
Abstract
Patient death is one of the most emotionally challenging experiences for healthcare professionals. Introducing structured education early in training may promote resilience and support more compassionate, patient-centered care. At Texas A&M Naresh K. Vashisht College of Medicine, preparation for patient death was historically addressed through the “hidden curriculum,” defined as informal, unspoken learning that occurs outside the formal educational structure. Recently, students led an initiative to develop a formal educational session—Preparing Students for Patient Death—combining asynchronous and live components for second-year students prior to clerkships. In Spring 2024, the session was piloted as part of the Practice of Medicine 3.5 course for approximately 60 students on the Dallas and Round Rock campuses. The session included a physician-led video and a live interdisciplinary panel, with Dallas students completing pre- and post-session surveys. Of the 40 Dallas attendees, 29 completed the pre-survey and 14 completed the post-survey. Findings showed increased preparedness (2.4 to 3.4), high clinical relevance (100% agreement), and strong endorsement (100% would recommend), addressing a key gap in medical education. These results suggest that early, interprofessional education on patient death and dying addresses a critical gap in undergraduate medical education that may support both student well-being and future patient care.
Introduction
Experiencing the death of a patient remains one of the most significant challenges faced by healthcare team members throughout their careers. Physicians, alongside chaplains, palliative care specialists, social workers, nurses, and other interprofessional team members, support patients and families through the emotional and logistical realities of end-of-life care. When encountered without preparation, these experiences may lead to burnout, maladaptive coping, and reductions in empathy. 1 Physicians-in-training are often involved in end-of-life discussions, care planning, and patient advocacy, placing them at particular risk for secondary trauma during an already demanding phase of professional development. 2
Processing the death of a patient—whether expected or sudden—can be deeply distressing in the absence of structured resources and healthy coping strategies. This challenge has become even more pressing following the COVID-19 pandemic, during which physician burnout surged and mental health outcomes worsened across the profession. 3 Burnout has been linked to long-term emotional distress, reduced empathy, and lower career satisfaction among physicians, which can in turn influence communication, decision-making, and the patient experience at the end of life.4,5 Preparing medical students to engage with patient death in a supported, reflective manner may therefore have downstream benefits for both physician well-being and patient care quality.
Over 90 medical schools currently address patient death within their medical school curriculum and give their students a space to prepare to process the feelings that accompany the loss of a patient. 6 At Texas A&M Naresh K. Vashisht College of Medicine, preparation for patient death was historically addressed within the “hidden curriculum,” referring to the informal, unspoken education that occurs alongside the formal curriculum in medical school. While students receive instruction on communication skills, such as delivering bad news and responding to grief, and have access to wellness services, including therapy, the emotional toll of witnessing patient death has received less structured attention. Students have limited opportunities to develop coping strategies or access institutional support resources during these experiences, underscoring the need for both dedicated training and supportive resources as they enter clinical environments. For many, patient death is first encountered during training, and without guidance, emotional responses may feel isolating despite being common and worthy of validation and support.
In 2023, student representatives from Texas A&M College of Medicine attended the Southern Organization of Student Representatives conference, where they engaged in discussions with peers about the critical need for structured support systems for medical students encountering patient death. These conversations inspired the creation of a student-led initiative tailored to the multi-campus model of the College. The program emphasizes both the human experience of patients and families and the emotional development of future physicians within collaborative care teams, with the goal of cultivating compassionate and resilient clinicians.
Methods
In January 2024, the College included a session titled Preparing Students for Patient Death as part of the Practice of Medicine 3.5: Transition to Clerkships pilot course. The curriculum was developed by a student-led working group in collaboration with faculty advisors in medical education and student wellness. Content was developed to adapt to a multi-campus model with an emphasis on reflection, narrative medicine, and discussion of lived clinical experiences.
This optional session was offered to second-year medical students at two campuses—Dallas and Round Rock—with approximately 60 students participating in total. To incentivize participation, students completing the course were offered an additional NBME STEP 1 practice exam during their dedicated study period.
The session included two parts:
(1)
(2)
Surveys were developed by the study team to assess self-reported familiarity with patient death, preparedness to care for dying patients, perceived clinical relevance, and usefulness of the session. Participation was voluntary, with the option to opt out. While both campuses participated in the educational session, formal evaluation was conducted only on the Dallas campus to assess acceptability and perceived value on the Preparing Students for Patient Death curriculum prior to broader implementation. Students on the Round Rock campus completed the curriculum without formal evaluation during this initial phase. This variation reflected differences in student leadership capacity at the secondary campus during the pilot phase.
Students on the Dallas campus (n ≈ 40) completed the surveys as a part of the Practice of Medicine 3.5 pilot course evaluation survey. Perceived preparedness, familiarity, and awareness of coping strategies were measured using 0–5 Likert scales and responses to outcome statements. Descriptive analyses were conducted by the authors. The study was approved by the University Institutional Review Board (IRB # STUDY2024-0980, STUDY2023-0007).
Results
Forty students were in attendance for the Preparing Students for Patient Death session on the Dallas campus, of whom 29 submitted the pre-survey (72.5% response) and 14 students submitted the post-survey (35% response).
Previous Experience With Death and Dying
In the pre-survey, over 50% of respondents reported being either “Not at all” or “A little” familiar with patient death. On a scale from 0 (Not at all familiar) to 5 (Completely familiar), the mean familiarity score was 1.69 (SD 1.29). Additionally, 27.5% of respondents reported no prior experience with patient death. Among those with prior experience, most cited the death of family members (69%), followed by friends (31%), patients (24%), and professional or work-related experiences (7%) (Figure 1). Pre-Session Student Past Experience With Patient Death (Select all that apply)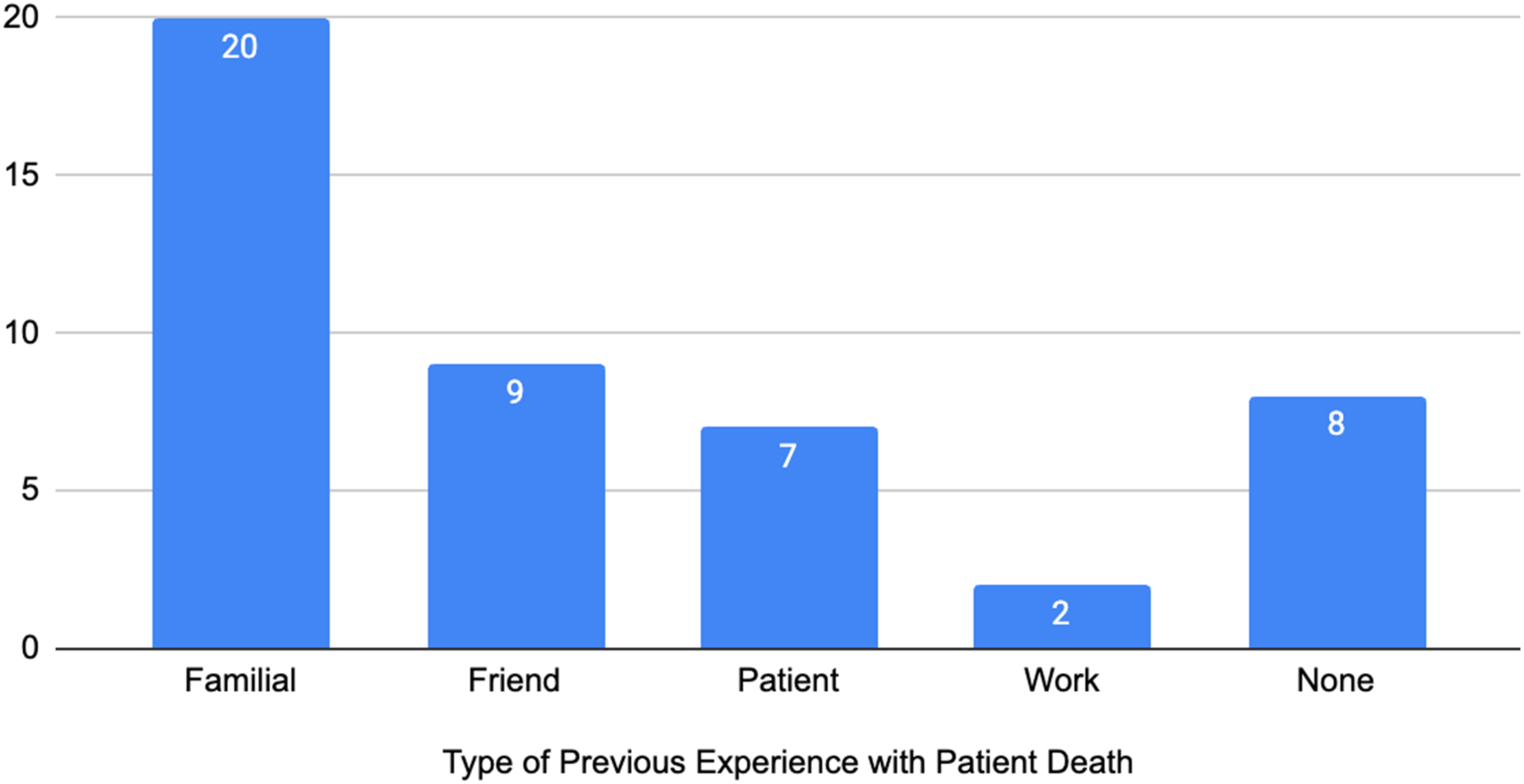
Perceived Level of Preparedness for Patient Death
Pre-session preparedness ratings had a mean of 2.4 (SD 1.03), with a mode and median of 2. Post-session preparedness ratings increased to a mean of 3.4 (SD 0.81), with a mode and median of 4 (Figure 2). Perceived Level of Preparedness to Care for Dying Patient and Manage Patient Death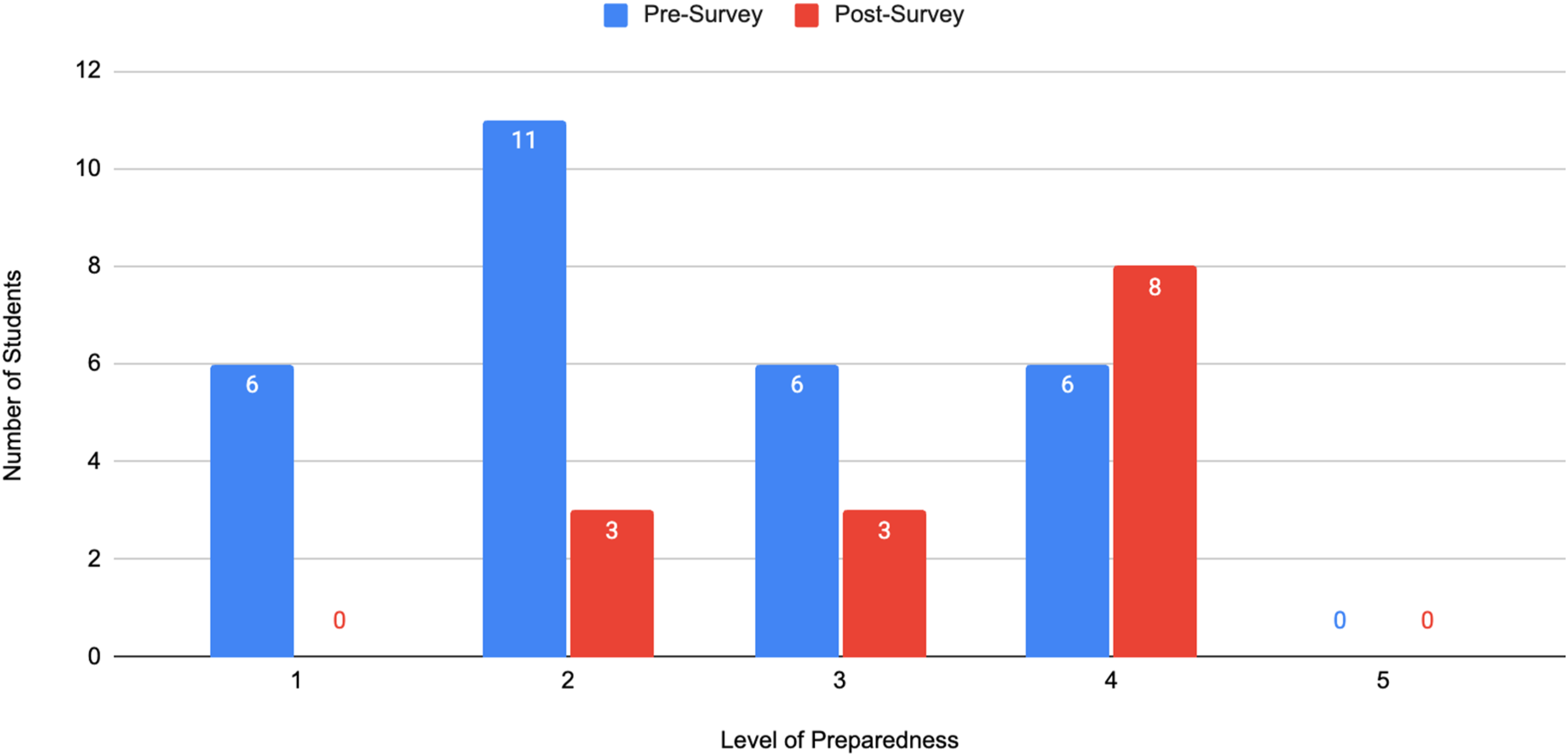
Perceived Clinical Relevance
All post-survey respondents agreed that the session was clinically relevant, with 85% strongly agreeing and 14% agreeing with the statement, “The program had sufficient clinical relevance.”
Learned Skills
Ninety-three percent (93%) of post-survey respondents agreed or strongly agreed with the statement: “I learned skills that I can use in the future when caring for a dying patient or a patient who has died.” One student (7%) selected “Neither agree nor disagree.”
Usefulness
The usefulness of the session was evaluated with a 0-5 Likert Scale. Of the 14 students who responded to the post-survey, 36% expressed that they found the preparation for patient death curriculum “5-Very Useful. 29% expressed that they found the curriculum “4-Mostly Useful”, and another 29% found it “3-Moderately Useful”. Seven percent (7%) found the curriculum “2-Somewhat Useful” and no students found the curriculum to be “1- A Little Useful” or “0-Not at all Useful”.
In addition, 100% of post-survey respondents responded that they would recommend this program to other and future Texas A&M Naresh K. Vashisht College of Medicine medical students.
Discussion
Findings from the single-site evaluation of the Spring 2024 pilot suggest that the session effectively improved students’ perceived preparedness to manage patient death and provided clinically relevant, applicable skills for future encounters in clinical settings. These skills included debriefing with peers and mentors during rotations and acknowledging loss with patient families in a professional manner.
Prior to the session, the majority of students reported limited familiarity with patient death, with a mean familiarity rating of 1.69 out of 5. This aligns with broader trends in undergraduate medical education, where exposure to patient death often occurs informally and without adequate guidance or structured reflection. 7 Most students’ experiences with death involved family or friends, further emphasizing the gap between personal and professional preparedness.
Following the session, students demonstrated increased self-reported preparedness, with mean preparedness scores rising from 2.4 to 3.4. Although based on descriptive data, the shift in mean, median, and mode suggests that even a brief, focused educational intervention can positively influence students’ confidence in approaching death and dying within clinical contexts.
Students overwhelmingly affirmed the clinical relevance of the session, with 100% of students expressing that they agreed or strongly agreed with the sentiment. This feedback reinforces the importance of addressing death and dying as a core part of the pre-clerkship curriculum, rather than relegating it to the hidden curriculum or leaving it to be addressed informally through clinical exposure alone.
In terms of practical outcomes, 93% of students agreed that they gained skills they could apply when caring for dying patients or processing patient loss. This indicates that the curriculum went beyond raising awareness and provided tangible tools for emotional resilience and professional development. Additionally, the strong endorsement of the session, as 100% of respondents reported that they would recommend it to peers, supports its value as a sustainable component of the curriculum.
For institutions seeking to replicate this model, key elements include early timing prior to clerkships, intentional interprofessional representation, and facilitation that prioritizes psychological safety. These components may be adapted to local resources while maintaining the program’s core objectives.
Limitations
Despite these promising results, it should be noted that the response rate for the post-survey was lower than that of the pre-survey (35% vs. 72.5%), which introduces response bias. Students who completed the post-survey may have been those who found the session particularly impactful or relevant, which could skew the data positively. There are multiple reasons that the post-survey may have gotten fewer responses, including difficulty enforcing survey completion at the end of the session. Additionally, the study relied on self-reported measures rather than objective assessments of knowledge, skills, or behavior and was conducted before clerkships began. While self-assessment provides important insights into perceived preparedness, it may not fully reflect actual competence or readiness in real-world clinical environments. This evaluation was also based on confidence prior to starting clerkships. The authors acknowledge that more direct, objective evaluation during and after clerkships could add value to this study and there are plans to do so for future iterations of this course.
Conclusion and Next Steps
Texas A&M College of Medicine students responded positively to the introduction of the Preparing Students for Patient Death curriculum, first piloted and evaluated on the Dallas campus in January 2024.
The session addressed a critical gap in medical education by helping students prepare to process the emotional realities of patient death—an experience many encounter for the first time during clerkships. Key takeaways included the perceived clinical relevance of the topic, the acquisition of practical coping strategies such as reflective writing, peer and mentor debriefing, and engagement with pastoral or wellness services, and a notable increase in students’ self-reported preparedness to respond to patient death. Although evaluation data was collected from a single campus during the pilot phase, the curriculum has since been implemented across all campuses beginning January 2025 for the Class of 2027 and beyond.
To strengthen evaluation of the program’s long-term impact, future iterations will incorporate: - Longitudinal tracking of students’ experiences with patient death during clinical training - Qualitative and quantitative assessments to measure changes in both emotional resilience and clinical communication skills
Additionally, a clerkship peer mentorship program is currently being piloted on the Dallas campus. Fourth-year medical students have been trained to serve as peer mentors, providing support to clerkship students during emotionally challenging experiences, including but not limited to patient death. This peer-based-support model offers a confidential, student-centered approach to processing emotionally challenging clinical experiences in real time and complements the foundations established in Practice of Medicine 3.5.
Together, these initiatives demonstrate a growing institutional commitment to fostering compassionate, emotionally prepared physicians at Texas A&M Naresh K. Vashisht College of Medicine. As the curriculum and support programs continue to evolve, these initiatives hold promise to improve both student well-being and patient care.
Footnotes
Acknowledgements
Thank you to My Lai for supporting the creation of the modules used in this project, and to Martin Hinojosa for assisting with the editing and creation of the videos—and for both of your willingness to record in person on campuses when it was not possible for us. Thank you to Talia Meidan for her support in evaluating this pilot and thank you to Dr. Halil Sari for reviewing the statistical analysis in this paper. We are deeply grateful to Dr. Renee Higgerson, Dr. Nicole Bedros, Dr. Patricia Watson, Dr. Joyce Hnatek, Dr. Kashif Piracha, and Dr. Rakhi Dimino for participating in the video modules, sharing your insights and personal experiences regarding patient death and its impact, and for your vulnerability in doing so. Thank you to Dr. Roque Ruggero and Dr. Vijar Giridhar for your openness to incorporating this curriculum into the Practice of Medicine 3.5 pilot. Finally, thank you to the Texas A&M faculty for supporting this student-led initiative and allowing us to pursue this work with your guidance and encouragement.
Ethical Considerations
This study, Preparing Medical Students for Patient Death: A Pilot Curriculum at Texas A&M College of Medicine, was conducted in accordance with ethical standards for research involving human participants. This study was approved under a secondary use protocol by the University Institutional Review Board under protocol numbers STUDY2024-0980 and STUDY2023-0007. Participation in the study was voluntary, and all participants provided informed consent prior to data collection. Confidentiality and anonymity of participant responses were maintained throughout the research process. No identifying information was included in the analysis or reporting of results.
Consent to Participate
Consent was obtained electronically, with participants affirming agreement by responding to the prompt: “Do you agree with the terms of the survey listed above and are you willing to participate in this study?”
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Texas A&M Naresh K. Vashisht College of Medicine’s Academy of Distinguished Medical Educators’ Innovators in Educator Grant.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.