
Abstract
Care partners of people living with dementia (PLWD) report significantly higher levels of stress, anxiety, and depression than non-care partners. Mindfulness-based programs improve overall well-being, but little research has evaluated the impact of emotional resilience programs for care partners of PLWD. This study reports the design and implementation of a pilot emotional resilience training initiative for care partners of PLWD. Three sessions were held at a monthly care partner support group. Emotional regulation skills were assessed using self-recorded emotional shifts before and after resilience practices. The feasibility and acceptability of the program was assessed using feedback collected through a post-survey and focus session. After participating in resilience practices, 82% of participants reported experiencing increased positive emotion. Most participants plan to use the program tools in the future and agree that their overall well-being improved after the training. Participants also noted that this program would be impactful for other care partners. The findings of this pilot study provide evidence that emotional resilience training may be a beneficial support strategy for care partners of PLWD.
Introduction
There are nearly 12 million care partners of people living with dementia (PLWD) who provide unpaid care in the United States. 1 Care partners of PLWD face tremendous stress daily. This group reports higher levels of care partner burden and psychological distress when compared to other types of care partners.2,3
Care partner burden can be defined as the “multidimensional response to physiological, emotional, social, and financial stressors associated with the caregiving experience”. 4 This burden can lead to increased rates of anxiety, depression, poor quality of life, chronic health conditions, and premature death in care partners.1,4,5 Care partners are often viewed as the “invisible patient,” bearing significant mental and physical health challenges that go unnoticed. 6 Worsening care partner burden can also lead to detrimental impacts for the patient, including poor quality of care, early institutionalization, elder abuse and neglect.6,7 It is crucial to develop evidence for strategies that support care partners of PLWD using a humanistic perspective in an environment emphasizing kindness, safety, and trust. 8
Although mindfulness training can increase positive affect and improve well-being in the care partner population, minimal research has explored emotional resilience training as a potential tool to improve well-being of care partners of PLWD.9,10 While mindfulness interventions emphasize present-moment awareness and attentional practices, emotional resilience training focuses on the applied development of strengths-based emotional regulation, adaptive coping, meaning-making, and values-aligned action in response to life stressors. Emotional resilience training emphasizes mechanisms such as stress reactivity, recovery, executive functioning, and adaptive appraisal while mindfulness practices function as a contemplative practice. Overall, emotional resilience is a purpose-based, evidence-informed approach to train one’s ability to effectively adapt and respond to stressful situations, and it is a skill that can be taught and developed over time. We report here the results of a pilot training program that aims to increase care partner emotional resilience while they provide high quality care to their loved one(s).
Methods
The pilot study used a mixed methods approach combining qualitative and quantitative measures to explore preliminary changes in emotional regulation and feasibility and acceptability of the program. Emotional regulation was evaluated using self-recorded emotional shifts before and after resilience practices such as heart-focused breathing (Appendix A). Program feasibility and acceptability was evaluated using a 20-question Likert scale (7-point) survey with 5 open response questions (Appendix B), as well as data gathered during a focus group session in which participants discussed their overall experience of the training (Appendix C). Participation in the recorded emotional shifts, survey, and focus session was optional for each participant. Human subjects activities were limited to evaluation of an educational program and, per the Institutional Review Board (IRB) were exempt.
Participants
Although demographic data were not formally collected from participants, we can provide general descriptive information about the care partners. Participants were predominantly White/Caucasian, with slightly more women than men represented. Participants’ relationships with their loved one with dementia varied and included spouses, sons, daughters, and friends.
Training Program
Three one-hour emotional resilience training sessions were held with 15 care partners of PLWD at a local support group. A manual (Appendix D) was adapted from Path2Green, an emotional resilience training model, and was provided to each participant to guide the training sessions. 11
Participants were eligible to attend any or all of the three sessions offered. Care partners attending the support group sessions were invited to participate in the research components of the program; however, those who chose not to participate in data collection were still welcome to engage fully in all session activities. Twelve participants joined the first session. Nine participants attended the second session with 6/9 attending both the first and second session and 3/9 attending the second but not the first session. Six participants joined the third session with 4/6 attending all three sessions and 2/6 attending both the first and third sessions.
Session One (n=12). Facilitators Introduced Three Tools/Techniques for Promoting Resilience
• • •
In small groups/pairs, care partners shared their strengths and discussed a time when they needed to adapt and respond to a challenging situation. Participants were guided in exploring emotional shifts by using the EGS before and after heart-focused breathing. Participants first identified how there were feeling by selecting one emotion listed on the EGS. Participants then practiced heart-focused breathing. Afterwards, participants returned to the scale to identify how they now feel by selecting an emotion on the EGS. Participants were encouraged to view their emotions in a non-judgmental way and were reminded that red emotions are not inherently bad; these emotions are normal and needed in daily life. Care partners reflected as a group about their shifts in emotions and perspective after participating in the exercise. No emotional shifts were recorded for research purposes during this session.
Analysis
Pre-post breathing exercise emotional shift recordings were evaluated. If a participant reported shifting from a red emotion to a green emotion after the breathing exercise (e.g. frustrated to satisfied), then this was considered improved positive emotion. Additionally, because the EGS is designed as a continuum, any shift towards the right such as from red to less red/closer to green (e.g. resentful to frustration) or green to more green (e.g. contentment to peaceful) would be considered improved positive emotion. Any leftward shift would be considered decreased positive emotion. No change was recorded if a participant reported the same emotion pre and post breathing exercise. Descriptive statistics were calculated for survey analysis. Free response survey questions as well as focus group transcriptions were analyzed using constant-comparative methods to identify overall themes. 12 The focus group audio recording was transcribed, and identifiable information was redacted. Two research team members reviewed the focus group transcripts and free-response survey data to identify recurring themes and patterns. Emergent themes were then categorized, and representative quotations and thematic examples were extracted.
Results
Changes in Emotions After Heart-Focused Breathing
A total of 17 emotional shifts were shared by participants. 14/17 emotional shifts (82%) reported improved positive emotion, with 3/17 (18%) reporting no change in emotion. For example, participants shifted from feeling “fear/powerless” before heart-focused breathing to “content” after the practice. Of those who did not show change, one stayed in the “red range”, one stayed “neutral”, and one stayed in the “green range” of the EGS (see Appendix D, p. 14; full results in Appendix G).
Post-Training Survey
The post-training survey (n=6) revealed that most participants strongly agreed or agreed with the utility and future use of tools and insights gained during the training. Representative statements are displayed in Figure 1 (see Appendix H for complete results). The post session survey revealed that most participants strongly agreed or agreed with the following statements.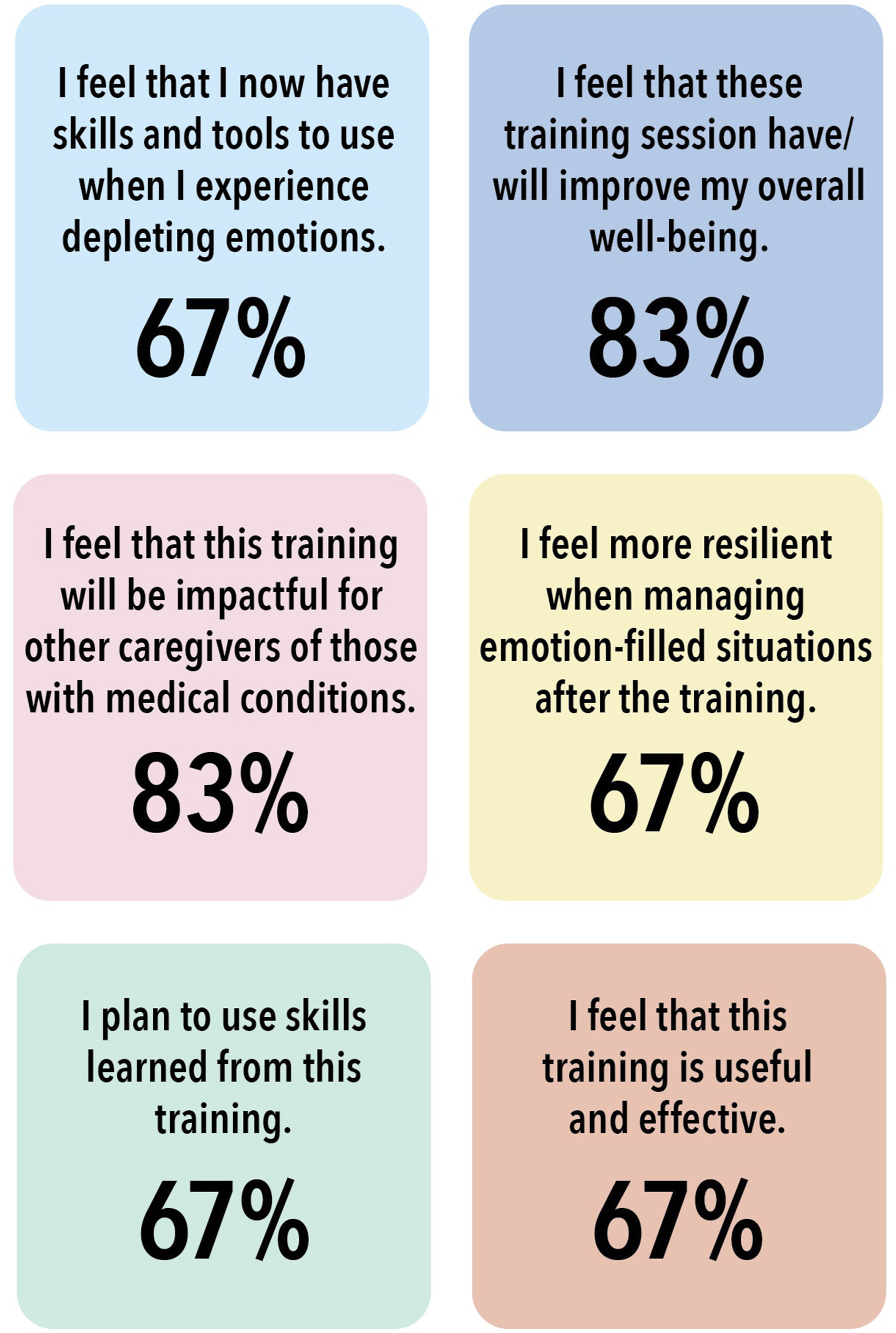
Focus Session and Free Response Survey Questions
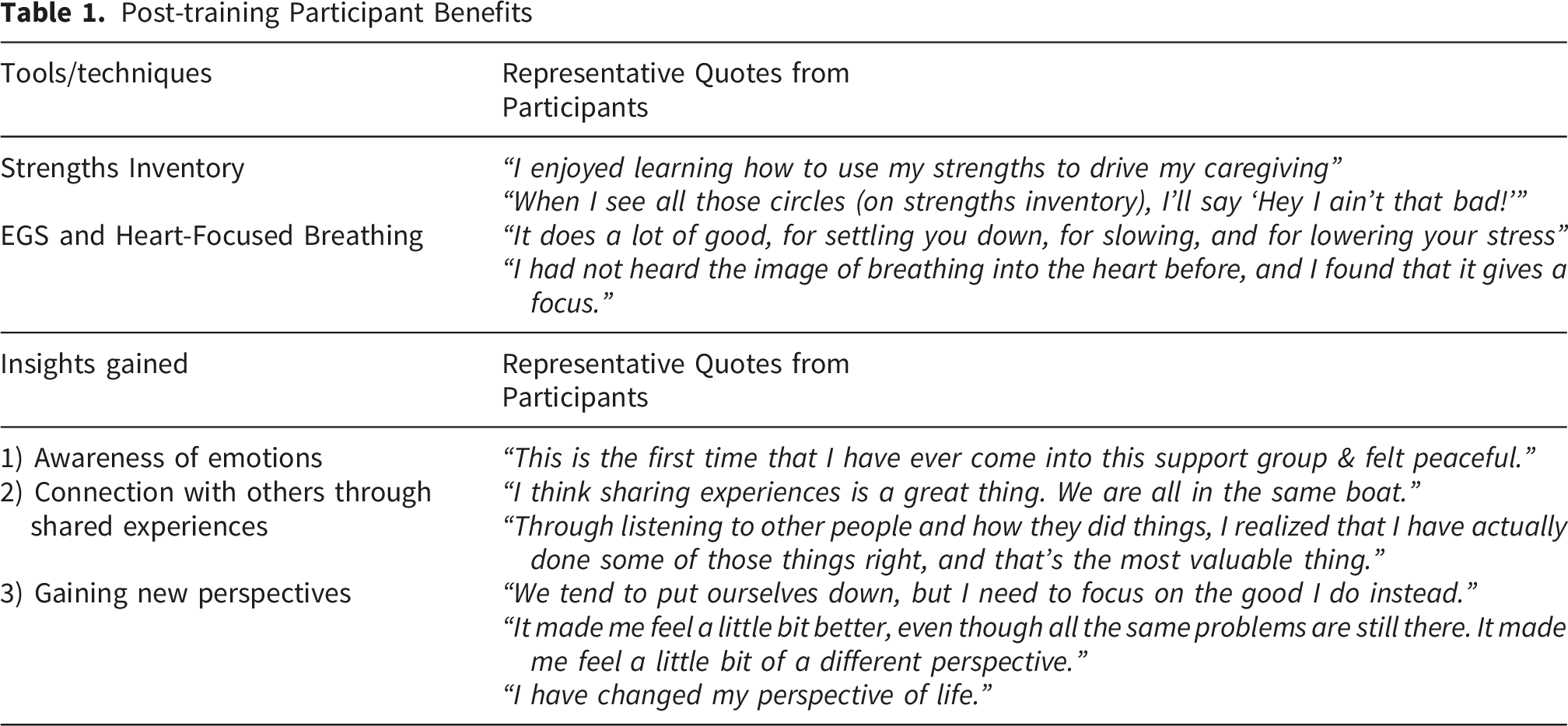
Post-training Participant Benefits
Suggested Improvements
Participants noted several suggestions for improvements, including: (1) simplifying the language to make following the program easier, (2) focusing on one micro-goal in a session, and (3) more time for group sharing experiences and strengths.
Future Impacts
Participants shared that they plan to (1) use resilience practices in future meetings, (2) start each meeting with a check in and a guided breathing exercise, (3) create one micro-goal during each meeting to accomplish before the next meeting, and (4) use specific prompts for each meeting (e.g., “What strength did you use this week?”).
Discussion
Care partners of PLWD agreed that the program was effective, useful, and easy to understand, and that they would use these skills at home. Many participants found that the program improved their ability to respond in stressful situations and that they were now more in touch with their emotions. Most care partners also agreed that they felt uplifted and encouraged after the sessions. Additionally, the majority of care partners experienced a self-reported increase in positive emotions after participating in heart-focused breathing. All of these findings together suggest potential benefits in emotional resilience.
Participants’ favorite aspects of the program included identifying their strengths, learning heart-focused breathing, and connecting with others through shared experiences. Suggested improvements included allowing more time for group discussions and simplifying the program language. The care partners ultimately chose to implement aspects of the training into their future support group sessions and believe that this training may be helpful for other care partners.
With high levels of stress, anxiety, and depression within the care partner community, it is vital that care partner burden does not continue to go unnoticed by healthcare professionals. Previous work has demonstrated that emotional resilience training can improve overall psychological well-being and increase resilience in care partners of patients with schizophrenia, but the present pilot study is one of the first to explore emotional resilience training in care partners of PLWD. 13 Further research is needed to investigate support strategies for improving overall well-being of care partners of PLWD.
Limitations
Although this pilot study sample size was small, the findings provide preliminary evidence supporting the feasibility and acceptability of this emotional resilience training modality. As care partners have busy and unpredictable schedules that limit their ability to attend support groups consistently, not all care partners were able to participate in all three sessions. Importantly, the sessions were intentionally designed as optional supportive activities in order to avoid creating additional pressure or burden for participants. However, this flexible attendance structure may have introduced self-selection bias, as participants who attended more sessions may have differed from those who attended fewer.
The small sample size also limits the generalizability of the findings. For example, only care partners of people living with dementia participated in the present study, making it unclear whether the emotional resilience training would be similarly beneficial for care partners of individuals with other chronic illnesses. In addition, the study lacked long-term follow-up data, limiting our understanding of the sustained impact of the intervention over time.
To assess engagement with emotional resilience practices outside of the sessions, participants were asked to complete an EGS tracking worksheet between meetings. However, many participants forgot to complete the worksheets, and the research team aimed to avoid imposing extensive home assignments or follow-up requirements in order to minimize additional care partner burden. As a result, the majority of data were collected during the sessions themselves and primarily reflected participants’ immediate reactions to the intervention. This limits conclusions regarding how the program may influence care partners’ daily lives beyond the training environment.
Another limitation of the present study is the potential for social desirability and interviewer bias. The primary investigator both facilitated the emotional resilience training sessions and conducted the focus groups, which may have influenced participants to provide more favorable feedback or emphasize positive experiences. Future studies may benefit from using independent facilitators or external evaluators to reduce potential response bias and improve objectivity.
To address some of these limitations, an innovative online version of this emotional resilience training for care partners of PLWD was created and can be done asynchronously based on the care partners’ schedules. 14 While the present study was an exploratory pilot study, future, larger studies should be done and may use validated measures for emotional resilience such as Connor-Davidson Resilience Scale (CD-RISC) or the Positive and Negative Affect Scale (PANAS).15,16
Conclusions
Care partners of PLWD stated that they enjoyed the emotional resilience training program and appreciated gaining tools for future challenges in caregiving. Participants self-reported an increase in positive emotion after participating in emotional resilience techniques and found it useful to identify their personal strengths. Although further research in this area is needed, this pilot study suggests that emotional resilience training may be a helpful support strategy for care partners of PLWD.
Declarations
Permission was obtained to reproduce and reference the Path2Green/MBN Systems materials included in Appendix D and the referenced online training program. The authors affirm that they have no financial, professional, institutional, employment, advisory, ownership, intellectual-property, or other conflict of interest relationships with Path2Green, MBN Systems, the CARE Center, or the online training program referenced in this manuscript. The inclusion of these materials is solely for scholarly and educational purposes relevant to the objectives of this work.
Supplemental Material
Supplemental Material - Emotional Resilience Training to Support Care Partners of People Living with Dementia: A Pilot Study
Supplemental Material for Emotional Resilience Training to Support Care Partners of People Living with Dementia: A Pilot Study by Delaney Lockwood, Amy Baldwin, Sarah Saint Hamilton, Casey Bassett, Janette R. Hill and Cathy Snapp in Journal of Patient Experience.
Footnotes
Acknowledgement
Many thanks to the Arnold P. Gold Foundation for supporting this project through the 2024 Student Summer Fellowship Program.
ORCID iDs
Ethical Considerations
Human subjects activities were limited to evaluation of an educational program and, per the University of Georgia Institutional Review Board were exempt. Informed consent was not required for this pilot study.
Author Contributions
DL: Conceptualization and design of the study. Acquisition, analysis, and interpretation of data. Drafting and revising manuscript. AB: Drafting and revising manuscript. SSH: Conceptualization and design of the study. Drafting and revising manuscript. CB: Drafting and revising manuscript. JRH: Drafting and revising manuscript. CS: Conceptualization and design of the study. Drafting and revising manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Arnold P. Gold Foundation, Grant ID#: SS-24-002.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Full data is available in Appendix.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.