
Abstract
Osteoarthritis (OA) affects millions of Canadians with substantial healthcare costs, yet education and exercise can improve outcomes. This study explored the perceived benefits, facilitators, and barriers influencing perceived access and adherence to an 8-week physiotherapist-supervised exercise and education program in a private clinic. Adults with hip and/or knee OA enrolled in the program were invited to complete a cross-sectional online survey. Descriptive statistics and qualitative content analyses were used to describe participant demographics, clinical features, and perceptions. Of 102 participants, 61 completed the survey (60% response rate). Perceived benefits identified by participants included physical improvements, socialization, increased confidence, expert support, and improved self-efficacy. Perceived facilitators supporting adherence were physical ability, financial support, transportation, and provider expertise. While most participants reported no major barriers, some noted financial constraints, physical limitations, inconvenient class times, and work demands. A group-based hip and knee OA program delivered by physiotherapists can provide substantial perceived physical, psychological, and social benefits, though self-reported adherence may be influenced by financial, physical, and social factors.
Plain Language Summary
Keywords
Introduction
Osteoarthritis (OA) affects over 4.6 million Canadians, with healthcare costs exceeding $1.4 billion annually.1,2 Saskatchewan residents face some of the longest wait times in Canada for total joint arthroplasty (TJA), 3 leaving many without timely surgical or non-surgical care. Conservative approaches including education and exercise are effective for moderate to severe OA, reducing pain and improving function and quality of life. 4 Without conservative care, individuals may adopt compensatory movement patterns, worsening joint degeneration and mobility loss. 5 By helping individuals with OA maintain physical abilities, improve movement strategies, and manage pain, exercise can lead to better daily function and post-surgical outcomes. 6 When delivered through physiotherapist-led programs that combine exercise and education, this approach has proven effective for those with mild to severe hip or knee OA. 7 While the clinical efficacy of these conservative approaches is well-established, there is a critical need to understand the patient-reported factors that translate clinical guidelines into sustainable, everyday management.
This study aims to identify the perceived benefits of a physiotherapist-led exercise and education program designed for individuals with hip or knee OA, and how participant demographics and perceived facilitators and barriers may be associated with perceived program access and self-reported adherence. The objectives of this study were to: 1) describe the sociodemographic and clinical participant features, and 2) identify and categorize perceived benefits of program participation and the perceived facilitators and barriers which impact adherence. By utilizing a patient-oriented approach to identify perceived benefits, facilitators, and barriers, this research advances patient-centered care by aligning research priorities with lived experiences, providing insight into the drivers of successful long-term self-reported adherence to conservative care. Understanding these factors could inform future program development and delivery, helping to guide the implementation of similar programs by identifying strategies to enhance perceived accessibility and engagement across diverse populations.
Methods
Study Design
This study adheres to the STROBE (STrengthening the Reporting of OBservational studies in Epidemiology) cross-sectional reporting guidelines 8 and evaluated participant experiences in an OA exercise and education program. The outcomes of interest were participant-perceived benefit from the program and perceived facilitators and barriers to program access and self-reported adherence. To ensure these outcomes aligned with the priorities of individuals with OA, this study utilized a patient-oriented approach, which integrates patients as collaborators with clinicians and researchers to produce evidence that directly improves care. 9 Three patient partners (i.e. program participants with lived experience of hip or knee OA) contributed to survey development, interpretation of findings, and manuscript preparation. In this study, ‘Access’ was defined as the participant’s perceived ability to enter and participate in the program, whereas ‘Adherence’ was qualitatively measured and defined by the self-reported participation duration and subjective identification of factors that influenced continued engagement, rather than objective attendance logs.
Program Participants and Setting
Study participants were individuals living with OA who were enrolled in the OA program. The OA program is a physiotherapist-led initiative tailored for individuals with hip or knee OA and delivered in a private-practice setting. Using an evidence-based approach, physical therapists deliver twice-weekly group classes over eight weeks to support OA management. 10 The program emphasizes education, neuromuscular and strength development, functional movement training, and ongoing progress monitoring to help individuals reduce symptoms and restore function.
Eligibility Criteria
Inclusion criteria consisted of current OA program participants aged 18 or older with self-reported hip or knee OA (i.e. diagnosis was self-reported and not verified through imaging or clinical assessment).
Data Collection
Description of Study Variables
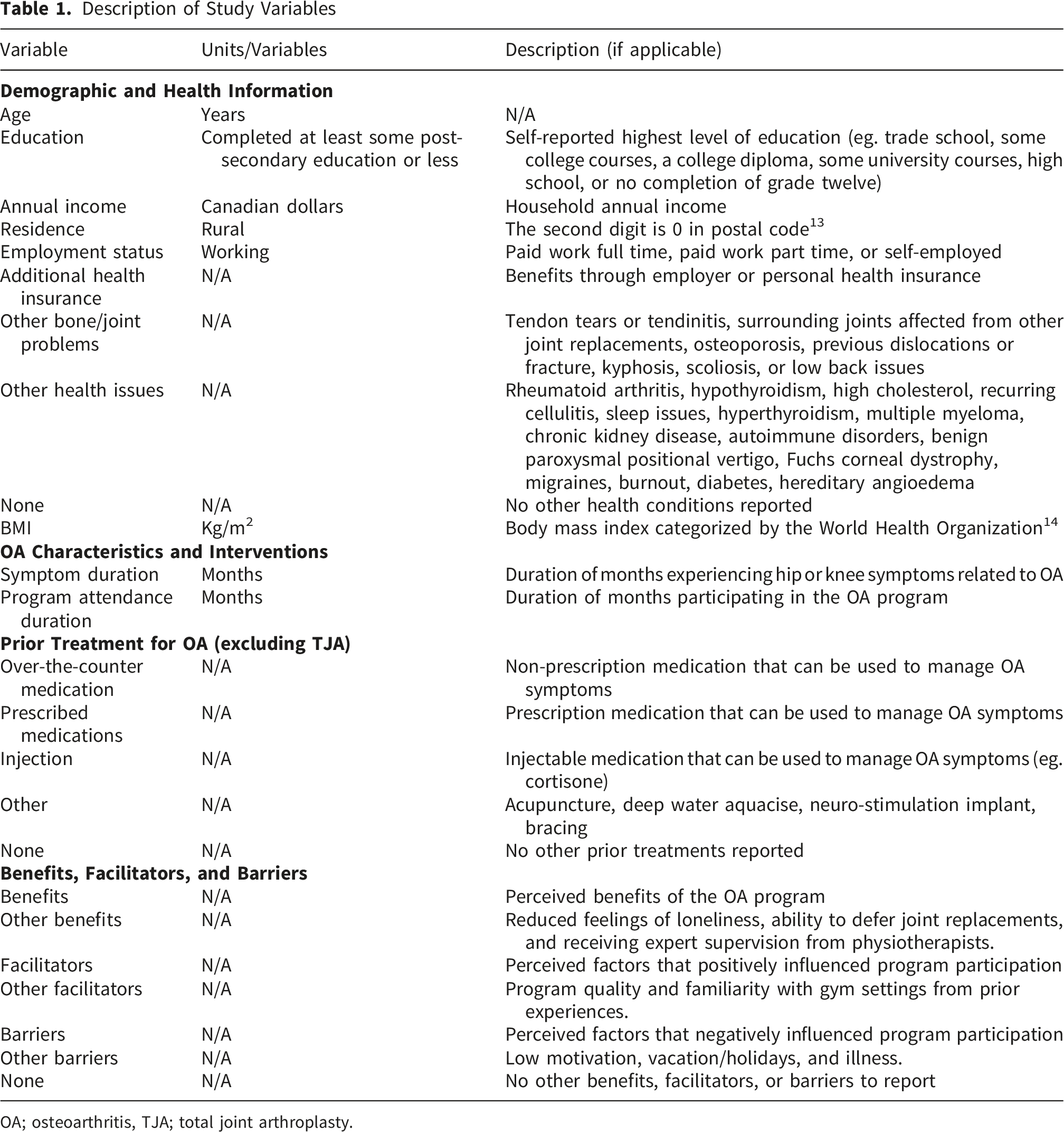
OA; osteoarthritis, TJA; total joint arthroplasty.
Data Analysis
Descriptive statistics were used to summarize participant demographics, clinical characteristics, and program-related variables. Frequencies and percentages were reported for categorical variables. Quantitative analysis was conducted by a single reviewer using Microsoft Excel to compute summary statistics. No inferential or hypothesis-driven statistical tests were performed due to the descriptive nature of the study. Responses to open-ended questions were analysed using NVivo 15 qualitative analysis software. Two researchers independently conducted inductive thematic coding to identify recurring patterns in the data. To ensure rigor, researchers met to compare codes and resolved any disagreements through consensus-based discussion. This collaboration aimed to minimize individual interpretive bias and ensure the final themes accurately represented the participants lived experience.
Ethical Considerations
The study was approved by the University of Saskatchewan Behavioural Research Ethics Board (ID 4102), Saskatchewan, Canada, and was conducted in accordance with relevant national ethical guidelines. All participants provided informed consent before completing the survey.
Results
Demographic, Health Characteristics, Osteoarthritis Status, and Prior Treatments Among Participants
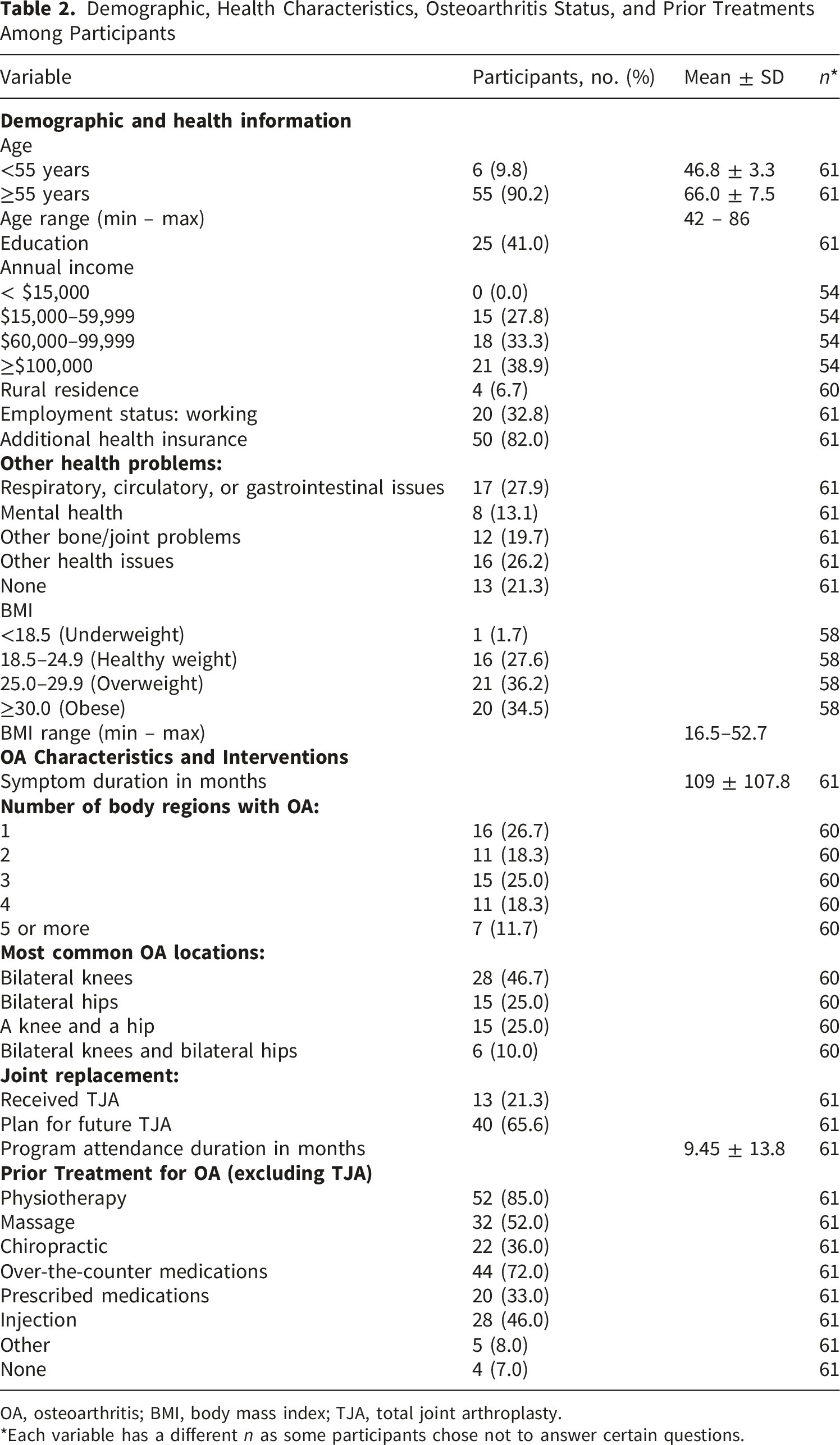
OA, osteoarthritis; BMI, body mass index; TJA, total joint arthroplasty.
*Each variable has a different n as some participants chose not to answer certain questions.
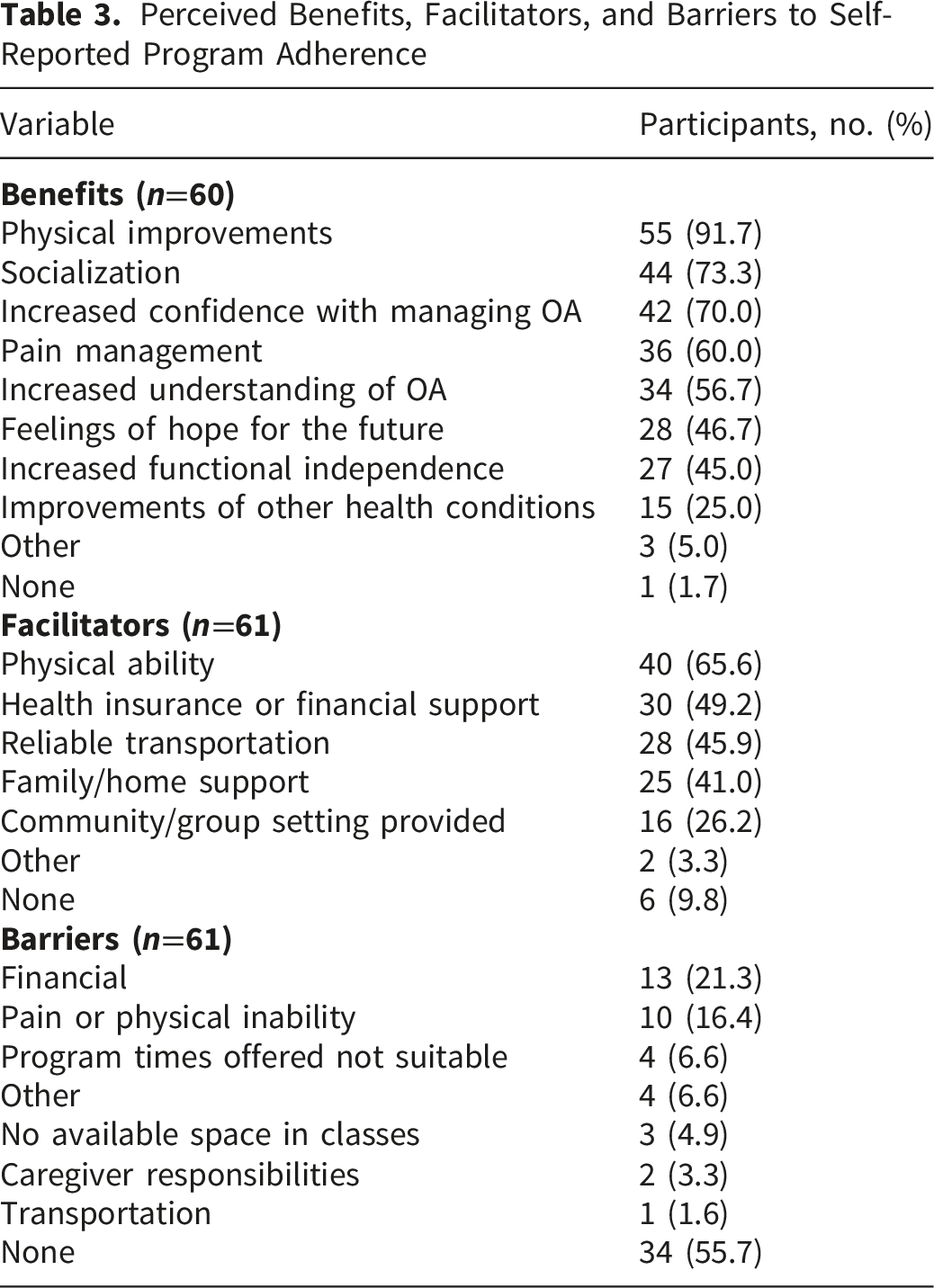
Perceived Benefits, Facilitators, and Barriers to Self-Reported Program Adherence
Participant-Reported Benefits, Facilitators, and Barriers by Theme (Qualitative Quotes)
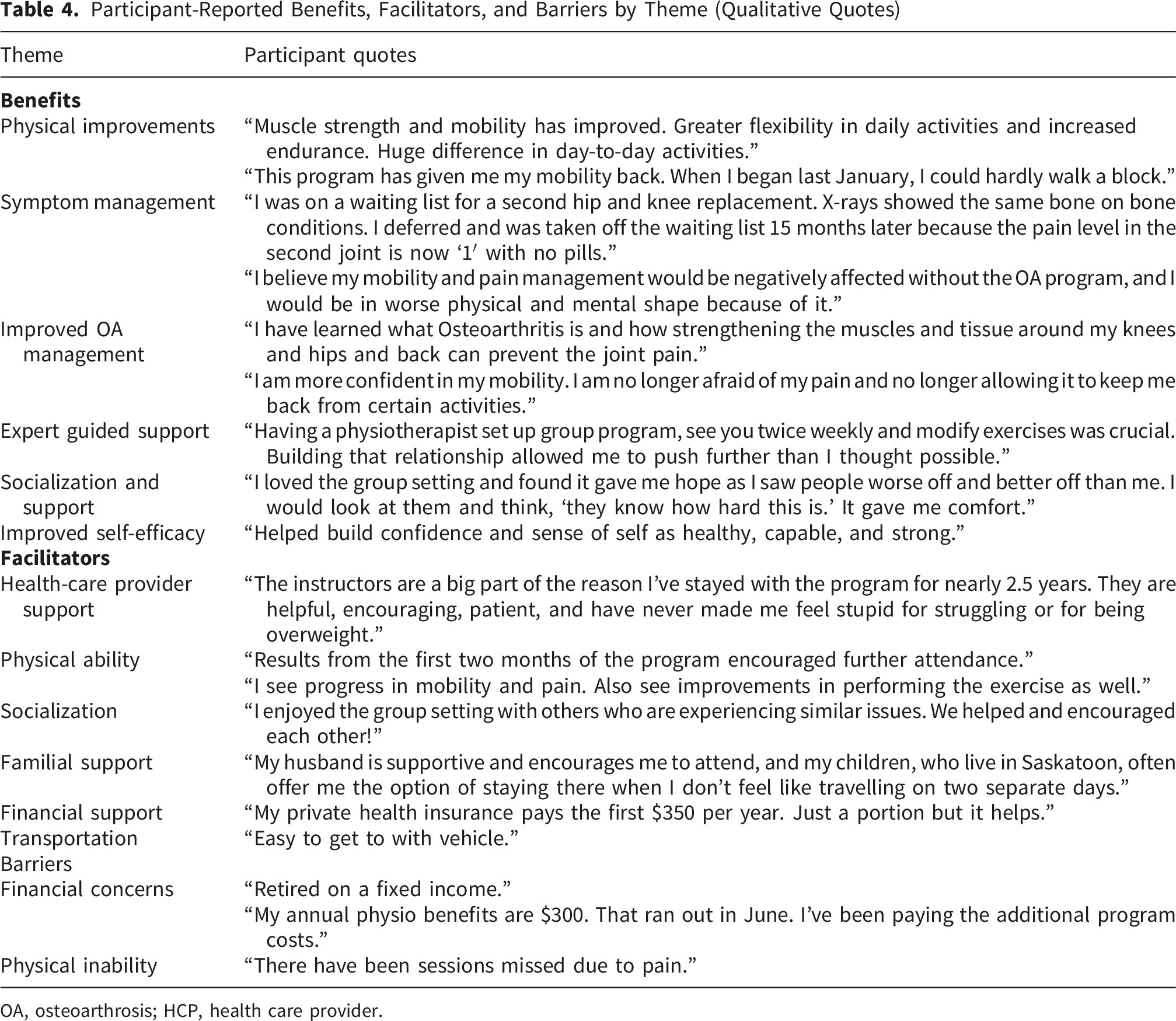
OA, osteoarthrosis; HCP, health care provider.
Most participants (77%) were women aged over 55, with 71% classified as overweight or obese. Approximately three-quarters reported a household income above $60,000 and had additional health insurance. Bilateral knee OA (n = 28, 47%) was the most frequently reported condition, and comorbidities were common. Many participants had previously received physiotherapy or over-the-counter medications as non-surgical treatments. Summary statistics and categorical distributions are presented in Table 2.
Thematic Definitions
Analysis of the open-ended survey responses revealed several themes regarding participant experiences. To ensure a shared understanding of these findings, the themes are defined based on the core experiences reported by participants.
Perceived benefits were defined by five key themes: Physical improvements (reported gains in mobility, strength, or function); Symptom management (reductions in pain or swelling); Improved OA management (the acquisition of disease-control strategies); Expert-guided support (the value of professional physiotherapist oversight regarding education and exercise); Socialization and support (the motivational impact of peer engagement in a group setting); and Improved self-efficacy (the increase in confidence toward independent condition management).
Perceived facilitators to adherence were defined by four key themes: Support systems (the encouraging influence of healthcare providers, family members, or peers); Physical ability (a baseline level of health that permitted successful program engagement); Socialization (the desire for community or group interaction and shared experiences); and Practical determinants (the availability of enabling resources such as reliable transportation and financial means).
Perceived barriers to adherence were characterized by two key themes: Financial concerns (the perceived economic burden of program costs or a lack of adequate insurance coverage); and Physical inability (health-related limitations, such as acute symptom flare-ups or co-morbidities).
Perceived Benefits, Facilitators, and Barriers
Participants identified a range of perceived benefits from the program, with the most frequently reported being physical improvements (91.7%), social connection (73.3%), and increased confidence in managing OA (70.0%) (Table 3). As one participant stated, “Muscle strength and mobility has improved. Huge difference in day-to-day activities.” Another shared, “This program has given me my mobility back.” Pain management (60.0%) and improved understanding of OA (56.7%) were also common benefits. One participant noted, “The program has been beneficial in reducing arthritis pain and inflammation in my knees,” while another said, “I am no longer afraid of my pain and no longer allowing it to keep me back from certain activities.” Participants frequently highlighted the importance of expert guidance from physiotherapists. One noted, “Building that relationship allowed me to push further than I thought possible,” and another described the “excellent, tailored instruction for my specific mobility and strength issues.”
Beyond a benefit, social interaction emerged as a key perceived facilitator of self-reported adherence, with 26.2% of participants citing the group setting as supportive (Table 3). Participants valued the peer support and shared experience: “I enjoyed the group setting with others who are experiencing similar issues.” and “I loved the group setting and found it gave me hope.” Other commonly reported perceived facilitators included physical ability (65.6%), financial support (49.2%), and access to transportation (45.9%). Physical progress reinforced motivation for many, as one participant explained, “Results from the first two months of the program encouraged further attendance.” Support from healthcare providers was also critical: “Having a physiotherapist ensure I was performing the exercises correctly gave me the confidence to continue.”
While 56% of participants reported no barriers to participation, others identified several perceived challenges, including financial constraints (21.3%), physical limitations (16.4%), inconvenient class times (6.6%), and competing responsibilities (Table 3). Financial concerns were common, with one participant stating, “I’ve maxed out my private insurance coverage,” and another noted, “My annual physio benefits is $300. That ran out in June. I’ve been paying the additional program costs.” Physical symptoms also interfered with attendance: “There have been sessions missed due to pain.” Others noted life demands: “Job demands caused me to miss some classes.” Among those who did report difficulties, financial constraints and physical symptoms were the most frequently cited factors perceived to influence self-reported attendance.
Discussion
This cross-sectional survey of 61 participants of a physiotherapist-led group-based education and exercise osteoarthritis program identified participant sociodemographic and clinical characteristics, as well as perceived benefits, facilitators, and barriers to perceived access and self-reported program adherence. Participants were predominantly women (77%) and older adults (mean age: 66.0 ± 7.5 years), with most having a BMI in the overweight or obese range. The majority reported annual incomes above $60,000, had supplementary health insurance, and lived in urban areas; one-third were employed. Bilateral knee OA was the most reported condition, and many participants also reported experiencing comorbidities. Participants reported a range of benefits from the program, most notably physical improvements, socialization, and increased confidence in managing osteoarthritis. Key perceived facilitators included physical ability, financial support or insurance, and reliable transportation. Perceived barriers were less frequently reported, but included financial challenges, pain or physical limitations, and inconvenient program times.
Our participant’s demographics, predominantly female and averaging 66 years of age, closely resemble those in the GLA:D® Canada program. 16 Our cohort of primarily urban, insured adults also shares key characteristics with participants in the Better Knee, Better Me™ trial, which involved adults with knee OA and elevated BMI. 17 In contrast, the ESCAPE-pain study enrolled a more socioeconomically diverse population from public healthcare settings, 18 whereas our sample was drawn from a fee-based clinic. This distinction is important, as our largely urban sample may not reflect the significant access challenges, such as substantially longer travel times, often faced by rural Canadians with OA. 19 The limited rural representation in our cohort, where 56% of respondents reported no participation barriers, suggests the program’s urban location, participant’s higher income, and insurance coverage helped mitigate common perceived access challenges. Although clinically similar to the broader OA population, the sample’s socioeconomic advantages limit the findings’ generalizability to those facing greater financial or geographic barriers.
The perceived benefits reported by participants emphasize the holistic impact of engaging in a structured education and exercise program for osteoarthritis, with reported benefits encompassing physical, social, and emotional domains. Perceived physical improvements include increased strength and mobility, improved function with daily activities, and reduced pain. These outcomes are relevant considering individuals with OA commonly experience greater pain, functional limitations, and chronic health conditions compared to the general population, with many being overweight, obese, or physically inactive. 20 Many individuals with OA enter a cycle where pain leads to inactivity, resulting in further declines in mobility and function, which in turn exacerbates symptoms and sustains inactivity.21,22 Structured exercise programs are a key component of non-surgical OA management, 22 offering a pathway to disrupt this cycle and support improved physical function.
In addition to self-reported physical improvements, participants described psychosocial benefits. Similar studies report that individuals in group-based exercise therapy value the support and connection, which helps reduce isolation and foster hope. 23 Improved understanding of OA and physical progress can contribute to greater self-efficacy, 23 highlighting the need to address psychosocial factors alongside physical outcomes. Our findings support this evidence, with participants highlighting a range of psychosocial benefits that influenced their engagement in the program.
Effective OA management requires collaborative patient–healthcare provider relationships, adequate disease education, and active patient engagement. Psychosocial factors such as pain catastrophizing, health literacy, and self-efficacy significantly impact patient compliance and adherence to interventions. 24 However, fewer than 25% of individuals receive sufficient education on OA diagnosis, management, and disease progression,24-27 limiting their capacity for self-management. Disease-specific education and consistent feedback from professionals has shown to manage expectations, identify progression risk factors, and support adherence. 6 Our findings support this evidence by demonstrating the value of patient-centred care within a physiotherapist-led OA program, reinforcing the importance of personalized, clinician-led care for improving adherence and outcomes. The current study identified expert supervision and guidance as key benefits, with participants expressing greater confidence in challenging their physical limits after receiving education on the purpose and outcomes of exercise. This highlights the need for healthcare providers to deliver tailored, disease-specific education that reflects patients’ health literacy and evolving needs.24,28
Several common perceived facilitators and barriers emerged from participant responses. Financial support was viewed as facilitating self-reported program adherence, while financial concerns were a perceived barrier. Although many participants had additional health insurance, some noted it only covered one or two sessions, requiring them to pay for continued care. These findings align with previous research identifying private health insurance as an enabler of access to non-surgical treatments such as physical therapy, and even individuals with insurance face significant financial barriers due to limited coverage and high out-of-pocket costs. 29 Furthermore, financial strain can deter ongoing participation and raises concerns about the sustainability of self-funded treatment. 29 These shared perspectives reinforce the need to address financial accessibility in program design to support long-term engagement with non-surgical OA interventions.
Engagement in OA exercise programs is influenced by personal and social factors. Prior research has identified personal beliefs about exercise outcomes and capabilities as common barriers, while structured environments that offer reinforcement and support act as key facilitators. 30 Our findings align with this, as participants frequently reported physical improvements that motivated continued attendance, highlighting the value of structured programming. Structured interventions can improve symptom control, self-efficacy, and reduce fear of movement in individuals with musculoskeletal (MSK) conditions. 31 Similarly, our participants described gaining confidence in their physical abilities and a greater sense of control over their OA symptoms. Program engagement is critical to success, and previous studies show that lower adherence to physical therapist-led OA interventions is associated with poorer outcomes, 23 while supervised, structured programs that incorporate monitoring, feedback, and education have been shown to improve adherence.32,33 Participants in our study echoed these findings, highlighting expert support and feedback as central to their experience and naming expert guidance as the most reported qualitative benefit. While cost, location, and wait times have been cited as barriers to accessing physiotherapy in other MSK populations, 31 our participants primarily reported financial strain, with fewer geographic concerns, likely due to the program’s urban setting. Notably, 56 % of participants reported no perceived barriers, highlighting the role of strong client–therapist relationships and supportive environments in supporting perceived engagement with non-surgical interventions.
Future program planning should consider delivery models that address cost and perceived service accessibility. Group-based programs offer a cost-effective alternative to private individual physiotherapy, with evidence showing comparable outcomes in pain reduction, functional improvement, and patient satisfaction among individuals with musculoskeletal disorders. 34 In addition to potential cost savings and reduced access to care wait times, group formats have been shown to promote socialization, which can enhance motivation and adherence.35,36 Our findings align with this evidence, as participants frequently cited the affordability, peer support, and motivating group environment as key perceived facilitators of engagement in the program.
While this study highlights the benefits for those enrolled, the identified barriers provide insight into populations likely excluded from this model. The theme of financial concerns suggests that individuals without extended health insurance or sufficient disposable income may be unable to access private-practice, physiotherapist-led programs. Consequently, this model may primarily serve higher-resource populations, potentially widening the gap for those of lower socioeconomic status who rely on publicly funded care.3,31 Furthermore, the barrier of physical inability, characterized by acute flare-ups and comorbidities, indicates that patients with the highest disease severity or complex medical needs may be excluded from a standardized group exercise format. 23 Since the program was delivered in a private-practice setting, geographic location may have acted as a perceived barrier. As noted in the facilitators, participants highlighted the importance of reliable transportation, suggesting those in rural areas may perceive significant barriers to access due to a lack of accessible transit options.19,31 By acknowledging these perceived barriers, it becomes clear that while the program is effective for those who can attend, further research is needed to adapt this model for more marginalized or medically complex populations.16,29
Strengths and Limitations
Several measures were taken to minimize potential bias in the study and enhance the reliability of findings. To reduce selection bias, all eligible participants were invited to complete the survey, which was administered anonymously and independently to limit social desirability bias. Data were collected during active program participation to reduce recall bias, and standardized, structured questions were used to improve consistency. Qualitative responses were independently coded by two researchers using NVivo to enhance coding reliability and limit interpretive bias. The survey achieved a 60% response rate—exceeding the 52.7% average found across 490 published cross-sectional studies using individual-level questionnaires, 37 aligning with the ≈60% mean for mail surveys in medical journals, 38 and meeting the ≥60% threshold recommended for program evaluation research. 39 This strong response rate reduces the risk of non-response bias while enhancing the precision and generalizability of the descriptive findings within the sampled population. 40
Several limitations should be interpreted with caution given the descriptive nature of the study. The cross-sectional design limits the ability to draw causal inferences, as data were collected at a single time point; consequently, the predominance of reported perceived benefits over barriers is likely influenced by positivity and self-selection biases. Due to the study design, participants who found the program ineffective or had lower attendance due to barriers were less likely to be captured in the sample. This implies that the high satisfaction and adherence levels reported here likely reflect a ‘best-case’ scenario among successful participants rather than the experience of every individual who was enrolled. These biases suggest that while the program can produce substantial benefits, these results should be interpreted as the perceived potential of the program under optimal conditions (e.g., higher income, urban access, and high motivation). Readers should exercise caution when applying these findings to broader public health settings where the ‘non-responder’ profile, those with lower income or higher disease severity, is more prevalent. 29
Additionally, because demographic and clinical data were not available for the 40% of invited individuals who did not complete the survey, the extent of non-responder bias cannot be fully determined. Although our response rate meets established thresholds for program evaluation research, 39 self-reported data remain subject to recall and social desirability biases, which could further overestimate favorable outcomes. Furthermore, the reliance on self-reported OA diagnosis introduces the risk of misclassification, as participants’ symptoms were not verified through clinical assessment or imaging. This may affect the generalizability of the results, as the cohort could potentially include individuals with non-OA joint pain or inflammatory conditions whose experiences with exercise may differ from those with confirmed osteoarthritis. We also did not correlate survey responses with objective attendance records or completion rates; consequently, ‘adherence’ reflects the participants’ perspective of their consistency and longevity in the program rather than a verified clinical metric. Given the private urban setting and the high proportion of participants with additional health insurance, findings from the small sample size may not generalize to rural populations or individuals without insurance. 31 Rural residents often face distinct barriers, such a longer travel times, 19 which were not fully captured in this study. Some variables, such as income, residence, and BMI, had missing data, which may limit the representativeness of the reported participant characteristics. Further research using longitudinal designs and comparative analyses is needed to clarify the extent to which these findings represent the broader population.
Conclusions
Multiple factors may influence perceived access to osteoarthritis exercise programs, including demographic, physical, and psychosocial determinants. Participants in the OA program reported perceived benefits that addressed physical, social, and emotional needs, reinforcing the importance of a biopsychosocial approach. Program accessibility may be enhanced by financial assistance and group-based delivery models led by qualified professionals. Self-reported adherence was perceived to be promoted by physiotherapists who foster self-efficacy through education and feedback. This study supports existing evidence that expert guidance and social support are key to participant engagement and improving outcomes in OA programs. However, given the descriptive design and sociodemographic profile of participants, findings should be interpreted cautiously and may not generalize to underserved populations. Future studies should explore long-term outcomes and applicability across more diverse settings to inform broader implementation.
Footnotes
Acknowledgments
The authors wish to thank the program participants for sharing their valuable experiences. We also acknowledge our patient partners, Pat Danyluk, Dawna Rose, and Ken Wilkinson, for their crucial contributions to the survey development, interpretation of findings, and preparation of this manuscript. We also extend our gratitude to the staff at the participating clinic for their support and assistance with participant engagement. During the preparation of this manuscript, the author(s) used Google Gemini to refine language and ensure adherence to the word count. All authors reviewed, edited, and take full responsibility for the final content of the manuscript.
Ethical Considerations
Ethical approval was approved by The University of Saskatchewan Behavioural Research Ethics Board (ID 4102), Saskatchewan, Canada. All procedures were conducted in accordance with the Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans TCPS 2 (2022).
Consent to Participate
Written informed consent was obtained from all participants for their anonymized information to be published in this article.
Consent for Publication
During the preparation of this work the author NW used Google Gemini to adjust the word count of the manuscript. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of this publication.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was funded by the College of Medicine, University of Saskatchewan, through the School of Rehabilitation Science MPT Research Project 2022-2023 and awarded to NW. This funding supports student-led research projects conducted under the supervision of faculty members within the School of Rehabilitation Science.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, Nikole Watson, upon reasonable request.
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans TCPS 2 (2022).
Appendix
Additional Participant-Reported Benefits, Facilitators, and Barriers by Theme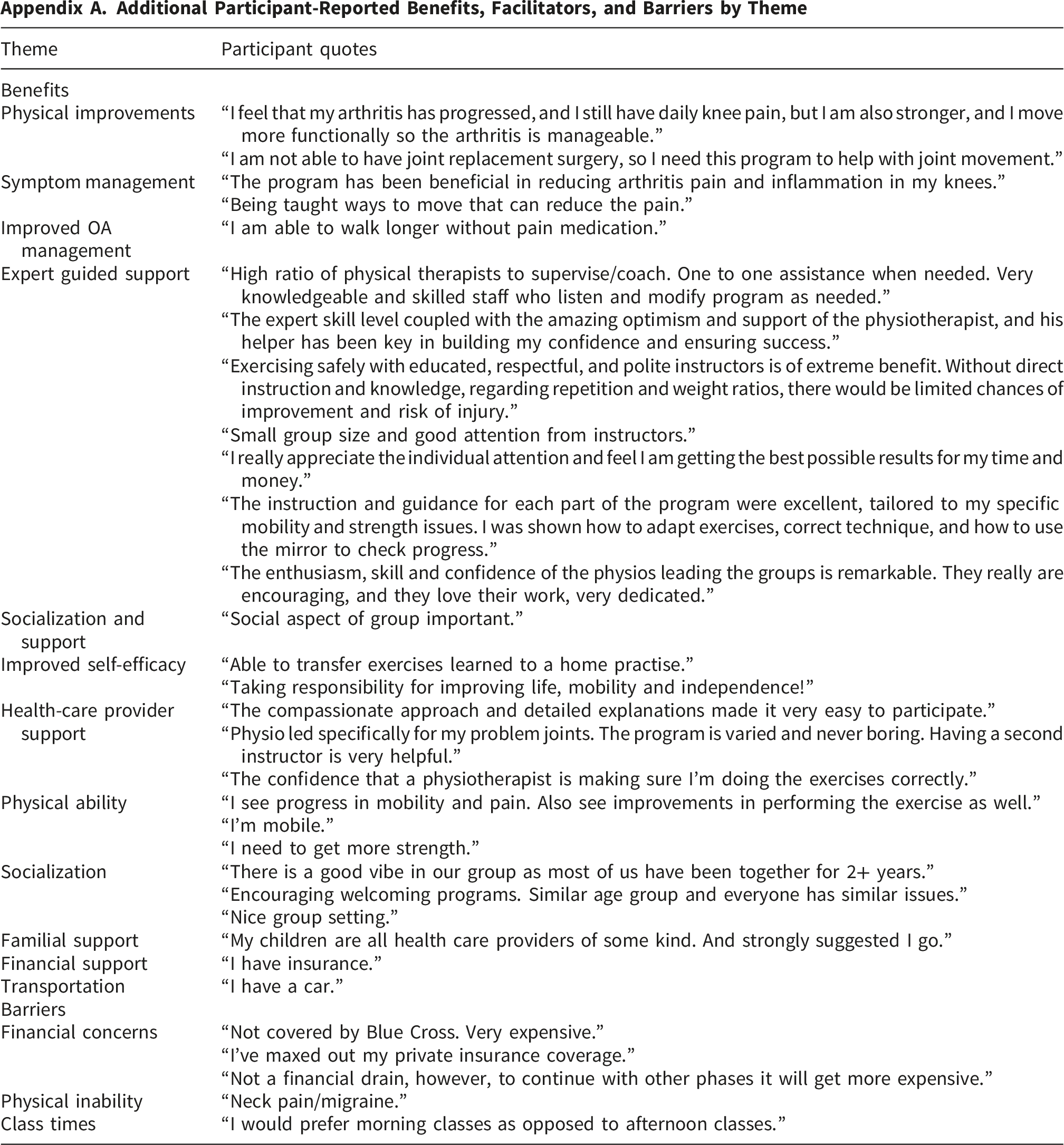
Theme
Participant quotes
Benefits
Physical improvements
“I feel that my arthritis has progressed, and I still have daily knee pain, but I am also stronger, and I move more functionally so the arthritis is manageable.”
“I am not able to have joint replacement surgery, so I need this program to help with joint movement.”
Symptom management
“The program has been beneficial in reducing arthritis pain and inflammation in my knees.”
“Being taught ways to move that can reduce the pain.”
Improved OA management
“I am able to walk longer without pain medication.”
Expert guided support
“High ratio of physical therapists to supervise/coach. One to one assistance when needed. Very knowledgeable and skilled staff who listen and modify program as needed.”
“The expert skill level coupled with the amazing optimism and support of the physiotherapist, and his helper has been key in building my confidence and ensuring success.”
“Exercising safely with educated, respectful, and polite instructors is of extreme benefit. Without direct instruction and knowledge, regarding repetition and weight ratios, there would be limited chances of improvement and risk of injury.”
“Small group size and good attention from instructors.”
“I really appreciate the individual attention and feel I am getting the best possible results for my time and money.”
“The instruction and guidance for each part of the program were excellent, tailored to my specific mobility and strength issues. I was shown how to adapt exercises, correct technique, and how to use the mirror to check progress.”
“The enthusiasm, skill and confidence of the physios leading the groups is remarkable. They really are encouraging, and they love their work, very dedicated.”
Socialization and support
“Social aspect of group important.”
Improved self-efficacy
“Able to transfer exercises learned to a home practise.”
“Taking responsibility for improving life, mobility and independence!”
Health-care provider support
“The compassionate approach and detailed explanations made it very easy to participate.”
“Physio led specifically for my problem joints. The program is varied and never boring. Having a second instructor is very helpful.”
“The confidence that a physiotherapist is making sure I’m doing the exercises correctly.”
Physical ability
“I see progress in mobility and pain. Also see improvements in performing the exercise as well.”
“I’m mobile.”
“I need to get more strength.”
Socialization
“There is a good vibe in our group as most of us have been together for 2+ years.”
“Encouraging welcoming programs. Similar age group and everyone has similar issues.”
“Nice group setting.”
Familial support
“My children are all health care providers of some kind. And strongly suggested I go.”
Financial support
“I have insurance.”
Transportation
“I have a car.”
Barriers
Financial concerns
“Not covered by Blue Cross. Very expensive.”
“I’ve maxed out my private insurance coverage.”
“Not a financial drain, however, to continue with other phases it will get more expensive.”
Physical inability
“Neck pain/migraine.”
Class times
“I would prefer morning classes as opposed to afternoon classes.”