
Abstract
This study evaluated patient experience in an Australian inpatient rehabilitation cohort in a tertiary hospital. Fifty-one consecutive patients admitted to an inpatient rehabilitation unit were recruited to evaluate their experience using the Australian Modified Client-Centred Rehabilitation Questionnaire (AM-CCRQ) across seven domains: decision-making, education, outcome evaluation, family involvement, emotional support, physical comfort, and continuity/coordination of care. Participants’ functional outcomes before and after rehabilitation were evaluated using validated Clinical Functioning Information Tool (ClinFIT) and Functional Independence Measure (FIM) tools. The median age of participants was 68 years (range 27-91), with the majority being female (54.9%). The most common conditions were orthopaedic (29.4%) and stroke (23.5%), with most participants reporting at least one issue in ClinFIT categories. Emotional support, decision-making and education AM-CCRQ domains received the highest positive ratings, while family involvement domain was rated the ‘lowest.’ The participants demonstrated significant functional improvement at discharge across ClinFIT categories and FIM subscales (p <0.001 for all). The AM-CCRQ can be a useful system-level indicator of quality and safety when used in conjunction with routine rehabilitation outcome tools.
Introduction
Patient-centred care is an emerging trend in the provision of safe and effective quality healthcare. It recognises the need for healthcare providers to understand the individual characteristics, preferences, values, needs and psychosocial contexts of patients, and to be able to respond flexibly to these needs and preferences with the delivery of responsive interventions. 1 Evaluating patient experience is an important component of patient-centred care, and is considered a more objective indicator than patient satisfaction, with lower susceptibility to ceiling effects.2-6 It encompasses aspects such as patient engagement, participation in decision-making, patient autonomy, therapeutic alliance, emotional support and continuity of care.7,8 Across a range of healthcare settings and socio-demographic groups, patient experience has been consistently associated with improved quality and safety of healthcare. 9 These associations extend to greater patient satisfaction, improved treatment adherence, reduced length of hospital stay, reduced readmission rates, fewer adverse outcomes, and reduced associated hospital costs.10-15
With an aging population, a growing number of people are living with chronic disabilities that require rehabilitation care, aimed at reducing symptom burden, activity limitations and participation restrictions, and improving their quality of life. Central to this process is the need for coordinated, longitudinal input from multidisciplinary health professionals, alongside recognition of complex, multidimensional patient and staff relationships underpinning shared goal-setting and discharge planning to the community, as well as effective communication to promote patient self-efficacy and self-management.16-18 These factors make rehabilitation care a ‘complex intervention’ and distinctive from acute hospital care.
Therefore, the patient-reported experience measurement (PREM) tools developed for acute care settings may not fully capture the domains relevant to rehabilitation context. The Australian Modified Client-Centred Rehabilitation Questionnaire (AM-CCRQ) survey tool (Supplementary Material 1) is a validated and widely used tool developed to address this gap, evaluating patient experience across seven domains: participation in decision-making and goal-setting, client-centred education, evaluation of outcomes from the client’s perspective, family involvement, emotional support, coordination and continuity of care, and physical comfort. 19 This integration of rehabilitation-specific domains allows contextualisation of patient experience within the clinical realities of rehabilitation care. Within rehabilitation settings, evidence suggests that positive patient experience is associated with increased adherence to treatment, with beneficial effects for participation and functional outcomes.9,20 Capturing patient feedback on their experience in rehabilitation settings is particularly important,21-24 as it allows identification of key areas for action, such as increased patient inclusion, improved discharge planning pathways, increased staff training, and improved quality of information provision to patients and families regarding their care and treatment. 25
Despite a growing body of literature on tools to measure patient experience,3,26-30 there remains limited rehabilitation-specific patient experience data.31,32 Furthermore, PREMs are typically interpreted in isolation from objective measures of functioning and clinical complexity, which may limit their interpretability and clinical applicability in heterogeneous inpatient rehabilitation populations. Therefore, this study aimed to evaluate patient experience in a tertiary inpatient rehabilitation setting using the AM-CCRQ tool alongside multidimensional measures of functioning and functional independence, namely Clinical Functioning Information Tool (ClinFIT) and Functional Independence Measure (FIM) tools, respectively. This integrated approach seeks to provide a more nuanced, rehabilitation-specific interpretation of PREM, provide feedback on the quality of rehabilitation service and offer further avenues for targeted service improvement.
Methods
Participants and Setting
This is a prospective study conducted at the 40-bed inpatient rehabilitation unit of a tertiary referral centre in Victoria, Australia. This study was approved by the hospital ethics committee as a quality assurance project. The participants were recruited from the inpatient rehabilitation ward from July 2024 to December 2024. The inclusion criteria included: >18 years of age, able to communicate in English, medically stable, ability and willingness to give informed consent. Those with severe cognitive issues, severe receptive dysphasia, or substantial psychiatric disorders that prevented informed consent were excluded.
Procedure
A total of 142 patients were screened between July 2024 to December 2024. Out of 142 patients, 40 were excluded based on the inclusion and exclusion criteria (22 due to severe cognitive-communication impairments, and 18 due to their inability to communicate in English). A total of 102 patients were recruited and invited to participate in the project by an independent project officer, and informed consent was obtained from all participants.
A primary independent research officer explained the study to the participants, and the paper-based AM-CCRQ was administered for participants to complete anonymously towards the completion of inpatient rehabilitation program. The AM-CCRQ data forms were collected by returning a de-identified envelope, secured, and filed into a password-protected database by an independent data entry officer.
Data collected in addition to the AM-CCRQ included an electronic medical record audit of demographic information, main impairment group for admission, and routine rehabilitation outcome data, including the International Classification of Functioning, Disability and Health (ICF)-based Clinical Functioning Information Tool (ClinFIT)33-36 and Functional Independence Measure (FIM) scores. 37 Participants were assessed at baseline (T0) and at the completion of the rehabilitation program for ClinFIT and FIM scores. The Clin-FIT was used to evaluate functions across clinically relevant domains of the ICF, while the FIM was used to assess levels of independence and assistance required. Together, these measures enabled a collaborative assessment of patient experience across varying levels of case complexity, function, and independence, providing a more comprehensive, rehabilitation-specific interpretation of PREMs by situating patient experience within the multidimensional realities of rehabilitation care.
Australian Modified Client-Centred Rehabilitation Questionnaire (AM-CCRQ)
The AM-CCRQ is a self-reported patient experience questionnaire including 31 items evaluating components of patient-centred care relating to inpatient rehabilitation setting (Supplementary Material 1). The AM-CCRQ enables patients to report their experience during their episode of care. The AM-CCRQ comprises 31 items scored on a five-point Likert scale ranging from ‘strongly agree’ (1) to ‘strongly disagree’ (5). Seven items also have a ‘does not apply’ (DNA) response. The 31 items are categorised into 7 subscales: 1. Decision-making (6 items: Q1, 6, 8, 13, 17, 20). The patient’s perceived level of participation in decision-making and goal setting in their rehabilitation program. 2. Education (4 items: Q2, 18, 21, 27). The patient’s perception of the education they have received with regard to their health condition and rehabilitation treatment. 3. Outcome evaluation (4 items: Q3, 9, 14, 29). The patient’s perception of how well they were informed of their progress and outcomes during their rehabilitation program. 4. Family involvement (5 items: Q4, 10, 19, 22, 28). The patient’s perception of how family or significant others were engaged and informed during the patient’s rehabilitation program. 5. Emotional support (4 items: Q5, 11, 23, 25). The degree of emotional support the patient perceived they received during their rehabilitation program. 6. Continuity/coordination (4 items: Q15, 26, 30, 31). The patient’s perception of the communication and coordination during their rehabilitation program. 7. Physical comfort (4 items: Q7, 12, 16, 24). The patient’s perception of the management of their pain and physical comfort during their rehabilitation program.
The ‘DNA’ responses were retained from the denominator for quantitative analyses when calculating domain-level summary scores and item-level percentages to reflect the full distribution of the responses and avoid overestimation of positive response rates.
ICF Clinical Functioning Information Tool (Clin-FIT)
It comprises of 30 categories, derived from the ICF core model, that define a minimum set of information on “functioning” and “disability” collected across health conditions along the continuum of care: “Body Functions” (9 items) and “Activities and Participation” (21 items).33-37 These categories, accompanied by clinically meaningful descriptions, are used to assess patient functioning on an 11-point numerical rating scale, ranging from “No problem” (0) to “Complete problem” (10). The ClinFIT demonstrated good internal consistency reliability, with a Cronbach alpha coefficient of 0.97 (Supplementary Material 2).
Functional Independence Measure (FIM)
The FIM comprises 18 categories, with the score measures in each area reflecting the level of dependency. The FIM consists of motor domain (13 items), assessing the level of function in 4 subscales: self-care, transfers, locomotion and sphincter control; cognition domain (5 items) in 3 subscales: communication, psycho-social and cognition. Participants are rated on each item on a scale of 1 to 7 (1=total assistance, 4=requires physical assistance, 5=needs supervision, 6=modified independence, 7=independent) by trained staff. 38
Statistical Methods
The socio-demographic and clinical characteristics of participants were analysed and summarised using basic descriptive analysis. These characteristics included age, gender, main impairment group, living situation and employment status. The AM-CCRQ item responses were similarly analysed using descriptive analyses, focusing on counts and proportions. To examine changes in Clin-FIT raw total score at admission (T0) and discharge (T1), a composite radar chart was used to represent the functional profile using the raw score and mean and standard deviation were calculated. A paired-sample t-test was used to calculate differences in outcome measures (ClinFIT and FIM) at T0 and T1 to examine improvements in participants’ functional outcomes during rehabilitation. A p value of <0.05 was set as the level for statistical significance. All calculations were performed using IBM SPSS Chicago, Illinois, US for Windows version 30.0.
Results
Participant Characteristics
A total of 51 responses were returned during the study period, yielding a response rate of 50.0% (51 out of 102), with non-response being primarily due to patient refusal or incomplete responses. When considered relative to the total recruited cohort, this corresponds to a completion rate of 35.9% (51 out of 142). The socio-demographic and clinical characteristics of participants are shown in Supplementary Material 3. The mean age of the respondents was 68 years (range 27-91), with over half being female (n=28, 54.9%). The most common conditions included orthopaedic (29.4%), stroke (23.5%) and trauma (11.8%). Most patients (54.9%) were from home with a partner or family; over half of the patients who were retirees (51.0%), 29.5% employed (27.5% full-time, 2% part-time) and unemployed (19.6%).
Outcome Measurement Scores
Australian Modified Client-Centred Rehabilitation Questionnaire (AM-CCRQ)
The AM-CCRQ items, grouped by subscales, are summarised in Supplementary Material 4. Most items had valid response rates, with 64.7% completing all the 31 items. The items relating to the family involvement subscale (items 4, 10, 19, 22, 28) had the highest “Does not apply” (DNA) responses (19.6%, 21.6%, 15.7%, 17.6%, 17.6% respectively), followed by the items relating to physical comfort subscale (items 7, 12, 16, 24) (11.8%, 13.7%, 0%, 0% respectively). Items involving decision-making, education, outcome evaluation, emotional support and continuity/coordination of care had 100% response rates.
The distribution of responses to individual items, grouped by subscale, is shown in Figure 1. Out of 31 items, 23 items had 80% or greater portion of positive response (“agree” and “strongly agree”). The aspects that participants rated positively (‘strongly agree’ and ‘agree’ responses) were demonstrated for: • Item 24 (n = 50) Rehabilitation staff tried to ensure my comfort • Item 11 (n = 48) I was treated with respect and dignity • Item 13 (n = 48) My treatment needs, priorities and goals were important to rehabilitation staff • Item 21 (n = 48) My therapy program was explained to me in a way that I could understand (A) Proportion of responses of Australian modified client-centred rehabilitation questionnaire by item number. (B) Proportion of responses of Australian modified client-centred rehabilitation questionnaire by subscale
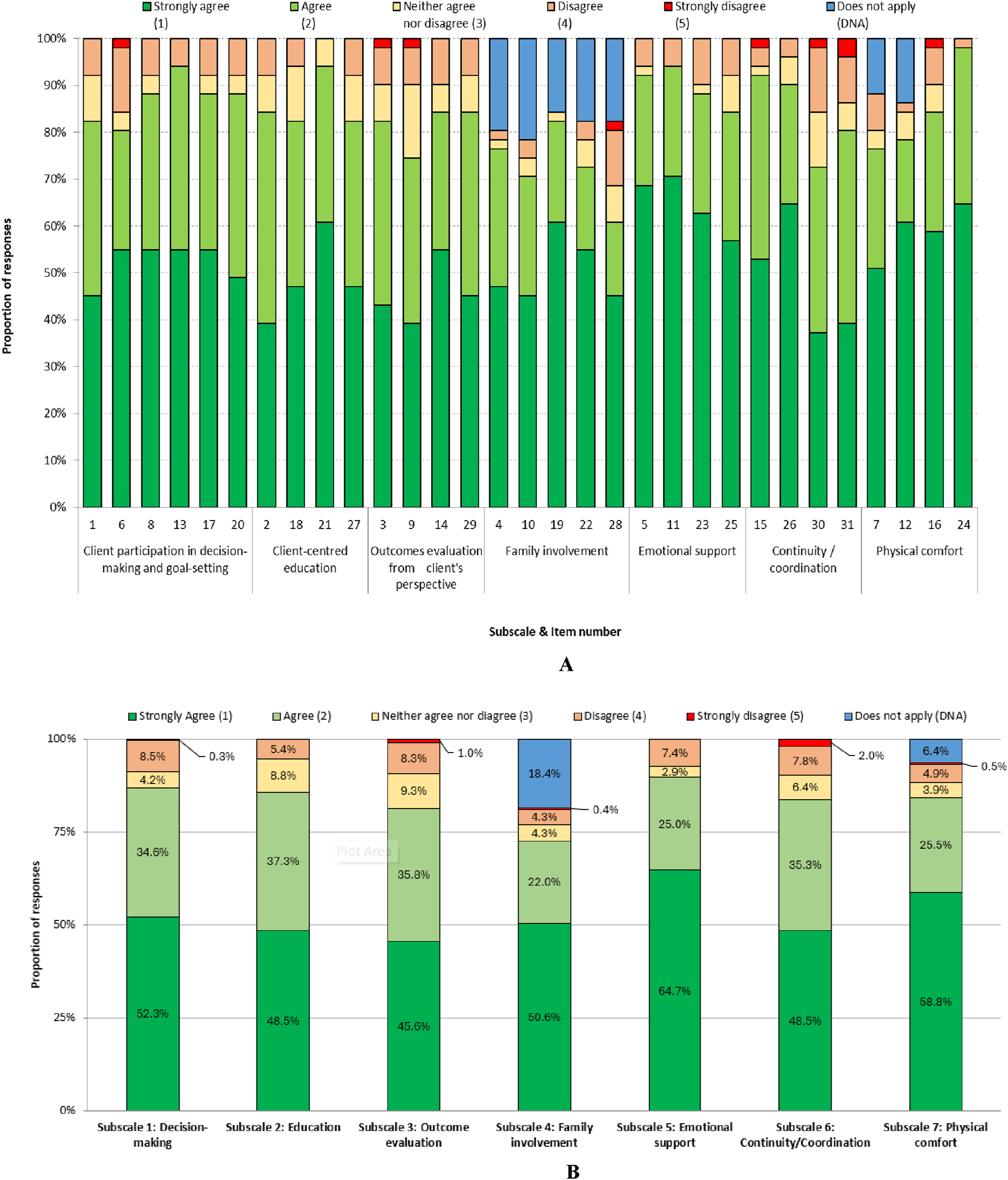
The highest positive responses by subscale included:
The aspects that participants rated lower, in descending order, included: • Item 30 (n = 8) I know who to contact if I have problems following discharge • Item 31 (n = 7) I was told what to expect when I go home • Item 28 (n = 7) My family/friends received information to assist in providing care for me at home • Item 6 (n = 4) The rehabilitation staff tried to accommodate my needs when scheduling my therapy
The items belonging to Subscale 4 Family Involvement had the lowest proportion of positive responses (range 60.8% - 82.4%), the highest proportion of ‘does not apply’ (DNA) responses (range 15.7% - 21.6%) and the largest variability in positive response across all 31 items. After excluding DNA responses, the items within the family involvement subscale that had the lowest proportion of positive responses included: • Item 28 (n = 31) My family/friends received information to assist in providing care for me • Item 22 (n = 37) My family/friends were involved in my rehabilitation as much as I wanted • Item 10 (n = 46) My family/friends were given information when they needed it
Functional Outcomes
Participants demonstrated substantial functional impairment (low FIM) and high multi-dimensional disability across ClinFIT categories, indicating a clinically complex cohort, within which patient experience findings should be interpreted. Most participants reported at least one issue related to one or the other ClinFIT categories. The most affected ClinFIT categories at admission (T0) were “d470 Using transportation” (86.3%), followed by ‘d640 Doing housework’ (86.3%), and ‘d455 Moving around’ (82.4%). Despite the lower rating scores, at discharge, the most concerning issues were “d470 Using transportation” (58.8%), followed by “d660 Assisting other” (51.0%), and “d455 Moving around” (41.2%). The top ten patient-reported issues at admission and discharge are listed in Supplementary Material 5.
Most participants, irrespective of their health condition, showed improvement from admission to discharge (Figure 2 and Supplementary Material 5). Mean scores for each ClinFIT item at admission and discharge. Rating: 0=no problem, 10=complete problem (see Table 1 for comparative analysis scores and Supplementary Material 5 for the most prominent issues reported at both admission and discharge)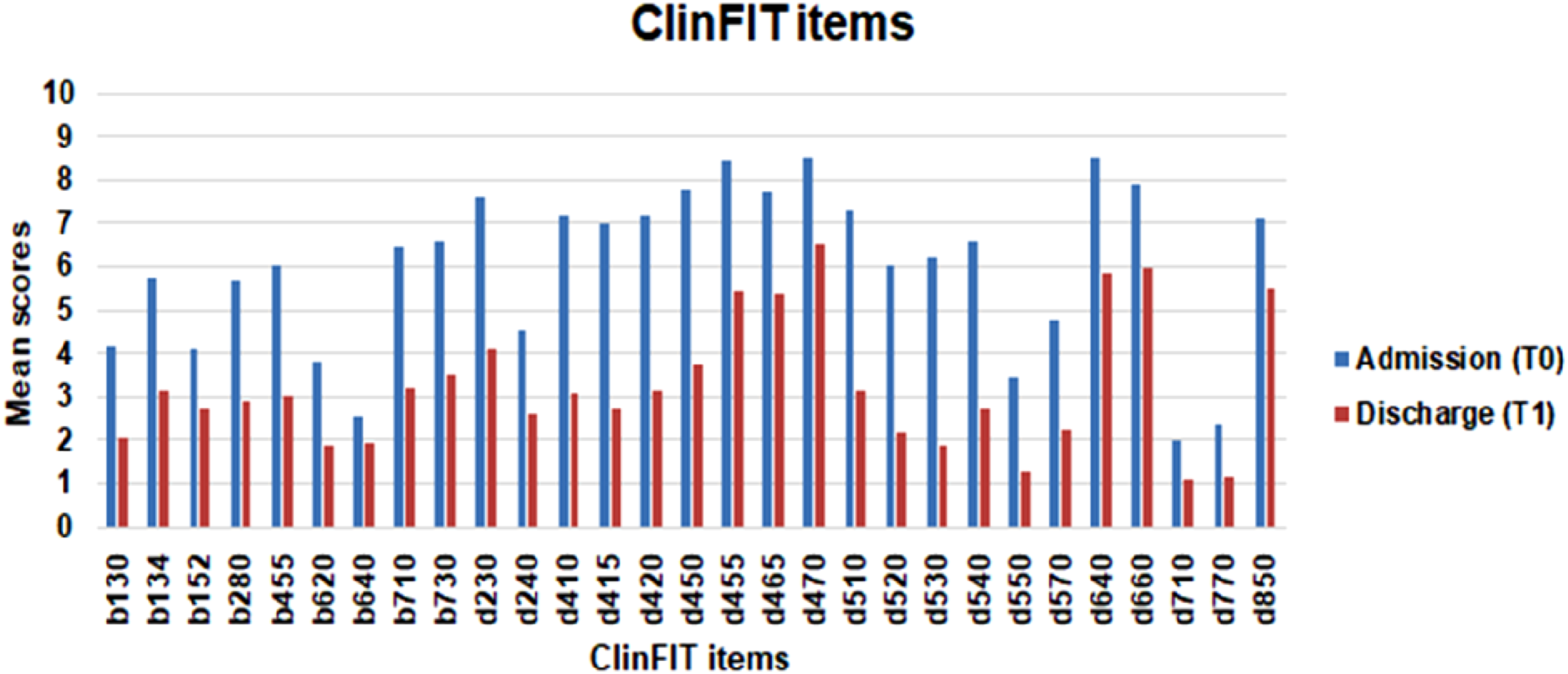
Figure 3 presents the composite radar chart and provides a graphic representation of the functional profile from the ClinFIT data. The 30-scale items are arranged as spokes of a wheel (codes out the circumference), with ICF qualifiers from 0 = no problem to 10 = complete problem, running from the centre outwards. Blue lines represent the mean admission (T0) scores, and the red lines represent the median discharge (T1) scores. b130-b730 represents 9 ClinFIT “Body function” categories and d230–d920 represents 21 ClinFIT “activity and participation” categories (see Table 1 for comparative analysis scores). Composite radar chart illustrating the mean scores for each ClinFIT item at admission and discharge Change Scores of Measurement Scale Over Time (n =51) ClinFIT: Clinical Functioning Information Tool; FIM: Functional Independence Measure; M: mean; MD= Mean difference. 95% CI: 95% confidence interval; SD: standard deviation; n: total number of participants. *Paired sample t-test. Correlations significant at the <0.05 level (2-tailed) are bolded.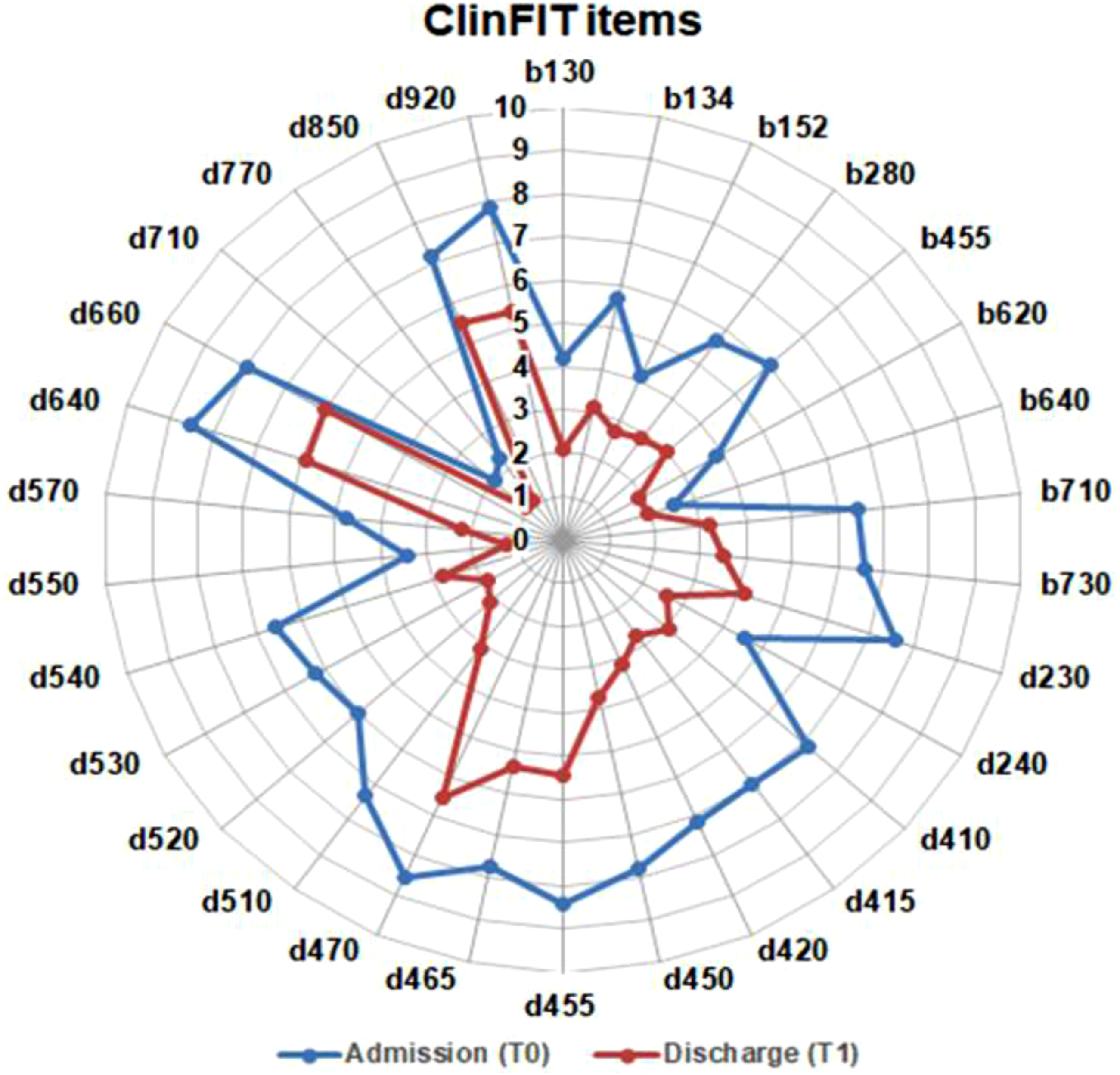
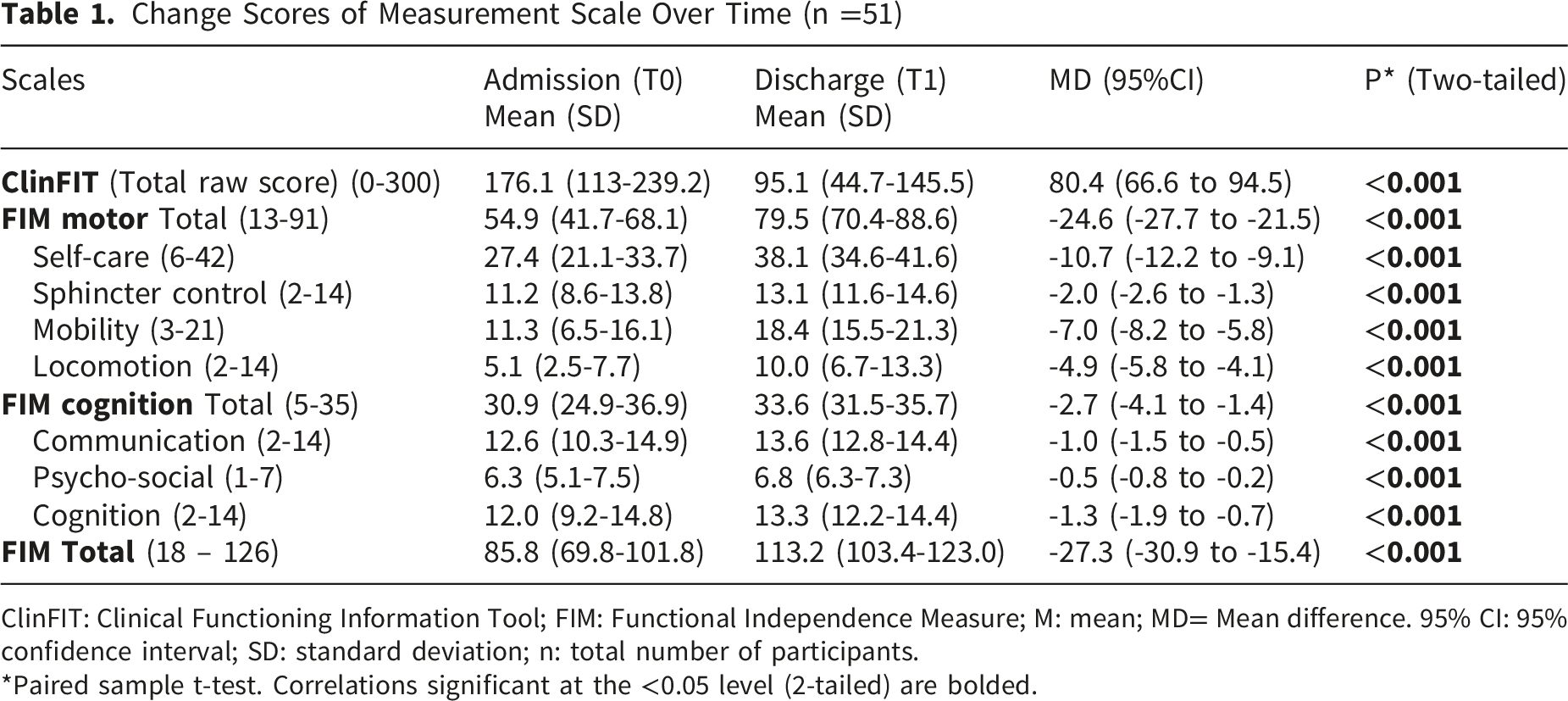
Compared to the admission (T0) [Mean (SD): 176.1 (113-239.2)], there was a significant improvement in participants across all health conditions in ClinFIT total raw score at discharge (T1): 95.1 (45.1-135.1), p <0.001 (Table 1). A paired-samples t-test on outcome measures (ClinFIT, FIM) at different assessment points (T0 and T1) are provided in Table 1. At discharge (T1), a significant improvement in participants’ functional and cognitive outcomes was noted in FIM motor ‘total’ and all subscales: ‘self-care’, ‘sphincter’, ‘locomotion’, ‘mobility’, ‘communication’ (p <0.001 for all), and FIM cognition ‘total’, and ‘communication’, ‘psychosocial’ and ‘cognition’ subscales (p <0.001 for all) (Table 1).
Discussion
To our knowledge, this is the first study evaluating patient experience in an inpatient Australian rehabilitation cohort, using a rehabilitation specific patient experience tool. Whilst most rehabilitation facilities in Australia provide patient experience surveys at the conclusion of care, these instruments are typically generic and contain minimal rehabilitation specific questions, such as state-wide public hospital survey tools, generic patient satisfaction surveys and subscription-based patient experience survey tools.23,38
The availability of this rehabilitation-specific AM-CCRQ data provides more relevant insights to evaluate service performance and identify areas of improvement for quality, safety and patient-centred care. This study aimed to further advance current PREM applications by integrating AM-CCRQ with objective measures of functioning and independence to contextualise patient experience within clinical complexity, whilst demonstrating the value of benchmarking to guide targeted service improvement beyond conventional quantitative measures.
Overall, the AM-CCRQ results revealed a high proportion of positive responses (‘agree’, ‘strongly agree’), particularly in the domains related to emotional support, decision-making and education. This pattern suggests that the participants generally perceived their rehabilitation as patient-centred, with these aspects of care being recognised as strengths. Conversely, there was variability in positive response across certain domains, highlighting actionable areas for further service improvement. For instance, there was a larger disparity between positive responses for the items within subscale 6 (continuity and coordination of care) (72.5 - 92.2% range). Participants had higher positive responses (“agree and “strongly agree”) for items relating to item 15 (n = 47, 92.2%) “I knew who to contact if I had problems or questions during my stay” and item 26 (n =46, 90.2%) “My therapists, nurses and doctors worked well together”. However, lower scores were noted in item 30 (n = 8) “I know who to contact if I have problems following discharge” and item 31 (n = 7) “I was told what to expect when I go home”. These findings highlight the need for improved discharge planning, communication, and greater involvement of family or significant others to enhance patient experience and facilitate community reintegration.
Notably, most participants in this study reported functional challenges across multiple ClinFIT categories, underscoring the complexity of disabilities, functional dependency, and participation restrictions. Although statistically significant improvements in ClinFIT and FIM scores from admission to discharge were observed, concerns remain regarding preparedness for community-based activities after discharge, such as using transport, assisting others, managing household tasks, and maintaining mobility. This suggests that inpatient functional gains may not fully translate to readiness for discharge to real-world environments, which is crucial insight for informing more targeted and nuanced quality improvement strategies.
Addressing these gaps requires more explicit communication and education from the rehabilitation team for patients and their significant others regarding anticipated functional outcomes and post-discharge expectations. Potential strategies include early realistic goal setting at admission, proactive identification and involvement of the primary carer, and structured “preparing for discharge” education sessions, supported by written resources. Emerging technology-enabled solutions may further enhance preparedness, including condition-specific video education, digital resources, and virtual home simulations of real-life tasks. Automated messaging systems can disseminate key information efficiently (e.g. rehabilitation admission details, discharge date, therapy schedules, procedures, family meetings, upcoming appointments), thereby improving communication and reducing clinician time spent on repeated clarification. At a service level, targeted staff education, focusing on communication clarity, checking patient understanding, and proactive engagement of significant others may further strengthen these processes. In addition, expanding ‘rehabilitation in the home’ models offer a practical pathway to support continuity of care and community integration.
This study has several limitations. The cohort was selective, drawn from a single tertiary inpatient rehabilitation service, and restricted to English-speaking participants without significant cognitive-communication impairments. The response rate was modest at 50%, and no additional data were collected to compare respondents with non-respondents, limiting the assessment of potential non-response bias and the risk of over-representation of more engaged patients. As such, the generalisability to the broader inpatient rehabilitation population is limited. Future research should explore strategies to improve response rates, including enhancing accessibility of the AM-CCRQ through flexible completion options (e.g. digital formats) and integration into routine discharge processes.
Given rehabilitation programs are also delivered in the community and in private rehabilitation units, the resource base and priorities for various providers can differ from publicly funded health care systems. Future research needs to address community-based service delivery models and systematically identify variables within patient experience in private versus publicly funded healthcare systems. Given the observational nature of the study, trends in service delivery and patient care could not be evaluated, which may be explored in future larger cohort studies. Furthermore, the AM-CCRQ tool used is still not universally customised to every context within rehabilitation care, given international variation between expectations of providers and system goals and funding models.
Further research should examine the validity and suitability of utilising AM-CCRQ across a range of rehabilitation settings and in broader patient cohorts, including those with linguistic diversity or communication impairments. Additionally, future research is required to evaluate its psychometric properties and clinical relevance within a longitudinal quality improvement framework, including its ability to detect meaningful changes at the domain and item levels following targeted service improvements. Such analyses should account for case complexity, functioning and independence, using assessment tools such as ClinFIT and FIM.
Conclusion
This study examined patient experience within an inpatient rehabilitation setting, highlighting its value as a useful system-level indicator of health care quality and safety. Given rehabilitation care is multifaceted and complex and requires a holistic approach, understanding patient perspectives is essential to evaluating and improving service delivery. Integrating patient experience tools such as the AM-CCRQ with functional outcome measures provide a promising avenue for capturing comprehensive and clinically meaningful approach to evaluating patient experience that are not typically addressed by traditional outcome measures. These tools can help identify both strengths and areas for improvement in the delivery of rehabilitation care. However, more research is needed to support the broader adoption of standardised rehabilitation-specific patient experience measures and to explore their full impact on rehabilitation outcomes. As the field continues to shift towards value-based care, embedding patient experience into quality frameworks will be critical to advancing person-centred rehabilitation services.
Supplemental Material
Supplemental material - Evaluation of Patient Experience in Inpatient Rehabilitation Setting: An Australian Perspective
Supplemental material for Evaluation of Patient Experience in Inpatient Rehabilitation Setting: An Australian Perspective by Haeyoon Ryu, Krystal Song, Bhasker Amatya, and Fary Khan in Journal of Patient Experience.
Footnotes
Acknowledgements
The authors have no acknowledgements to declare.
Ethical Considerations
This study was approved by the local hospital ethics committee as a quality assurance project (QA2024101).
Author Contributions
HY, KS: study design; KS, BA, FK: supervision; HY: data collection; HY, KS, BA, data analysis; HY, KS, BK, and FK: manuscript preparation for publication.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The relevant study data has been provided within the study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.