
Abstract
Transitions from inpatient rehabilitation to home critically affect patient recovery and caregiver well-being. Social determinants of health (SDoH) shape these outcomes yet remain underexamined in rehabilitation settings. The objective of this study was to examine the prevalence of SDoH on patient and caregiver experiences during the first 30 days following discharge from a multi-site inpatient rehabilitation facility in the southeastern United States and explore patterns of patient satisfaction and caregiver burden that can influence care transitions. A prospective cross-sectional descriptive study surveyed 61 patients and 50 caregivers using validated instruments assessing SDoH, communication, discharge preparedness, and caregiver burden. Social isolation, affecting 18% of patients and 10% of caregivers, was the most prevalent challenge. Additional challenges include health literacy and transportation barriers. Caregivers experienced substantial burden: 60% decline in social activities, 50% decreased energy, and 40.9% negative physical health effects. However, 58.1% reported strengthened patient relationships. This study identifies the importance of care continuity and SDoHs after inpatient rehabilitation. Interdisciplinary interventions focused on these key challenges are essential for improving outcomes.
Keywords
Introduction
Transitional care involves coordinated actions ensuring continuity and communication as patients move between care settings and providers.1-4 Appropriate transitional care relies on continuous communication between patients, their caregivers, and interdisciplinary care teams who share the responsibility for managing an individual’s care. 1 Often, patients and their caregivers play active roles in planning, coordinating, and managing care-related information. 5 However, their ability to perform these tasks may be significantly influenced by social determinants of health (SDoH). 6
SDoH encompass the societal and environmental conditions in which people are born, grow, live, work, and age, including their access to healthcare. 7 These determinants profoundly influence health outcomes and are increasingly recognized as critical factors during care transitions. The World Health Organization’s (WHO’s) framework emphasizes the influence of SDoH on patients undergoing integrated care within diverse healthcare settings. 8 For instance, a patient may receive exemplary care yet experience poor health outcomes due to challenges like inadequate housing, food insecurity, or limited social support. 9 Prior research has increasingly linked SDoH to health outcomes during care transitions. Adverse events such as higher mortality rates, 10 hospital readmissions, 11 and emergency department visits 12 have all been linked to SDoH. These risks intensify when patients leave structured inpatient support for home-based care. However, the majority of prior research has focused on acute general hospital settings.
Rehabilitation settings provide a unique perspective through which to examine the importance of SDoH. These settings focus on restoring functional abilities and independence. However, successful rehabilitation-to-home transitions depend heavily on addressing SDoH to ensure patients can adhere to therapeutic regimens, access necessary outpatient services, and receive adequate caregiver support.13,14 Failure to incorporate SDoH into clinical practice can undermine the benefits of medical interventions and rehabilitation efforts. 15 Vulnerable populations, such as underserved patients, encounter additional challenges tied to SDoH. Factors such as lack of transportation, financial constraints, housing instability, geographic isolation, and low health literacy have been shown to affect health outcomes during care transitions.5,16-18
Transitional care is particularly critical for older adults with multiple conditions and complex therapeutic regimens, as well as for their family caregivers. 19 The quality of transitional care is profoundly influenced by SDoH, shaping both patient and caregiver experiences. Caregivers, the primary source of support for patients during transitions, face compounded challenges when coming from disadvantaged backgrounds. These challenges can hinder their ability to facilitate the patient’s recovery and their own well-being. A previous study by Bakas, Champion, Perkins, Farran and Williams 20 using the Bakas Caregiving Outcomes Scale (BCOS) reveals that caregiving experiences can yield both positive and negative dimensions. While caregivers often experience stronger relationships with the patient and family, enhanced self-esteem, and more optimistic outlook on the future, they may also face reduced time for social and family activities, diminished energy levels, poorer physical health, and financial strain. 20
Addressing SDoH is critical to designing transitional care interventions that support patients and their caregivers. 14 These interventions should consider the complex interplay of medical needs, social circumstances, and other factors such as discharge preparation, communication with providers, and available support systems. By understanding the patterns of SDoH and the experiences of patients and caregivers during transitions, rehabilitation organizations and providers may develop patient-centered strategies to enhance care transitions and improve health outcomes. Therefore, the objectives of this study are to 1) explore the patterns of SDoH among inpatient rehabilitation patients and their caregivers during care transitions and 2) examine the patterns of patient and caregiver experiences during transitions, with a focus on how these factors interact and influence outcomes.
Methods
Study Design and Setting
We conducted a prospective study examining SDoH during the 30-day transition from inpatient rehabilitation to home. The study used structured surveys administered either online or via telephone to assess SDoH factors and their relationship to patient and caregiver experiences. The study period encompassed July 2022 through July 2023. The study used the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
The study was conducted at a multi-site inpatient rehabilitation facility in the southeastern United States through its care transitions program. This care transition program focused on supporting patients during their transition from the inpatient rehabilitation hospitals to home. The program provided transition navigation, medication reconciliation, follow-up appointment coordination, and ongoing monitoring to support patients in their home environments.
Participants
The study population consisted of two groups: (1) Adult patients (≥18 years) who had completed an inpatient rehabilitation hospital stay between July 2022 and 2023 at one of the multi-site inpatient rehabilitation facilities and were subsequently enrolled in the care transitions program. Inclusion criteria required English-speaking patients to be at least 30 days post-discharge from inpatient rehabilitation and cognitively able to complete the survey independently or with assistance. Patients with severe cognitive impairments that prevented survey completion were excluded. Cognitive impairment was determined through clinical documentation and information provided by caregivers of patients’ inability to provide informed responses. (2) Primary informal caregivers (family members or friends aged ≥18 years) of the enrolled patients who self-identified as providing regular assistance with activities of daily living, medical care, or other support after discharge.
Recruitment and Sampling
Potential participants were identified upon enrollment into the care transitions program using data retrieved from the electronic medical record. A convenience sampling approach was then used to identify eligible participants who were at least 30 days post-discharge and no more than 90 days post-discharge. This timeframe was selected to allow patients and caregivers sufficient time to establish post-discharge routines and reflect on their transition experiences.
Data Collection Procedures
Eligible participants received an initial phone call inviting them to participate in the study. During this call, participants indicated their preferred method for survey completion. Participants who opted for the online format received a personalized link to the survey via email, which was hosted on the Qualtrics™ platform. The email also included information about the study’s purpose, procedures, risks, benefits, and confidentiality protections, along with a survey link where they could consent and complete the questionnaire. The online survey began with an electronic consent form and took approximately 20-30 minutes to complete.
For those who preferred telephone administration, a specific survey date and time was scheduled. Research staff administered the survey by phone. The phone survey took approximately 30-40 minutes. Verbal consent was obtained at the beginning of the call, and responses were directly entered into the Qualtrics™ platform by the team member. Of the 1,797 patients enrolled in the program during the study period, a total of 61 patients (3.3%) and 50 caregivers were successfully recruited and completed the surveys, and 22 dyads were included in the final sample. Participants received a $10 incentive for their participation in the study.
Data Collection Instruments
The comprehensive survey comprised 11 major sections, with approximately 55 questions for patients and 68 for caregivers (Supplemental material, Table 1). All participants completed demographic information. SDoH were assessed using the Health Leads Social Needs Screening Tool, a validated 9-item instrument that evaluated various SDoH domains. Additional SDoH assessments included questions about social isolation and substance use, measuring frequency of loneliness/isolation on a 5-point scale from “Never” to “Frequently,” and prescription drug misuse and illegal drug use on 5-point scales from “Never” to “Daily or Almost Daily.” All participants were also asked an open-ended question: “Is there anything else that you would like to share about your experiences with the Care Transitions program?”
Patient-specific instruments included the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) follow-up questions, a 6-item assessment that evaluated the quality of discharge planning and transition support. Readmission assessments captured unplanned emergency room visits, doctor’s office visits, and hospital readmissions after discharge, along with reasons for readmission through open-ended responses. The Communication Assessment Tool was administered to assess patients’ perceptions of healthcare provider communication across 15 domains, including greeting, respect, attention, information sharing, understanding, involvement in decisions, and care/concern, with response options ranging from “Poor” to “Excellent” on a 5-point scale.
Caregiver-specific instruments included the BCOS, a validated 15-item scale that measured changes in caregivers’ lives resulting from providing care, using a 7-point rating from “Changed for the worst (-3)” to “Changed for the best (+3)” with a midpoint of “No change (0).” The Caregiver Burden Scale 21 was also administered, comprising 22 items that assessed caregiver burden across multiple dimensions, including physical and emotional strain, social constraints, relationship changes, feelings of being overwhelmed, and impact on health and quality of life, with response options ranging from “Not at all” to “Often” on a 4-point scale.
Ethical Considerations
All collected data were de-identified and stored on secure, password-protected servers to ensure confidentiality. Participation was entirely voluntary, and participants were informed they could withdraw from the study at any time without affecting their care.
Data Analysis
Descriptive statistics were used to summarize the demographic characteristics, SDoH, and patient and caregiver experiences during the transition from inpatient rehabilitation to home. Continuous variables, such as patient age, length of stay (LOS), and household size, were analyzed using means, medians, standard deviations (SD), minimums, and maximums to capture central tendencies and variability within the sample. Frequency distributions and percentages were reported for categorical variables, such as the presence of food insecurity, healthcare access barriers, and caregiver burden.
We examined the distribution of responses across different SDoH domains to identify common patterns and areas of concern among patients and caregivers. For the BCOS data, we organized responses into categories showing positive impact, no change, and negative impact to identify which aspects of caregivers’ lives were most affected by their caregiving responsibilities. The descriptive analytical approach allowed us to characterize the prevalence of SDoH factors in our population and identify potential patterns that could inform future interventions and more complex analytical studies.
Results
Our patient participants reported an average household size of 2.2 (SD=1.30) people with a mean of 0.3 (SD=0.84) children in the household. The average length of stay for these patients in inpatient rehabilitation varied, with a mean of 14.6 days (SD=5.77). The average age of our patient participants was 63.8 years (SD =12.18).
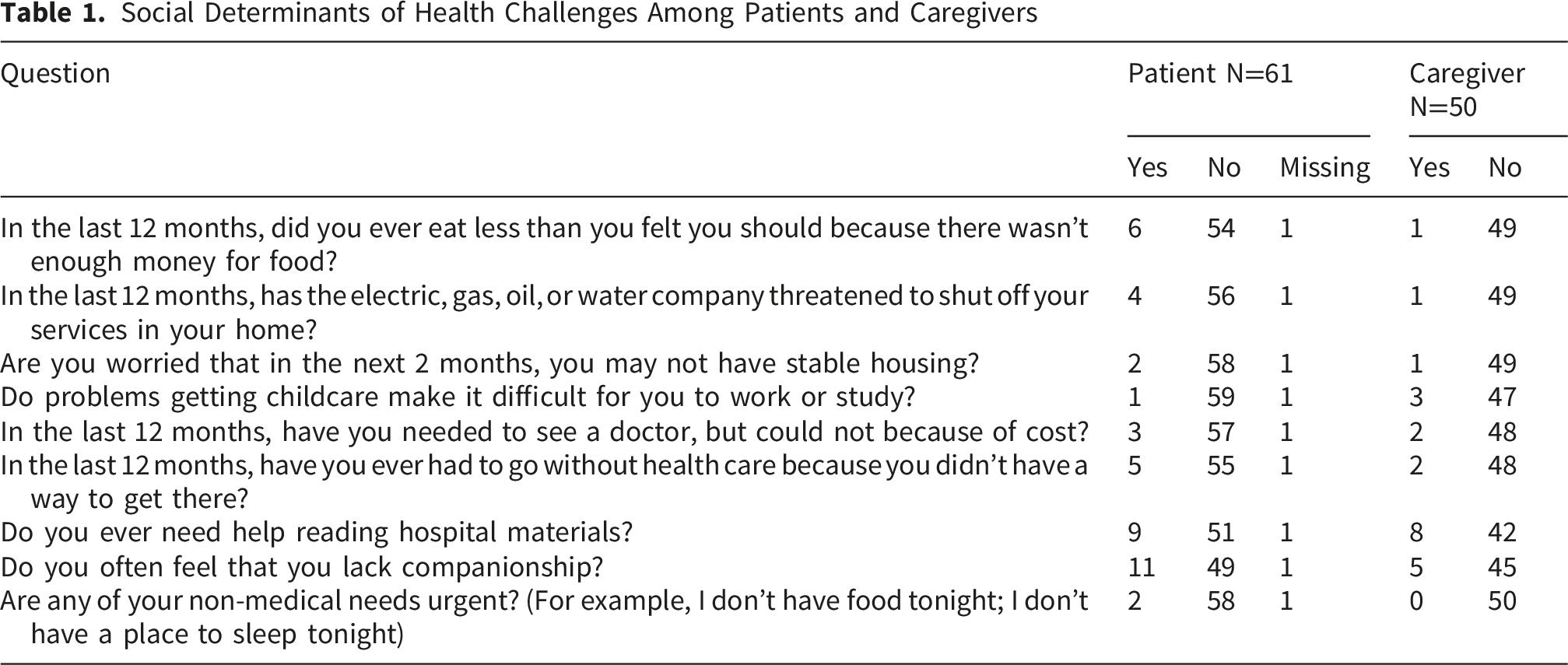
Social Determinants of Health Challenges Among Patients and Caregivers
Discharge Planning and Communication Assessment Among Patients (N=61)

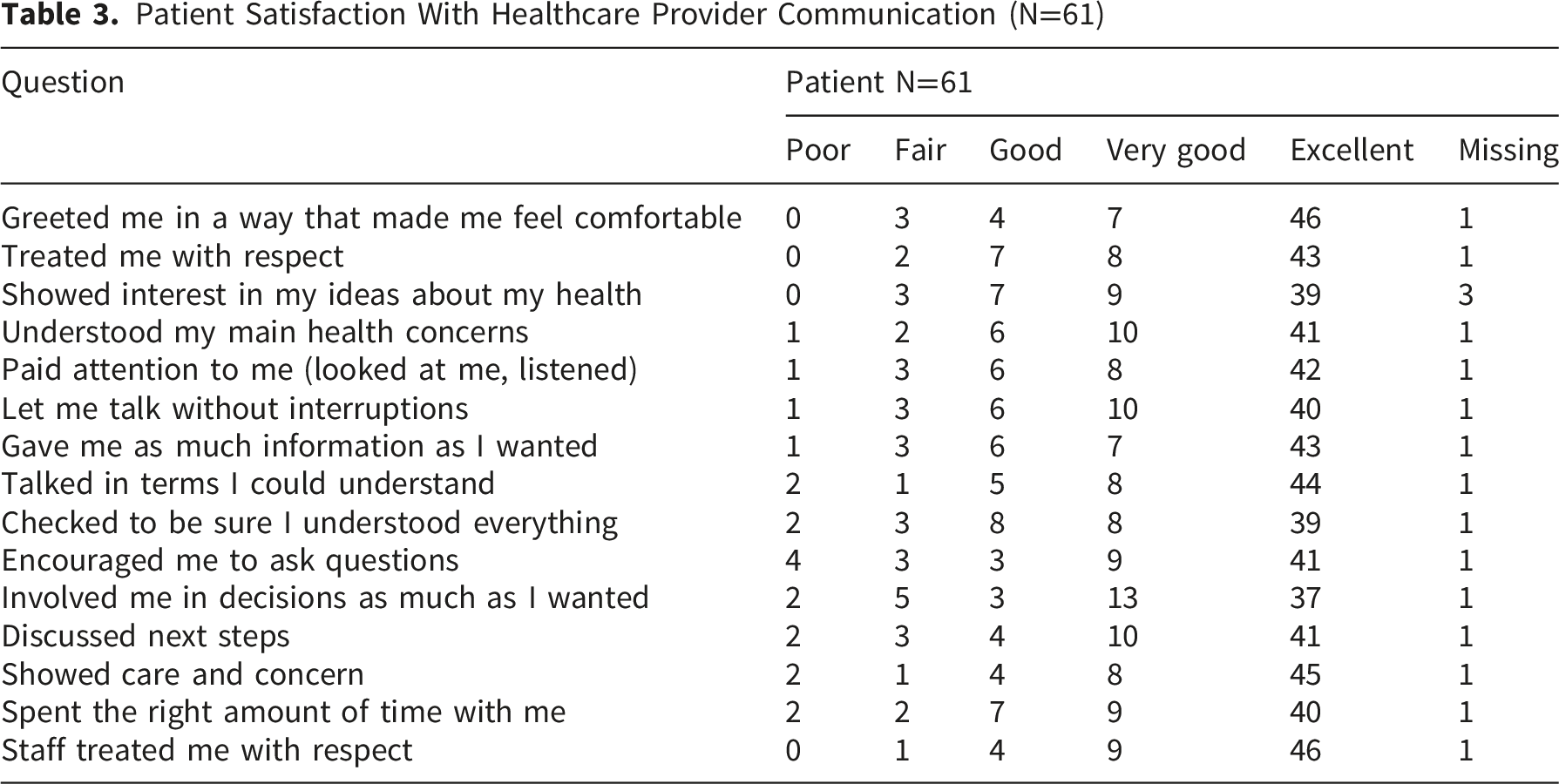
Patient Satisfaction With Healthcare Provider Communication (N=61)
Caregiver Outcomes and Life Changes Following Caregiving Experience (N=50)
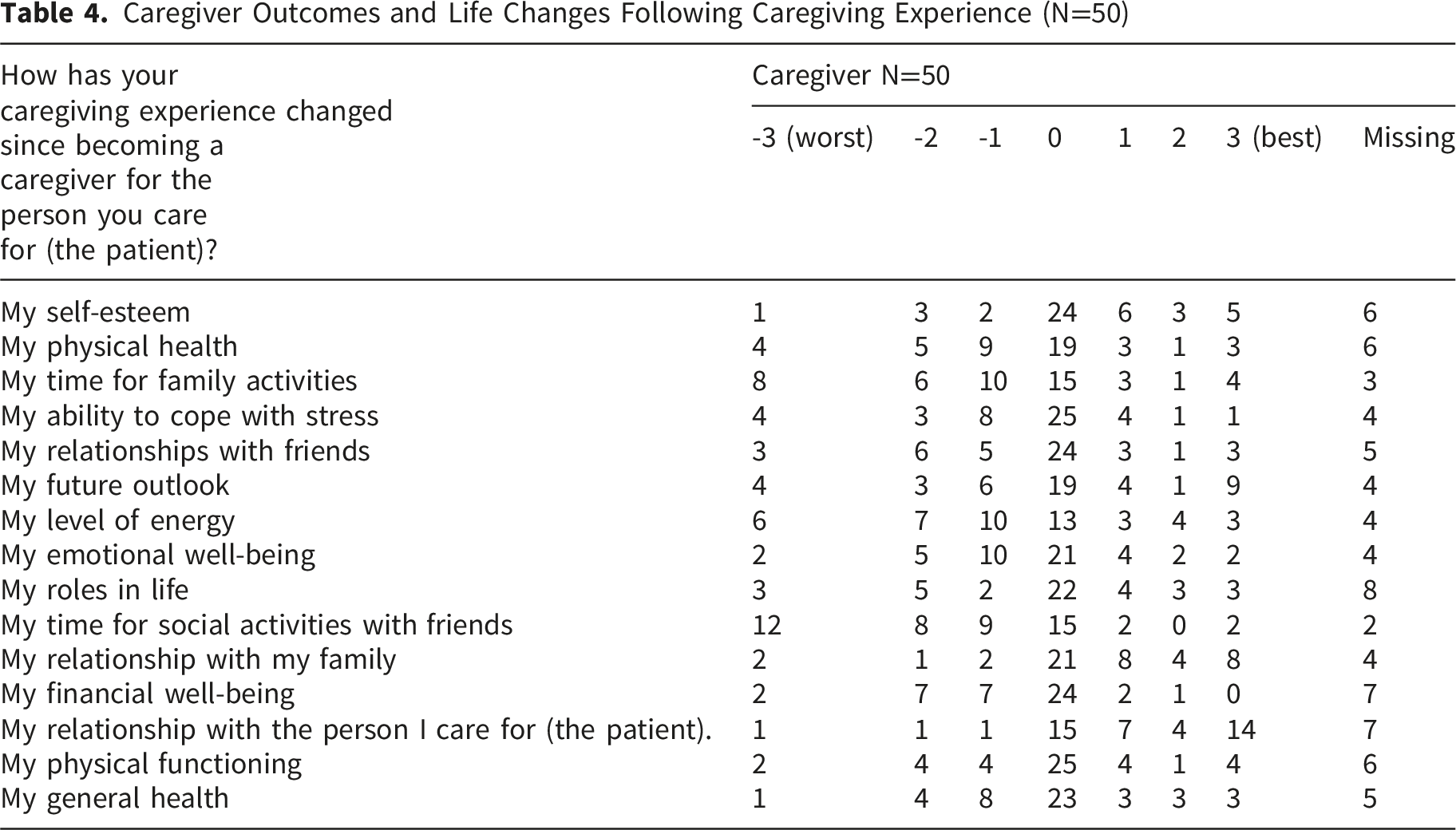
Despite these challenges, many caregivers also identified positive outcomes. A majority (58.1%) of caregivers reported strengthened relationships with the patient, and 43.5% experienced improved relationships with their family, suggesting that caregiving fosters deeper personal connections. Additionally, 31.8% of caregivers noted an increase in self-esteem, and 30.4% reported a more positive outlook on the future, indicating that caregiving may also foster a sense of purpose and fulfillment.
In contrast, some aspects of caregivers’ lives remained relatively stable. Roles in life, physical functioning, and general health showed minimal change. However, stress management and emotional well-being remain areas of concern. Whereby, 32.6% reported difficulty managing stress and 37% experienced emotional strain. While some caregivers found resilience, only 13% reported improved stress coping abilities, underscoring the need for accessible mental health resources and caregiver support programs.
Discussion
The purpose of this study was to examine SDoH, along with patient and caregiver experience, which influence the transition from inpatient rehabilitation to home. This study identified important converging pressures on patients and caregivers during the first 30-days post inpatient rehabilitation stay. Post-discharge recovery is a shared cognitive, social, and economic task carried by the dyad (patient-caregiver), and gaps in any one domain compromise the others. Health literacy and social isolation, which are known to influence post-acute outcomes, were the most prevalent SDoH among patients. Caregivers similarly experienced strain, including reduced social engagement, decreased energy, and physical and financial challenges. Discharge planning and communication were rated highly across nearly all domains, yet it did not solve the social and behavioral conditions experienced by both patients and caregivers in at-home recovery. These results reflected the multifaceted nature of transitional care and emphasized the need to address both clinical and non-clinical factors to support successful transition to home. Overall, this study highlights the need to address SDoH and caregiver capacity within the same care plan to ensure a comprehensive approach to transition care. This approach would allow for better alignment with functional and recovery goals.
This study extends the SDoH literature in three main ways. First, it examines SDoH at the rehabilitation-to-home transition rather than the acute hospital discharge, where care outcomes differ. In rehabilitation hospitals, post-discharge functional recovery and self-management demands differ from those in acute care hospitals.22,23 Second, the dyad approach to this study by pairing patients and their caregivers during the same recovery window allows for the two points of view to be explored with intentionality. Third, this study links SDoH measures to valid communication and caregiver burden survey instruments, allowing us to treat clinical and social factors as connected rather than two separate but parallel constructs.
This study found that the transitions from inpatient rehabilitation to home are particularly critical for patients, especially those living in small or single-person households. Caregivers in those same households face strain as they might be absorbing the social and energy costs. A recent 2024 study found that across the United States, social isolation or loneliness (31.9%) and lack of social and emotional support (24.8%) were the most commonly reported SDoH measures. 24 Consistent with prior research, the findings from this study showed these adults experienced more social isolation, with over a quarter of patients and caregivers reporting feelings of loneliness. 25 This isolation is not only emotional, but also clinically significant, as loneliness has been linked to poorer health outcomes, delayed recovery, increased risk of depression, and higher risk of hospital readmission. 26 Furthermore, caregivers reported substantial declines in social engagement, energy levels, and physical well-being, reinforcing the need for supportive services for caregivers, who are significant partners in recovery. 27 These strains emphasize the need for structured caregiver supports, including interdisciplinary care coordination and a caregiver education program that can mitigate burden and improve sustainability of care. 28 Interestingly, many caregivers also reported positive emotional outcomes, including strengthened relationships and personal growth through improved self-esteem or a more positive outlook. These findings align with existing literature suggesting that while caregiving is undoubtedly demanding, it can also foster deeper interpersonal connections and a sense of purpose when adequate support systems are in place.29,30 Strategically, integrating supports and in-person/online digital tools and resources, such as virtual peer groups and caregiver communication platforms, has shown effectiveness in reducing isolation and supporting patients and their caregivers.31,32
Patients with limited or inadequate health literacy require more intensive transitional care support. Addressing this need is a shared responsibility across all health professions. 33 Low health literacy is related to a serious threat to medication adherence, chronic disease management, and follow-up care. 34 In this study, strong discharge communication scores and patients’ high levels of reported understanding regarding their medications reflect that the rehabilitation facility is already implementing effective strategies. However, self-reported comprehension does not always translate into consistent patient behaviors, such as correct medication-taking, indicating that important gaps remain. Patient-centered discharge education that incorporates multiple teaching methods has been shown to reduce readmissions and increase patient confidence. 35 Reinforcing verbal explanations with clear, jargon-free written materials, using teach-back techniques, and conducting follow-up calls may be essential for ensuring patients understand and apply care recommendations once they return home.36-38
This study highlights the multifaceted needs of rehabilitation patients and their caregivers during the transition home. Transitions from inpatient rehabilitation to home are demanding because patients are expected to assume greater responsibility for self-management while still recovering from significant functional impairments. It also must account for socioeconomic vulnerabilities, emotional and social well-being, and the capacity of both patients and caregivers to manage complex care regimens. While recent federal and state budget proposals have included reductions to social safety net programs, such as Medicaid and community-based support services, 39 these shifts may limit access to essential resources that support transitions from inpatient rehabilitation to home. In this context, interventions that address health literacy, improve access to follow-up care, address mental health and social support needs, and recognize caregiver strain become even more critical for transitional care. The frequencies observed in the study, especially around health literacy, social isolation, and caregiver strain, reflect the distinctive demands of rehabilitation discharge and the need for transition strategies tailored to the rehabilitation patients and their households. A patient-centered, SDoH-informed discharge approach may have the potential to improve recovery trajectories and promote long-term well-being of both patients and their caregivers.
Limitations
Our study had several strengths, such as an in-depth understanding of the SDoH among both patients and their caregivers. There is inconsistent reporting of the SDoH related to rehabilitation services provided after discharge within the scientific literature, indicating the importance of documenting and reporting the role of SDoH. This study has several limitations that affect the interpretation and generalizability of findings. The descriptive cross-sectional design prevents us from drawing causal inferences between SDoH and outcomes. Furthermore, a recruitment form limited to a geographic area reduces generalizability. Convenience sampling may have introduced selection bias, as participants who agreed to participate may differ systematically from those who declined. The sample sizes of 61 patients and 50 caregivers, while adequate for descriptive analysis, limit the statistical power to detect associations between variables or to conduct subgroup analyses. The 30-day post-discharge timeframe captures immediate transition experiences but may not reflect longer-term outcomes or recovery trajectories. Furthermore, the 30-day timeframe may have introduced recall bias.
Conclusion
Successful transitions require recognizing SDoH interventions as essential transitional care components. In addition, there is a strong need for measurable benchmarking to successfully address the SDoHs of both patients and caregivers. As the healthcare system evolves its payment structure, new healthcare reimbursement models may need to incorporate and support comprehensive discharge planning that addresses social risks. Specifically, in inpatient rehabilitation facilities, SDoH screening needs to be integrated into standard discharge protocols targeting patients who may experience high social risk factors. Healthcare systems should also establish dedicated caregiver support programs, which will require allocating resources for respite care services, caregiver education programs, and mental health support specifically designed for the rehabilitation-to-home transition period.
Supplemental Material
Supplemental Material - Social Determinants of Health and Patient Experiences During Transitions From Inpatient Rehabilitation to Home
Supplemental Material for Social Determinants of Health and Patient Experiences During Transitions From Inpatient Rehabilitation to Home by Hanadi Hamadi, Chloe E. Bailey, Mindi R. Manes, Trevor Paris, Heather A. Kendall, Sinyoung Park, Jing Xu, Kristen Hicks-Roof, Aaron Spaulding in Journal of Patient Experience
Footnotes
Acknowledgements
The authors would like to thank the patients and caregivers who participated in this study.
Ethical Considerations
Ethical approval for this study was obtained from the University of North Florida Institutional Review Board (April 5, 2022/IRB#1879810-4)
Consent to Participate
Informed consent was obtained from participants in this study information for the publication of this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Brooks Rehabilitation Collaboration Grant (no grant number), and the University of North Florida Brooks Professorship Grant (KEY003607)
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data underlying this article are available from the corresponding author upon reasonable request for privacy reasons.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.