (GWVs), yet recognition of the condition and effective treatments remain limited. GWVs with GWI describe feeling dismissed by institutions tasked with their benefits and healthcare, fueling mistrust and disengagement. This qualitative study explored the messages GWVs with GWI wished to convey to the Department of Veterans Affairs (VA) providers and U.S. policymakers. We conducted semi-structured interviews (2019–2022) with a national sample of 39 GWVs with GWI. Veterans emphasized persistent challenges in transitioning to VA care, navigating complex disability claims, and obtaining recognition of GWI as a chronic, service-connected illness. Participants perceived inequities in recognition, benefits, and other support compared to other service eras, and mistrust in compensation and pension processes. Finally, central to these GWI narratives was a desire to be heard, acknowledged, and validated. These findings underscore the importance of Veteran-informed policies, provider education, and empathetic and cooperative dialogue in restoring trust and improving care for GWI.
Introduction
The 1990-1991 Persian Gulf War (GW) involved a large-scale, multinational military operation in response to Iraq’s invasion of Kuwait. An estimated 200,000 U.S. servicemembers returned home reporting persistent, unexplainable symptoms. 1 Eventually, this constellation of symptoms—including chronic fatigue, pain, cognitive impairment, and gastrointestinal distress—became known as Gulf War Illness (GWI). Despite decades of research, few management strategies have demonstrated effectiveness in reducing the complex symptom burden of GWI.2,3
Many Gulf War Veterans (GWVs) have long reported feeling ignored, doubted, or dismissed by the institutions tasked with their care. 4 These experiences have contributed to a feeling of institutional betrayal—a failure by trusted institutions, such as the Department of Defense (DoD) and the Department of Veterans Affairs (VA), to validate, investigate, and address Veterans’ suffering. 4 GWVs have been told their symptoms were psychological, stress-induced, or signs of aging, despite growing evidence of distinct multi-symptom patterns associated with GW service. 5 Recent research found that dismissive provider interactions and poor communication about illness can exacerbate mistrust and reduce treatment adherence among Veterans with medically unexplained symptoms (a term to describe physical symptoms with no attributed root cause 6 ) with overlapping features of GWI.5,7
To date, there have been no studies directly examining GWVs’ perspectives on how the VA cares for GWI, and there is still a paucity of qualitative data to elucidate how GWVs with GWI construct and communicate messages and recommendations they believe would improve provider and institutional understanding to ultimately improve care for GWI. The primary aim of the overall study was to amplify patient voices in Gulf War-related research and clinical care to improve understanding of illness experiences, treatment, and care. This analysis addresses this goal by identifying messages that GWVs believe are crucial for providers and institutions to understand, thus addressing a critical gap in the literature. These messages and recommendations offer direct insight into GWVs’ priorities, explanatory frameworks, and unmet needs, which are central to improving patient-centered care and system-level responsiveness.
Methods
This manuscript uses data from VA project Listening to Gulf War Vets: A Qualitative Inquiry into the Health Experience and Treatment of those with Chronic Multisymptom Illness (Joint IRB OHSU/VHAPORHCS 17470/3786). Health Experiences Research methods (formerly known as Database of Individual Patient Experiences) were used,8,9 and detailed in previous publications.7,10
Recruitment and Eligibility
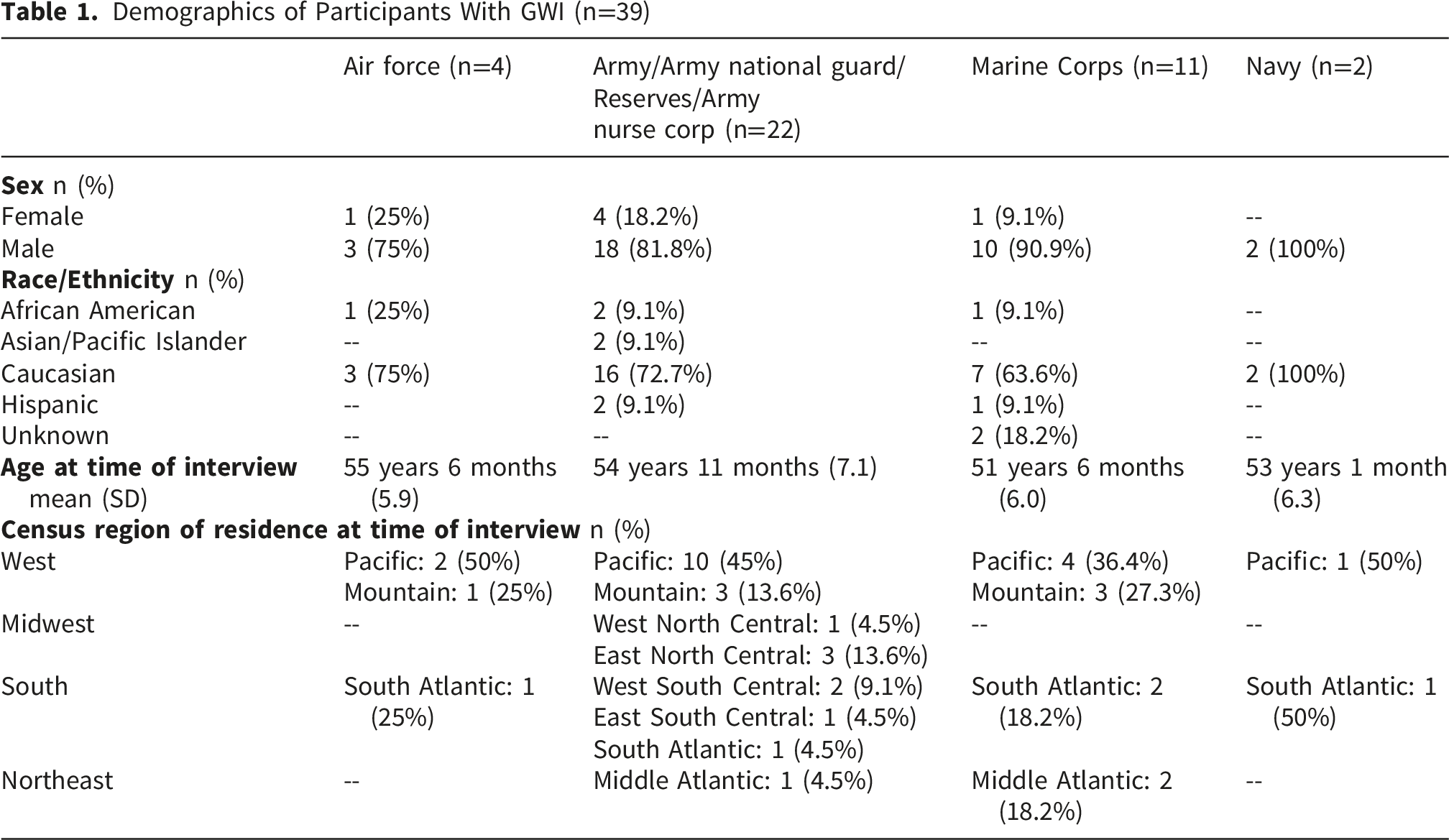
We used a combination of flyers, word-of-mouth, and clinical relationships to recruit a national sample of GWVs, including Active Duty, Reserves, and National Guard units, regardless of deployment or illness status. Veterans who were in the military during the 1990-1991 GW, were willing to be audio recorded, and were cognitively able to provide informed consent were determined to the eligible for the study. We employed maximum variation sampling based on clinical and sociodemographic factors to capture a large range of stories and experiences. While GWVs with and without GWI were interviewed (n=59), this analysis focuses on the messages and recommendations GWVs with GWI (n=39) had for policymakers and providers (VA and non-VA).
Data Collection Procedures
Two study team members used a semi-structured interview guide to ask questions about military, healthcare, and life experiences (supplemental material). These 2- to 4-hour-long audio- and if willing, video-recorded interviews were conducted in-person or, after March 2020, virtually. Participants were paid $50 for their participation and had the ability to stop the interview at any time. Recordings were transcribed, then checked for accuracy and de-identified by a study team member.
Qualitative Analysis
A coding scheme and codebook were iteratively developed over the first several months of interviewing and open coding. After each of the first 10-15 interviews, the interviewers met to discuss potential codes and future avenues of inquiry that appeared during the interview that just took place. Transcripts were dual-coded by K.M and S.N.. If codes were added later in the process, all prior transcripts were re-coded to include new codes, when applicable. Thematic saturation was met when all parties agreed no new significant ideas were illustrated in the transcripts. Using Atlas.ti 22, 11 coded transcripts were used to generate code reports, which were analyzed using an integrated approach of inductive thematic analysis and content analysis for topical themes. 12
Reflexivity
It is important to take into consideration the positionality of the authors, and its potential impact on the analysis and interpretation of results. All authors are Caucasian-identifying; three are cis-gender females, and one is a cis-gender male. All authors have completed a Master’s degree or higher (M.D., Ph.D.), and each have 5-11 years of experience working inside of the VA healthcare system. One author is a US military Veteran, and two authors have immediate family members who are US military Veterans. Finally, the authors range in age from their 30s to their 60s and have varying levels of experience with illness and interactions with healthcare systems.
Results
Demographics of Participants With GWI (n=39)
When asked about their motivation to participate in this study, participants overwhelmingly cited a desire to help other GWVs or future generations of military servicemembers feel heard and understood, and to contribute to potential solutions for problems that have plagued them and others. Threads of optimism that their stories could improve healthcare for GWI, enhance recognition of service-connected illnesses, and create a more supportive system were interwoven throughout their narratives. Below, we summarize GWVs’ key messages to the U.S. government, DoD, VA, and providers. Pseudonyms are provided with quotations to humanize experiences. 1. DoD and VA roles in the experiences of GWVs compared to other service eras around learning about, enrolling in, and receiving VA benefits – Messages to DoD and VA leadership a. Limited information about VA services upon transitioning home or military out-processing
A chief complaint was the lack of effective communication about initiating VA services upon discharge from the military. Participants, including Phil, expressed frustration with the chaotic nature of being discharged without any information about VA services: “We were activated, then we get done with the war, they ship us back. We go back to an active-duty base for a couple of days. Then they ship you right back home. You’re released; you’re back to your normal life... They didn’t do a very good job of explaining VA benefits or even to go to the VA.”
A solution suggested by numerous participants was to include a post-deployment physical as a required element of “returning” from active duty. For instance, Merle said if he were in charge: “Every Veteran who comes out would have their C&P evaluation before they left the military. They’d be evaluated, they’d be granted whatever they’re going to be granted, and they’re given a healthcare card.” Compensation and pension exams (C&P exams) are comprehensive health exams by providers at either the VA or with third-party contractors. They are important when leaving the military because they directly affect access to various VA disability benefits, healthcare, and long-term support. Dale recommended a mid-career event where representatives advise servicemembers what is available to them once they leave the service and “if you feel you’re having problems, this is what you need to do right now, and have that system, because I know there’s a joint system between the VA and DoD systems.”
b. The government not applying lessons learned from Vietnam-era Agent Orange exposure to GWVs with GWI
GWVs expressed needing to feel acknowledged by both the government and their providers. There is a disappointment that lessons learned from the Vietnam-era Agent Orange health crisis were not translated into care for GWVs. Bob and Ralph among others, believed the powers-that-be were “waiting for us to die.” Walker explained: “It took 30 years for the Vietnam Vets for Agent Orange, and it’s the same timeframe for the Gulf War Vets… We have our own running joke, most Vets. They hope we die off, so they don't have to pay us… Just treat us like human beings.”
Participants want the DoD and VA to take responsibility for the health-related consequences of military service, as they eventually did with Vietnam-era Veterans. Ralph said he hopes “for the VA to get to the point they got to with Agent Orange at some point. They denied, denied, denied, and they finally came and said ‘okay, all right you got us. Okay, we’ll book treatment.’” Ryan wishes for a “better organized VA system and more responsibility of the VA taking care of us,” and an admission of the clear-cut role those military exposures had on their ongoing health problems: “I just want ‘em to admit to what they have done.”
c. Feeling forgotten: Inequity in VA services available to more recent eras
GWVs can see VA has made strides since the GW and believe they are treating the post-9/11 Veterans with more care: “I mean when they come out of Iraq and Afghanistan, they have got a ton of support for them through VA… They’re doing a lot better,” (Ronnie). These perceptions have led to some animosity about the inequities between service eras. Colin stated, “They don’t take care of us the way they take care of post-9/11… [they] get way more benefits than the Gulf War.” There is frustration that “both served time overseas, but if you’re post-9/11 it’s like they’re better than us,” (Jerry). 2. Challenges and recommendations within VA Healthcare System – Messages to VA Leadership a. Mistrust in the service connection claim process
Navigating entry into VA services exposed weaknesses in the disability claim exam (also known as compensation and pension [C&P]) process. There were gaps in what GWVs told examiners and what was ultimately documented: “Compensation and pension exams, totally untrue. Totally not what I told them at all,” (Holly) and “I’ve had some really excellent examiners for my C&Ps. I had others that, when you walked in the room, you just knew that whatever you said is gonna go out the window,” (Jimmy). Several participants with GWI ultimately hired lawyers to appeal the results of their claim exams: “It was a whole list of issues, and they denied it and so I hired an attorney after the second denial… I needed guidance. I needed help,” (Ralph). GWVs felt they should not require attorneys to be “treated fairly” by examiners. For some, like Holly, the tone of the denial letters added insult to injury: “You get letters that are not nice… There’s easier ways to talk to people and deescalate the situation. It gets to some of these guys. Especially when they're in a bad place anyways, mentally, physically, or both. The first thing I would change is the C&P, and the way they write these letters.”
The cracks in the C&P process became chasms for some GWVs who described a “frustratingly slow” process. When asked about their experiences getting service connected, most GWVs expressed frustration, Jerry remarking he “already fought a war” and questioning why he “ha[s] to fight” for benefits. Lack of transparency in the service connection process was highlighted by Billy, who said he understands that it took a long time for GWI to be recognized as a service-connected condition, but did not understand “why after 15 years and a diagnosis” he was still denied benefits. Jimmy recommended developing a database to track the locations of Veterans, enabling better identification and treatment of exposure-borne illnesses found among servicemembers who spent time in specific regions. Like other GWVs, Ryan recommended a “streamlined process that actually takes the Veterans into consideration.”
For several participants, a serendipitous encounter with a Veterans Service Officer (VSO; a no-cost, trained, accredited professional who helps Veterans navigate applying for and receiving VA benefits, like disability, pension, and education) or recently transitioned servicemember were the only reasons they knew to visit VA. Bob explained: “I had no idea what a VSO was. I barely had an idea of what the VA was. I was working at a little medical supply place and one of the VSOs came in. And I don’t know how he figured out that I was a Veteran, but we started talking about it, and he goes, yeah, I’m a Veterans Service Officer. You should come see me.”
GWVs wished they had been “hooked up” with a VSO or other VA or Veterans Benefits Administration (VBA) coordinator right away, rather than having to navigate the complicated systems themselves.
b. Need for more VHA-wide and provider-level recognition of GWI as a long-term, service-connected illness – Messages to VA providers
GWVs thought difficulties receiving GWI-related service connection and accessing treatment pathways were attributed to the dismissal of their symptoms as a serious problem, historic denial of GWI as a long-term, service-connected illness, and lack of care coordination that normally comes with chronic health conditions. A common message from participants to providers was that they need to do a better job of listening and acknowledging, rather than dismissing, symptoms. Symptoms of GWI can overlap with other health-related issues that occur with age, and some participants, like Walker, felt his provider attributed his symptoms to age rather than service-connected exposure: “They told me, oh, it’s all because I’m getting older. It’s old age… But getting old isn’t supposed to hurt like this.” Jerry was worried GWI would not be properly recognized in time for the aging population it affects: “It’s getting worse because we are getting older. Now, when they finally do recognize it, it’s going to be too late.” And some, like Shania, felt her GWI was getting worse with age: “It is a real thing, and it is a thing that lingers. After almost 30 years it hasn’t gone away, it’s actually gotten worse. There’s certain things that progress with age and I think that the Gulf War Illness is part of that.”
Actively listening and creating a compassionate, cooperative dialogue between patient and provider can “go a long way… [toward] at least acknowledge[ing] that I’m a human being and that I have a problem” and taking steps to “understand our disease,” (Parker). GWI has been under-diagnosed and poorly understood for decades, and GWVs felt this was partially due to not being believed, Dolly explaining “they need the system to believe that there really could be something wrong with them, and it really could be service connected, even if it’s been 20 years since they’ve been in the service.”
Some participants, such as Parker, felt providers should educate themselves about GWI: “Avail yourself to the information that’s out there. Gain some knowledge.” Additionally, providers should keep open lines of communication during the diagnostic journey: “Let the Veteran know what happened with [the tests], whether it’s good or bad, because I always thought that no news is good news... [but] people fall through the cracks,” (Jackson).
Discussion
Here, we present the messages and recommendations of 39 GWVs with GWI, who were interviewed between 2019 and 2022. Across interviews, GWVs described persistent challenges navigating entry into VA care, frustration with the disability claims process, and a perceived lack of recognition of GWI as a legitimate, service-connected condition. Participants emphasized that these experiences shaped not only their access to care and benefits, but also their trust in VA and its ability and willingness to adapt to their needs. Importantly, GWVs expressed hope that their experiences, and the messages embedded within them, would reach policymakers and VA healthcare providers, informing improvements in services tailored to the unique needs of GWVs with GWI.
Beyond structural messages and constructive criticism, our findings contribute novel insight into how GWVs construct and communicate their illness identity. To date, limited research has examined what messages GWVs with GWI believe would improve provider and institutional understanding and care. Literature on medically unexplained symptoms and fibromyalgia offers relevant parallels, as these conditions share features with GWI, including diagnostic uncertainty, stigma, and histories of patient–provider mistrust.13,14 Participants in our study often framed recommendations and messages in constructive ways, reflecting upon care they wish they had access to and how they wish they had been treated. A key finding was a desire to “be believed” that GWI is a debilitating condition warranting the same seriousness as any other service-connected illness. In the context of diagnostic and treatment uncertainty and patient provider mistrust, prior research demonstrates that communication strategies, such as a Concordant Care Model, 15 characterized by validating patients’ experiences and engaging their explanatory models, can improve satisfaction, trust, and treatment adherence.15-18 Our findings suggest a similar communication approach would be particularly important for GWVs.
The most actionable messages were directed upstream to the DoD and VA leaders responsible for structuring transition out of service—GWVs we interviewed consistently expressed frustration over the absence of structured guidance when transitioning out of military service, particularly related to accessing VA benefits and healthcare. Several recommended mandatory post-deployment physicals and evaluations prior to discharge to streamline benefit eligibility and continuity of care. These findings align with existing literature demonstrating that the transition from military to civilian life presents substantial challenges, especially in navigating VA healthcare systems.19-23 Although transition programs have been piloted over the past decade, 24 GWVs who separated in the mid-1990s described minimal support from either the DoD or VA. This early lack of guidance, participants suggested, laid a foundation of confusion and distrust that has persisted for decades.
Their experiences rarely improved once they were able to undergo their C&P evaluations and disability claim process. GWVs’ frustrations with claims processing echo long-documented systemic deficiencies, suggesting these messages are not only experiential, but institutional. Echoing participants’ overwhelmingly negative experiences, the U.S. Government Accountability Office (GAO) placed the VBA on its “high-risk” list in 2003 due to fundamental problems with outdated criteria and claims processing inefficiencies, 25 and 10 years later the need for improved training for claims processors recommendation remained. 26 Despite these findings, GAO reported in 2021 that the VBA had still not fully adopted leading federal training practices, 27 and by 2024 only six of ten recommendations had been implemented. 28 Further, while VA providers have been diagnosing GWVs with other multisymptom illnesses like Chronic Fatigue Syndrome, Fibromyalgia, and Irritable Bowel Syndrome as a proxy for Gulf War Illness for at least two decades, it was not until October 1, 2025 that an International Classification of Diseases (ICD)-10 code (a standardized way to record the presence of a diagnosis) for GWI was introduced, 29 34 years after the GW and when some started presenting with the illness.30,31 The systemic challenges and “achingly slow” progress of improvements have been felt by GWVs, further validating their complaints regarding the lack of acknowledgment of GWI as a service-connected condition for which they can receive VA care.
Once able to receive VA care, the GWVs we interviewed understood that VA providers must often operate under a system that was not necessarily designed for out-of-the-box approaches to the unique needs of a seldom-understood health condition like GWI. They stressed the continued need for provider education on symptoms, evaluation, and treatment options for GWI. Specifically, GWVs recommended providers have a more empathetic and compassionate dialogue with them when discussing GWI. This is supported by recent research on using the Concordant Care Model in patient-provider communications with GWVs with GWI, and its ability to establish patient-provider trust by legitimizing patient experiences and demonstrating knowledge and a willingness to understand GWI. 15 This model emphasizes the importance of validating the patient, creating a shared understanding of the concern, and co-creating an action plan to address it.
Veteran-Identified Needs and Recommendations for Improvement
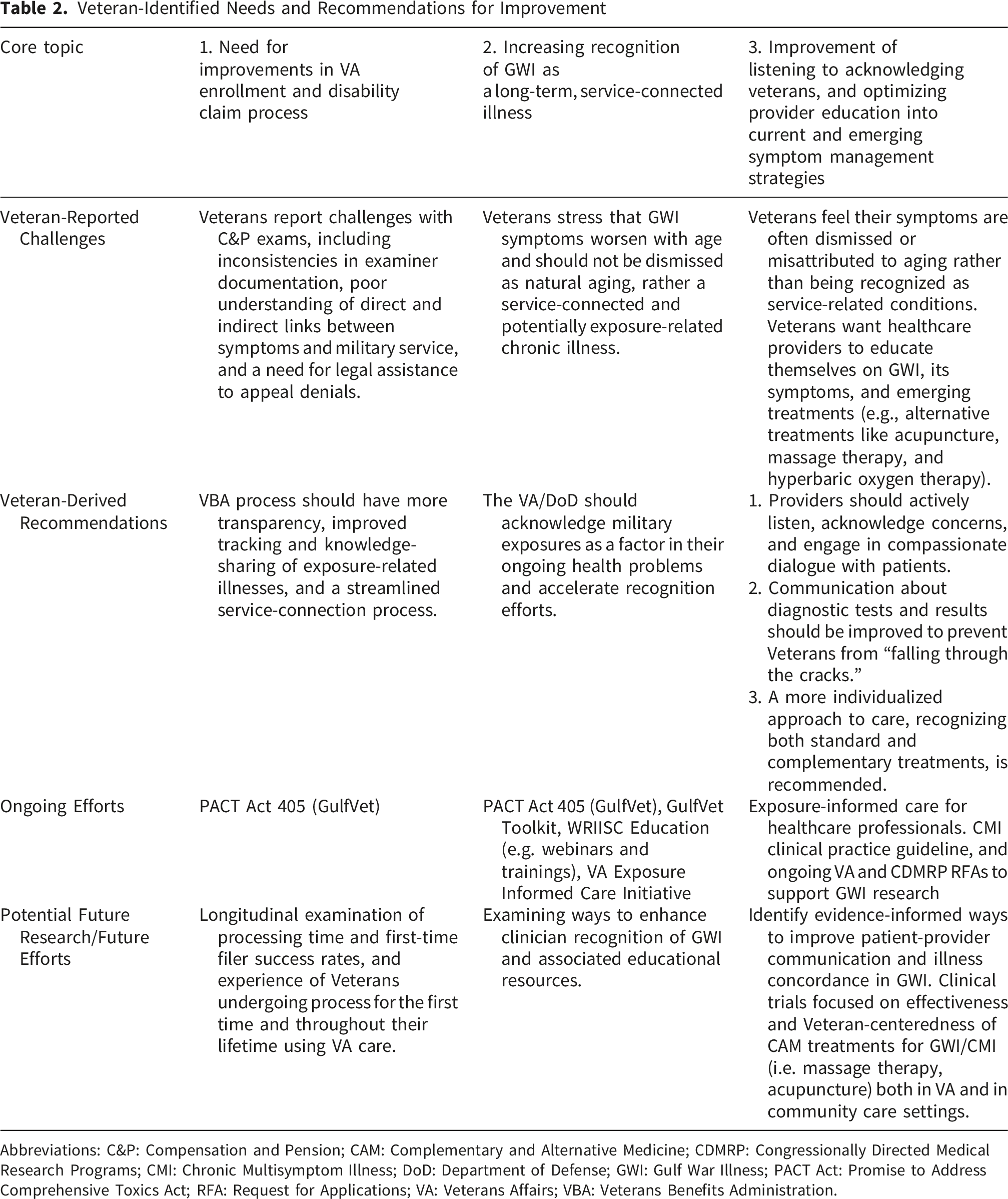
Abbreviations: C&P: Compensation and Pension; CAM: Complementary and Alternative Medicine; CDMRP: Congressionally Directed Medical Research Programs; CMI: Chronic Multisymptom Illness; DoD: Department of Defense; GWI: Gulf War Illness; PACT Act: Promise to Address Comprehensive Toxics Act; RFA: Request for Applications; VA: Veterans Affairs; VBA: Veterans Benefits Administration.
Limitations
Results of this study should be interpreted with limitations. Since the GW, and since obtaining these stories in 2019-2022, improvements to the VHA have been made that were not captured in these interviews; yet we attempted to contextualize findings with recent policy changes and evolutions in VA care. As with most qualitative research, results have limited generalizability, especially due to the specialized population (GWVs with GWI). Relatedly, this manuscript focused on suggested improvements from a population that has historically experienced many challenges, thus we rarely heard positive experiences or messages. While we attempted to reach maximum variation sampling, these patient experiences are not comprehensive of all experiences with healthcare systems. These interviews span decades of personal and emotional recollections, so while this work was grounded in perception and experiences, there is a risk of recall bias.
Conclusion
This study amplifies the voices of GWVs with GWI, revealing challenges in communication, benefits navigation, and equitable recognition of their illness. Participants’ messages underscore the need for streamlined transitions, greater acknowledgement of service-connected conditions, and broader access to individualized care and treatments. While recent legislative and policy changes represent progress, our findings highlight that historical gaps in recognition and care continue to shape Veterans’ trust in VA. Addressing these concerns with sustained institutional commitment and Veteran-informed policy is essential to improving health outcomes and restoring trust. Beyond Veteran care, messages of improved patient navigation, compassion around under-recognized conditions, and emphasis on continued provider education can positively impact all realms of patient experiences and care.
Supplemental Material
Supplemental Material - “Treat us Like Human Beings”: Messages and Recommendations to U.S. Policymakers and Veterans Health Administration Providers from a Qualitative Inquiry into the Health Experiences of Gulf War Veterans With Gulf War Illness
Supplemental Material for “Treat us Like Human Beings”: Messages and Recommendations to U.S. Policymakers and Veterans Health Administration Providers from a Qualitative Inquiry into the Health Experiences of Gulf War Veterans With Gulf War Illness by Kara A. Montague, Megan Lafferty, Michael Graham, and Shannon M. Nugent in Journal of Patient Experience.
Footnotes
Ethical Considerations
Ethical approval to report this case was obtained from Oregon Health and Science University/VA Portland Health Care System Joint IRB (17470/3786).
Consent to Participate
Written informed consent was obtained from the participants for their anonymized information to be published in this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: VA Health Services Research and Development, SDR-17-151 (PI: Helfand/Nugent).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
De-identified data are available upon request (Patient Narratives Repository OHSU/VHAPORHCS IRB 10085).
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the Oregon Health and Science University/VA Portland Health Care System Joint IRB (17470/3786) approved protocols.
Disclosure
The Department of Veterans Affairs did not have a role in the conduct of the study; in the collection, management, analysis, or interpretation of data; or in the preparation of the manuscript. The views expressed in this article are those of the authors and do not necessarily represent the views of the Department of Veterans Affairs or the U.S. Government.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.