
Abstract
Background
The Heart Failure Somatic Perception Scale (HFSPS) is a brief instrument designed to assess the perceived burden of common symptoms of heart failure (HF).
Aim
To investigate the psychometrics of the Arabic HFSPS.
Methods
This methodological study investigated the construct validity of the HFSPS among 180 Omani patients with HF through exploratory factor analysis (EFA) and confirmatory factor analysis. Criterion validity was evaluated through correlations with the symptom frequency dimension of Kansas City Cardiomyopathy Questionnaire 12-item (KCCQ-12), Control Attitudes Scale-Revised Five-Items (CAS-R 5), and Patient Health Questionnaire-2 (PHQ-2).
Results
EFA revealed three factors with eigenvalues >1, which explained 56.1% of the variance. Out of seven competing models, a five-factor structure comprising a new factor “weight gain,” which comprised correlated items “11 and 14” in other models, expressed the best fit. It was invariant across gender and marital status with adequate convergent and discriminant validity as indicated by average variance extracted >0.50, strong subscale–total correlations, and acceptable heterotrait–monotrait ratios. Criterion validity was evidenced by significant associations with KCCQ-12 symptom frequency, PHQ-2, and CAS-R 5, and HFSPS reliability was excellent (ω = .93).
Conclusion
Weight gain seems a distinct dimension that deciphers error correlations previously found in the HFSPS. It may relate to patients’ physical activity, nutritional habits, and metabolic dysregulations, necessitating integrating weight control measures in the routine care of patients with HF.
Keywords
Introduction
Heart failure (HF) is a major health problem that strikes more than 65 million people worldwide (676.7 per 100,000 population) and 7.7 million adults in the United States, with estimated annual economic costs of US$27.9 billion (American Heart Association, 2026; Aune et al., 2016; Peng et al., 2025; Ran et al., 2025). It is a major cause of recurrent hospitalization, which depletes the resources of healthcare systems (Olofsson et al., 2025). Despite advanced HF management, it is associated with an excessive global mortality of up to 55.5 million deaths in 2021 (American Heart Association, 2026), with 1-year risk ranging from 20% to 40% to reach 75% over a 5-year period (Aune et al., 2016; Emmons-Bell et al., 2022). HF is an irreversible and progressive syndrome that is characterized by the frequent occurrence of multiple symptoms simultaneously (e.g., breathlessness, lower limb edema, and fatigue), along with many signs, for example, elevated jugular venous pressure and pulmonary crackles (Türker et al., 2025). Accordingly, disease sufferers struggle with increased cumulative sum and severity as well as symptom burden (Jurgens et al., 2017; Stubblefield et al., 2021). Symptom burden is a multidimensional construct that reflects more than the mere presence of symptoms; rather, it is a summary measure that captures the subjective and quantifiable prevalence, severity, frequency, distress, and overall impact of multiple co-occurring symptoms on a person's well-being and daily life functioning (Gapstur, 2007; Löwe et al., 2024). Aggregate data show that symptoms of HF may increase illness workload, form barriers to self-care engagement, and reduce individuals’ capabilities and willingness to access external resources (e.g., hospitals; Austin et al., 2021).
Theoretical Framework
While symptoms vary in their severity, burden, and impact, patients also vary in their manner of perceiving and expressing the symptoms (Türker et al., 2025). Unfortunately, poor symptom detection among HF patients is common, and it impedes timely treatment and promotes poor prognosis (Lee & Moser, 2013)—around 50% of the patients experience dyspnea, which may take acute forms (e.g., orthopnea and paroxysmal nocturnal dyspnea) for 3 or more days prior to hospitalization while most patients endure less acute symptoms (e.g., fatigue, cough, edema, and weight gain) for long time until they interfere with their physical functioning and daily activities. This is because these symptoms are usually confused to be less threatening and normally associated with aging (Antonio-Oriola et al., 2023). On the other hand, seeking information on the disease as well as self-monitoring behaviors are associated with increased control of the disease (Olofsson et al., 2025).
Theory of unpleasant symptoms (TOUS) targets symptoms (multiplicity, timing, intensity, quality, and distress) within a frame that involves interactions among numerous key pathophysiological mechanisms, influencing situational factors, and the resulting performance outcomes for the patients such as health-related quality of life and clinical event risk (Lenz et al., 2003). Thus, it facilitates multifaceted patient-centered holistic nursing approaches that focus on cyclical relationships that underscore the complexity of patient health experiences, with an emphasis on addressing symptoms and their underlying etiology (Blakeman, 2019).
Literature Review
Review studies confirm that symptom measures in patients with HF are limited in number, psychometric performance, and scope of symptom assessment (number, frequency, and severity of symptoms; Lee & Moser, 2013; Santos et al., 2020). Acknowledging limitations in existing symptom measures of HF (e.g., extensive variations in timeframes and type of signs and symptoms, with less attention paid to hallmark symptoms, e.g., dyspnea and subtle symptoms that may act as early indicators of impending decompensation), Heart Failure Somatic Perception Scale (HFSPS) has been developed as a specific measure of the breadth and complexity of HF physical symptoms, including hallmarks (e.g., dyspnea) as well as early and subtle symptoms of impending decompensation (Jurgens et al., 2017). Guided by TOUS, the HFSPS was originally developed as a 12-item measure of subtle symptoms of HF. The scale has been expanded by including six additional items that evaluate dyspnea on exertion, fatigue, nocturia, and symptoms associated with right-sided congestion such as loss of appetite and abdominal swelling (Jurgens et al., 2017). The English HFSPS (Jurgens et al., 2017) has been translated and validated into many languages including Italian (Pucciarelli et al., 2019), Spanish (Antonio-Oriola et al., 2023), Turkish (Türker et al., 2025), Japanese (Hayashi et al., 2025), Farsi (Vajargah et al., 2023), and Arabic (Massouh et al., 2025).
HFSPS testing in most studies involved the use of classic testing theory (confirmatory factor analysis, CFA; Antonio-Oriola et al., 2023; Hayashi et al., 2025; Jurgens et al., 2017; Pucciarelli et al., 2019; Vajargah et al., 2023), sometimes in addition to principal component analysis (Antonio-Oriola et al., 2023), to evaluate the model originally suggested by the developers. However, testing was limited in the Arabic study to the use of primitive methods: its construct validity was evaluated through exploratory factor analysis (EFA) while its discriminant validity was evaluated through correlations with the self-management domain of self-care. While this test would be suitable for criterion validity, it is not relevant to construct validity, that is, it does not indicate if the factors are distinct from each other or not (Massouh et al., 2025). This type of testing is not suitable for discriminant validity testing either since patients actively involved in symptom monitoring usually engage in self-care behavior (Olofsson et al., 2025). Moreover, not a single study examined scale measurement stability between men and women or other patient characteristics. To fill the gap, the current study aimed to evaluate (1) the construct validity of the Arabic HFSPS through EFA and CFA, (2) measurement invariance, convergent validity, and discriminant validity through robust measures, and (3) criterion validity in relevance to symptom frequency, perceptions of control, and depressive symptoms. In this respect, the study hypothesizes that greater symptom burden (HFSPS) would be associated with higher symptom frequency, lower perceived control, and greater levels of depressive symptoms.
Methods
Design, Setting, Participants, and Procedure
This methodological study employed a cross-sectional design and recruited a convenience sample of HF patients from inpatient and outpatient tertiary care facilities from five governorates in Northern and Southern Oman. Data collection was conducted over the course of 7 months through structured personal interviews that were conducted on the phone or in the clinical setting depending on participants’ choice. Interviews were conducted by trained research assistants.
Potential respondents were identified through an initial check of the medical record. Those with documented comorbid dementia, major psychiatric disorders, renal impairment, cancer, and other terminal diseases were not eligible to take part in the study. Communication and hearing difficulties were identified through an initial interview that took place 1 week before data collection; patients with those problems were also excluded. Eligibility criteria included age of 18 years and above, Arabic fluency, and agreeing to take part in the study. During the initial interview an appointment for the data collection interview was determined. According to the rule of thumb (10 responses for each scale item, i.e., 10:1 ratio), the current sample size (N = 180 participants) would be sufficient for evaluating the structure of the HFSPS (Boateng et al., 2018).
Potential participants were assured that participation is voluntary and that refusing to take part in the study has no impact on their care. They were also assured that their data will be used for research purposes only, and that only researchers are allowed to access the data. They all signed an informed consent form before the commencement of data collection. The study is conducted according to the guidelines in the Declaration of Helsinki. The procedure was approved by the Ethics Committee of Sultan Qaboos University (CON/EA/43/2019) and Research Committee of the Omani Ministry of Health (MOH/CSR/20/11605). The STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) guidelines were used in the study.
Instruments
Data were collected on patients’ age, gender, marital status, physical activity, type of HF, etiology, Charlson comorbidity index (CCI), and New York Heart Association Functional Classification (NYHA) in addition to the following psychometric measures.
HFSPS v. 3 is a tool frequently used to measure the awareness and severity of physical symptoms in patients with HF. It comprises 18 items in four subscales: dyspnea/shortness of breath (six items), early and subtle symptoms (seven items), chest discomfort (two items), and edema (three items). It prompts the patients to report the extent to which they are bothered by cardiac symptoms during the past week. Items “e.g., felt my heart beat get faster ‘item 1,’ felt discomfort or pain in my chest ‘item 3,’ had a cough ‘item 5,’ felt tired ‘item 6’” are rated on a five-point Likert scale, with response categories ranging from 0 (I did not have the symptom) to 5 (extremely bothersome). The minimum and maximum total scale scores range between 0 and 90. Higher scores indicate higher symptom burden and vice versa (Jurgens et al., 2017). It consistently demonstrated a four-factor structure in former studies (Antonio-Oriola et al., 2023; Hayashi et al., 2025; Pucciarelli et al., 2019; Türker et al., 2025; Vajargah et al., 2023); however, its construct validity is understudied in an Arab context (Massouh et al., 2025).
Kansas City Cardiomyopathy Questionnaire 12-item Short-Form (KCCQ-12) is a wide-spread sensitive measure of health status that is recommended by the US Food and Drug Administration as an outcome measure of health-related quality of life among HF patients. The KCCQ-12 symptom frequency subscale comprises four items that prompt patients to rate the frequency of having “swelling in feet/ankles or legs; fatigue and shortness of breath that limited your ability to do what you wanted, and being forced to sleep sitting up in a chair or with at least 3 pillows to prop you up because of shortness of breath” over the past 2 weeks. Items are rated on five- or seven-point response categories ranging from 1 (all of the time/every night/every morning) to 5 or 7 (never). Mean scores are indicated as summary scores, and a difference of five points or more is considered clinically important—meaning it is significant enough to reflect a meaningful change in the patient's symptom experience, not just a minor or random variation (Stubblefield et al., 2021). The total subscale scores are standardized to range between 0 (the worst health status) and 100 (the best health status; Jones et al., 2013; Spertus & Jones, 2015). The Arabic KCCQ-12 has been evaluated previously, and it demonstrated adequate test–retest reliability and good concurrent validity (Albarrati et al., 2023).
Control Attitudes Scale-Revised (CAS-R; Moser et al., 2009) is a well-known tool that captures patients’ perceptions of control over their cardiac condition. A five-item (CAS-R 5) short form of the scale has recently exhibited more robust psychometric properties relative to the original CAS-R (Ali et al., 2026). It was developed by dropping negatively worded items in the original CAS-R, along with one positively worded “item 6” that introduced measurement invariance at the scalar level across numerous characteristics. Therefore, the CAS-R 5 comprises five positively worded items “e.g., I feel lots of control, I have considerable ability to control my symptoms.” Items are rated on five-point response categories ranging from 1 (strongly disagree) to 5 (strongly agree). The minimum and maximum total scale scores range between 5 and 25. Higher scores indicate greater levels of perceived control and vice versa.
The Patient Health Questionnaire-2 (PHQ-2) comprises two items, which inquire about key depressive symptoms during the last 2 weeks “losing interest” and “feeling down, depressed, or hopeless.” Items are rated on four-point response categories ranging from 0 (not at all) to 3 (almost every day). The maximum and minimum total scale scores range between 0 and 6, with higher scores indicating more severe depression and vice versa. The validated Arabic version of the scale has been employed in the analysis (Ali, Al-Dossary, Aljaberi et al., 2025).
Statistical Analysis
In an initial step, the structure of the HFSPS was evaluated through EFA with maximum-likelihood method of extraction, Oblimin rotation, Kaiser–Meyer–Olkin (KMO) measure of sampling adequacy, and Bartlett's test of sphericity. This would help us realize how patients’ responses under unconstrained conditions would relate to the latent construct apart from the underlying theory, especially as Oblimin rotation allows for the possibility that factors are correlated, leading to a more realistic and interpretable solution when the underlying variables are related (Ali, Al-Dossary, Fekih-Romdhane et al., 2025).
In a second step, CFA was used to examine nine competing structures of the HFSPS. Beginning with a one-factor model is a valid first step as done by the developers (Jurgens et al., 2017); it assumes that all items on the HFSPS measure a single underlying construct—the somatic symptom burden or perceived physical symptoms, which may be targeted by clinicians to monitor patients’ overall response to interventions. Therefore, the first two models comprised a one-factor structure and a one-factor structure with correlated errors. We replicated the three-factor solution resulting from EFA. Because the pattern matrix indicated cross-loading of item 2 “could not breathe if I lay down” (on the first and third factors) and item 10 “shoes were tighter” (on the first and second factors), those two items were forced to load on factors on which they expressed the highest loadings. In addition, items 8 “feet were swollen” and 15 “woke up to urinate” were omitted as they did not load on any factor in EFA. This model was tested after correlating error terms suggested by modification indices. Because the HFSPS is reported by the developer and all subsequent testing as multidimensional, the study also tested the previously reported four-factor structure (Antonio-Oriola et al., 2023; Jurgens et al., 2017; Pucciarelli et al., 2019), which separates symptoms into four specific domains (dyspnea, edema, chest pain, early and subtle symptoms) and a four-factor structure with correlated errors. Based on error correlations noticed in those models, a five-factor structure was developed as a modification of the four-factor solution—it included a new factor which comprised items with error correlations in the former models. Considering that the overall score of the HFSPS and the scores of its specific domains may be used for certain reasons (e.g., evaluating overall disease burden or evaluating improvement of specific symptoms such as dyspnea in response to specific treatment), two second-order factors based on the four- and five-factor structures were also tested. A second-order solution comprises a hierarchical model where several related first-order latent variables (subconstructs/primary factors) are explained by a single, broader, higher-level latent variable, which is known as the second-order construct (Mansolf & Reise, 2017). Acceptable model fit was determined based on nonsignificant chi-square test (χ2), minimum discrepancy function by degrees of freedom divided <3, comparative fit index (CFI), and Tucker–Lewis index (TLI) > 0.90, along with root mean square error of approximation (RMSEA) and standardized root mean residual <0.08 (Alharrasi et al., 2025; Ali, Al-Dossary, Laranjeira, Amer et al., 2024).
Models exhibiting the best fit were assessed for average variance extracted (AVE) of each factor—an indicator of convergent validity depicted by the average r-squared of items comprising each factor. AVE >0.50 denotes that items properly represent their latent factor (El-Gazar et al., 2025). Heterotrait–monotrait (HTMT) ratios of correlations were estimated to reflect scale discriminant validity, that is, dimensions comprising a model pertain to distinct or unique concepts. It is calculated by comparing the average correlation between indicators of different constructs (heterotrait) to the average correlation between indicators of the same construct (monotrait). Lower values (<.85–.90) identify factors as conceptually different while higher values reflect overlap of the latent constructs (Ali et al., 2022).
Measurement invariance of the best-fitting model across gender and marital groups was assessed through multigroup CFA, which employed four nested models to evaluate model stability at the configural, metric, scalar, and strict levels. These models impose constraints on factor loading, intercepts, and residuals across groups. Significant changes in model fit were indicated by ΔCFI and ΔTLI > 0.020 and ΔRMSEA > 0.015 (Ali, Al-Dossary, Laranjeira, Atout et al., 2024; Ali et al., 2023; Sabah et al., 2024).
Correlations of the HFSPS with its subscales were used to evaluate predictive validity, that is, subscales would demonstrate comparable predictive performance to the parent scale—meaning that they should be equally effective in predicting relevant clinical outcomes associated with the construct being measured (Ali, Al-Dossary, Laranjeira, Atout et al., 2024; Song et al., 2023). For criterion validity testing, correlations were examined of the HFSPS and its subscales with the KCCQ-12 symptom frequency subscale, CAS-R 5, and PHQ-2. For known-group validity, HFSPS subscales scores were compared among CCI groups through one-way analysis of variance (ANOVA). Coefficient alpha (α) and Macdonald's omega coefficient (ω) were used to examine the reliability of all instruments. As an additional check of scale reliability, alpha if item deleted was checked while item total correlations were assessed to reflect convergent validity of the scale at the item level (Alvarenga et al., 2024). SPSS version 25 and Amos version 26 were used to perform the statistical analyses. Significance of the results was determined at probability values below .05 in two-tailed tests.
Results
Sociodemographic and Clinical Characteristics
The sample comprised 180 HF patients with a mean age of 70.3 ± 9.8 years. Most of them were married (n = 122, 67.8%), with more females than males (n = 93, 51.5%). HF with reduced ejection fraction was prevalent in 78.3% of the participants (n = 141), and it was of an ischemic etiology in around two-thirds of the participants (n = 118, 65.6%). Most participants were classified as NYHA functional class II (n = 113, 62.8%). CCI scores of 2, 3, 4, or above were recorded in 18.9, 55, and 26.1% of the participants (n = 34, 99, and 47).
Exploratory Factor Analysis
KMO (0.91) and Bartlett's test χ2(153) = 1,460.8, P = .001 indicate adequacy of sample size and ratio of participants to items for conducting EFA. As shown in Figure 1, the analysis revealed three factors with eigenvalues greater than 1 (7.80, 1.45, and 1.05), which explained 42.2%, 8.1%, and 5.8% of the variance in the HFSPS. While the pattern matrix indicated that items 8 and 15 did not load on any factor, two pairs of items cross-loaded on the second and third factors (Table 1). Items 15, 16, and 8 had the lowest communalities. Interfactor correlations were high (r = .53 and .71), indicating that the three factors were not distinct.
Scree plot of exploratory factor analysis examining the Heart Failure Somatic Perception Scale (HFSPS) among Omani patients (N = 180).
Item Statistics, Exploratory Factor Analysis, Internal Consistency of the Heart Failure Somatic Perception Scale (HFSPS) Among Omani Patients (N = 180).
Note. ITC = item total correlation.
Item 6 “tired” was the most prevalent symptom followed by items 1 “my heart beat get faster,” 3 “discomfort or pain in my chest,” and 15 “woke up to urinate.” Meanwhile, items 14 “clothes felt tighter around my waist” and 11 “gain weight” were the least experienced symptoms.
Confirmatory Factor Analysis
The unidimensional HFSPS expressed suboptimal fit, but most fit indices approached satisfactory fit when two pairs of items were correlated (Figure 2b). The fit of the three-factor solution was unsatisfactory. Modification indices suggested correlating the residual of item 10 with those of items 14 and 11 on the second factor to improve the fit (Figure 2d). Meanwhile, the four-factor HFSPS expressed a fit almost similar to that of models 2 and 3 (Table 2), which considerably improved when the error terms of items 11 and 14 were correlated. The best fit was exhibited by model 7 when a new independent factor “weight gain” was added; it included items 11 and 14. Notably, all items loaded significantly (>0.4, P < 0.001) on the corresponding factors in all models.
Confirmatory factor analysis examining the Heart Failure Somatic Perception Scale (HFSPS) among Omani patients (N = 180).
Goodness-of-Fit of the Confirmatory Factor Analysis of the Heart Failure Somatic Perception Scale (HFSPS) Among Omani Patients (N = 180).
Note. χ2 = chi-square; df = degrees of freedom; CFI = comparative fit index; TLI = Tucker–Lewis index; RMSEA = root mean square error of approximation; CI = confidence interval; SRMR = standardized root mean residual; CMIN = minimum discrepancy function; CI = confidence interval.
AVE expressed by factors of model 5 (0.59, 0.55, 0.35, 0.54, 0.61) was more favorable than that displayed by the factors of model 4 (0.59, 0.55, 0.33, 0.47), indicating a better convergent validity of the former. Meanwhile, the convergent validity of the overall scale was indicated by high item total correlations ranging between .464 and .724 (Table 1). Likewise, item total correlations of subscales of the five-factor HFSPS indicate strong convergent validity of all the subscales at the item level (chest pain: .592, dyspnea: .624 to .772, early and subtle symptoms: .406 to .617, edema: .528, and weight gain: .606). HTMT ratios also indicate a better discriminant validity of model 5 (0.40–0.87) over model 4 (0.56–0.88), albeit both were within acceptable levels. See Supplemental materials (Excel 1, HTMT model 4 and 5) for more details.
The fit of the second-order factors based on models 4 and 5 was similar and better than the fit of all models. All items loaded significantly on the second-order general factor. However, item 14 did not load on the early and subtle symptom factor in model 6; this item was still strongly correlated with item 11. Meanwhile, all items of the dyspnea domain did not load on their domain specific factors in model 7 (Supplemental materials: Excel 1, CFA second-order).
Measurement Invariance
The four-factor and five-factor structures of the HFSPS expressed stability across gender and marital groups as indicated by configural, metric, scalar, and strict invariance (Tables 3 and 4). Models comprising second-order structures failed to converge.
Invariance of the Four-Factor and Five-Factor Structures of the Heart Failure Somatic Perception Scale (HFSPS) Across Gender Groups Among Omani Patients (N = 180).
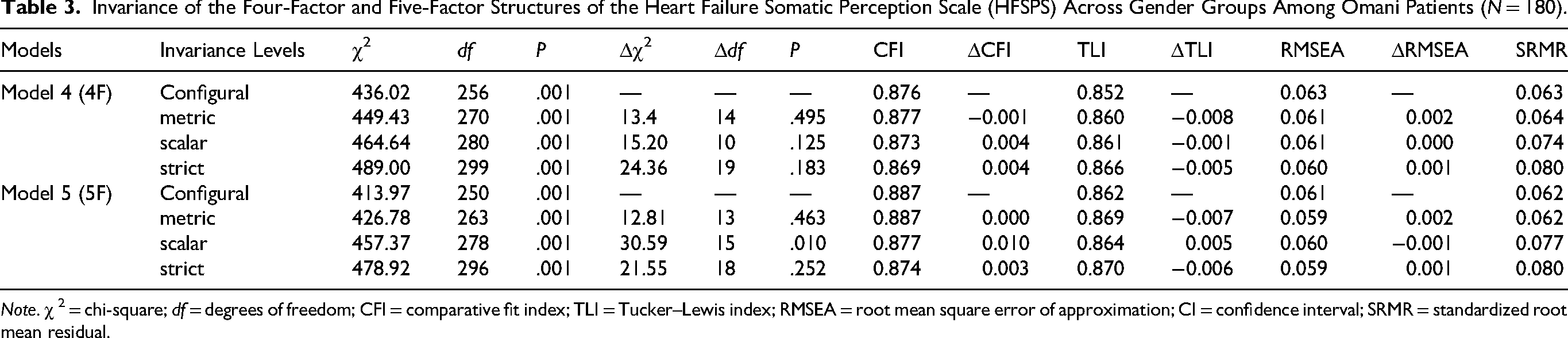
Note. χ 2 = chi-square; df = degrees of freedom; CFI = comparative fit index; TLI = Tucker–Lewis index; RMSEA = root mean square error of approximation; CI = confidence interval; SRMR = standardized root mean residual.
Invariance of the Four-Factor and Five-Factor Structures of the Heart Failure Somatic Perception Scale (HFSPS) Across Marital Groups Among Omani Patients (N = 180).
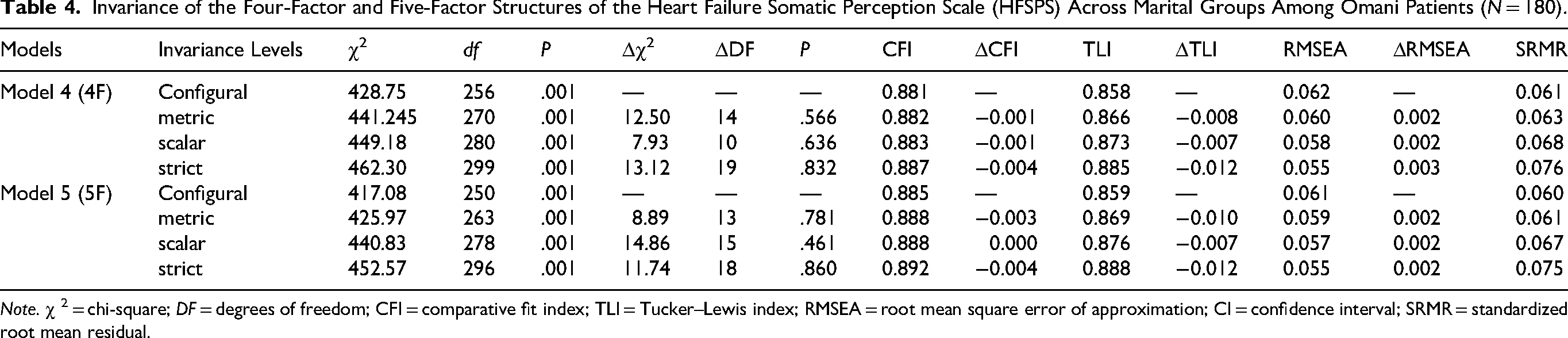
Note. χ 2 = chi-square; DF = degrees of freedom; CFI = comparative fit index; TLI = Tucker–Lewis index; RMSEA = root mean square error of approximation; CI = confidence interval; SRMR = standardized root mean residual.
Predictive Validity, Criterion Validity, Known-Group Validity, and Internal Consistency
As shown in Table 5, the HFSPS strongly correlated with all its dimensions, which also significantly correlated with each other in the support of scale predictive validity. The HFSPS and all its subscales positively correlated with the symptom frequency subscale of the KCCQ-12 and the PHQ-2 (all P values <.01). The HFSPS and two of its domains (dyspnea, early and subtle symptoms 4F/5F) had significant negative correlations with the CAS-R 5, lending support to scale criterion validity. ANOVA revealed a significant within group difference in weight gain scores only across CCI groups, F(2) = 3.14, P = .046. The internal consistency of the HFSPS was excellent (Table 5) while that of its subscales ranged between acceptable (0.70) and very good (0.88). Values of alpha if item deleted (Table 1) indicate minor reductions in scale reliability following the removal of any of its items, indicating that all items contribute to scale homogeneity.
Convergent Validity, Criterion Validity, Descriptive Statistics, and Internal Consistency of the Five-Factor Heart Failure Somatic Perception Scale (HFSPS) and its Subscales Among Omani Patients with Heart Failure (N = 180).
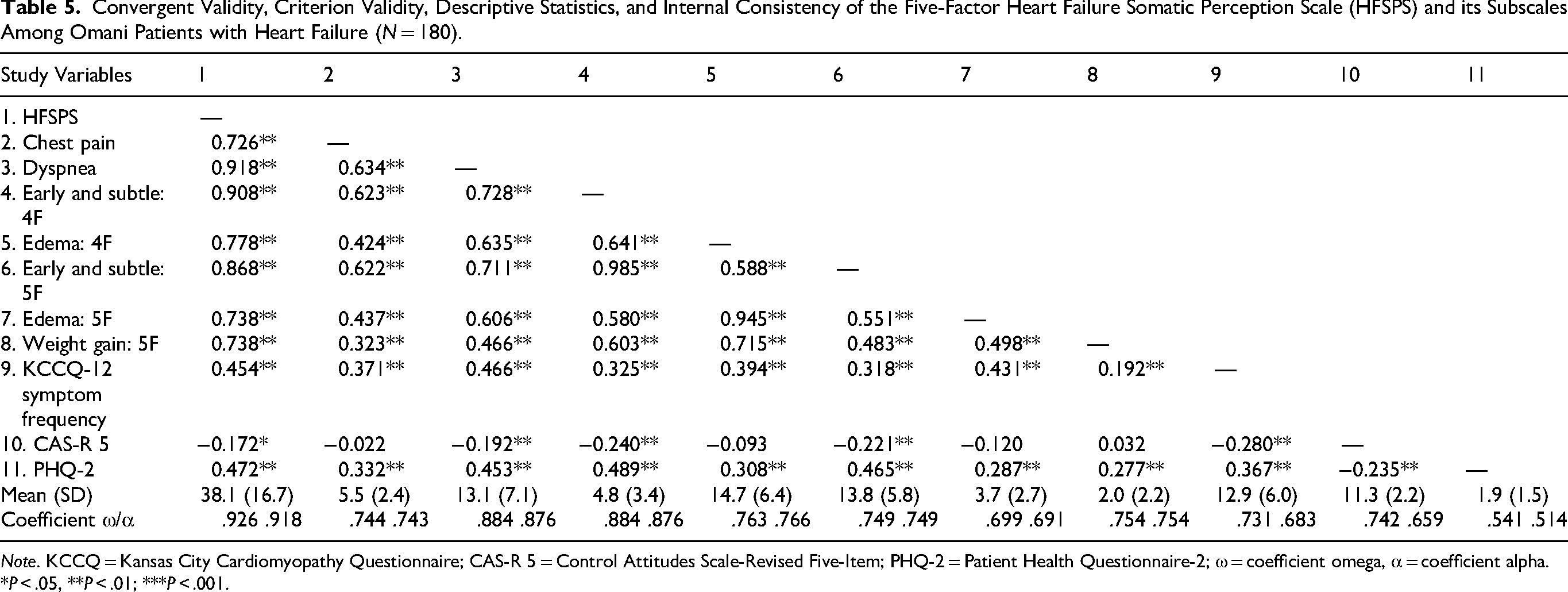
Note. KCCQ = Kansas City Cardiomyopathy Questionnaire; CAS-R 5 = Control Attitudes Scale-Revised Five-Item; PHQ-2 = Patient Health Questionnaire-2; ω = coefficient omega, α = coefficient alpha.
*P < .05, **P < .01; ***P < .001.
Discussion
This study evaluated the psychometric properties of the Arabic HFSPS using EFA and CFA. The best-fitting solutions comprised two second-order models with four and five factors, with correlated errors between items 11 and 14 indicating a distinct weight-gain-related dimension. Addressing a clear gap in the literature, this is the first study to examine HFSPS measurement equivalence across gender and marital status; invariance was supported for the four- and five-domain models—but not the second-order structures—at configural, metric, scalar, and strict levels. Overall, HFSPS subscales showed acceptable to high reliability and adequate convergent, predictive, discriminant, and criterion validity.
To date, only Jurgens et al. have examined a unidimensional HFSPS, which showed suboptimal fit (CFI = 0.880, TLI = 0.864). Although their four-factor model demonstrated excellent fit across indices, except for RMSEA (0.091), it remains unclear whether residual correlations were specified to achieve this fit (Jurgens et al., 2017). The present one-, three-, and four-factor HFSPS had poor fit, which improved after correlating the error terms of chest pain (items 1 and 3 “heart beat get faster” and “pain in my chest”) on the single-factor model, item 10 “shoes were tighter than usual” with 11 “gained weight” and 14 “clothes felt tighter around my waist” on the three-factor structure, as well as item 11 with 14 on the one- and four-factor models. Likewise, the Italian four-factor HFSPS had poor fit due to excessive covariance between three pairs of error terms (item 11 with 14, item 6 with 7, and item 8 with 10), which improved after correlating those residuals (Pucciarelli et al., 2019). The Spanish HFSPS also expressed poor fit, item 6 was removed in EFA, and the fit of the resulting 17-item version improved after correlating the residuals of items 15 with 16 and 17, item 5 with 8, and item 7 with 13 (Antonio-Oriola et al., 2023). Likewise, the Iranian version expressed satisfactory fit after error correlation (item 8 with 10, item 7 with 9, item 4 with 5, and item 15 with both 14 and 16; Vajargah et al., 2023). Item 14 correlated with 13 to achieve acceptable fit of the Turkish HFSPS (Türker et al., 2025). Persistently correlated errors (e.g., involving item 14 across HFSPS versions) indicate systematic, not random, shared variance unaccounted for by the latent factors, suggesting model misspecification.
EFA showed items 11 and 14 loading on a single factor, with item 10 cross-loading; their persistent correlation across models—and in the Italian four-factor solution (Pucciarelli et al., 2019)—supported defining a distinct “weight gain” factor, with satisfactory fit in the absence of correlated errors (model 7), meeting the assumption of local independence. While this factor was supported by EFA loadings and CFA modification indices, item wording reflects central and general obesity; residual correlations of both items together and with item 10 across others models are theoretically justified, consistent with Fornell and Larcker's recommendations (Fornell & Larcker, 1981).
Central and general obesity are highly prevalent in HF patients (77% and 62%, respectively); central obesity, typically indexed by waist circumference, is associated with multiple comorbidities, elevated cardiac filling and pulmonary pressures, markedly reduced aerobic capacity (Darsini et al., 2020; Sorimachi et al., 2022), and increased risk of HF hospitalization or death (Parente et al., 2021). HF patients are prone to obesity due to reduced physical activity driven by fatigue and kinesiophobia—excessive, irrational fear of physical movement (Heimburg et al., 2025). Extensive evidence links general obesity to elevated dynamic plantar pressures, adversely affecting foot structure, mechanics, and function (Mickle & Steele, 2015; Steele et al., 2015), with most patients reporting foot pain (Mickle & Steele, 2015). These findings theoretically justify the new “weight gain” factor, reflecting central (waistline) and general obesity, with item 10 “shoes were tighter” capturing both edema and weight gain.
Fatigue was the most prevalent individual symptom while most participants reported exercising (84.4%, n = 152). HFSPS scores and all domains were higher in nonexercising participants, albeit increases in weight gain were not significant (Supplemental materials: Excel 1, t-test). Thus, physical activity may reduce HF symptom burden, though its effect on weight gain is unclear. Regular moderate-to-high intensity exercise may shift fat from visceral to subcutaneous stores, enhance safe lipid storage, and limit tissue toxicity from proinflammatory adipokines, reducing systemic inflammation, insulin resistance, and oxidative damage (Ali & Kunugi, 2020a). Because data on exercise intensity and frequency were unavailable, exercise dose may have been insufficient to prevent weight gain, particularly with aging, which promotes mitochondrial dysfunction, altered fat distribution, increased visceral fat, and worsening HF (Ali & Kunugi, 2021; Aune et al., 2016; Heimburg et al., 2025).
The five-factor HFSPS is recommended. Although weight gain reflects obesity rather than a direct HF symptom, it is a key risk factor linked to fatigue and reduced activity, which may complicate the condition—factor 2 in EFA comprised “weight gain” and item 16 “had to rest more than usual during the day”—indicator of fatigue or shortness of breath when physically active. Consistent with TOUS, weight gain fits as an antecedent factor, supporting the implemention of weight control interventions like supervised exercise and dietary strategies to enhance patient mobility (Ali & Kunugi, 2020b; Ali, Hori et al., 2021).
HFSPS total scores could not be compared with prior studies, which focused on factor structure, reliability, and validity without reporting overall means. Sample heterogeneity (region, age, disease severity, NYHA class) likely drives variations in symptom averages. Symptom patterns also varied across samples: Omani patients reported more “heart beat faster” and “chest pain,” unlike Spanish or Italian samples (Antonio-Oriola et al., 2023; Pucciarelli et al., 2019) while dyspnea and fatigue dominated in the Iranian cohort (Vajargah et al., 2023). Indeed, meta-analytic evidence identifies four symptom clusters—congestive, weary, ischemic, and stress-related—linked to poorer quality of life (Qiu et al., 2022). Awareness of heart beat “palpitation, the most prevalent symptom in the present sample” in cardiac patients is largely attributed to psychiatric reasons (Alijaniha et al., 2016). According to PHQ-2 cutoff (Ali, Al-Dossary, Aljaberi et al., 2025), 31.1% (n = 56) of subjects screened positive for depression. Welch's t-test indicates significantly higher HFSPS scores across all domains except for edema/weight gain in depressed patients. Fatigue, the first expressed symptom in this sample, is also widely reported by depressed patients (Ali et al., 2023), suggesting psychological factors may shape symptom patterns noticed in this study. Further cross-cultural studies addressing HFSPS association with psychological characteristics are needed.
To date, not a single study evaluated measurement invariance of the HFSPS. Although two second-order factors fit best, they failed to converge in multigroup CFA. In contrast, the four- and five-factor HFSPS demonstrated full invariance across gender and marital groups, ensuring that observed group differences reflect true variations rather than differential interpretations of the scale. This finding is important as researchers are particularly interested in ensuring equivalent scale functionality and robust comparisons of latent constructs between men and women (Ali, Hendawy et al., 2021; Putnick & Bornstein, 2016).
The Arabic HFSPS showed excellent internal consistency, comparable to previous studies (Hayashi et al., 2025; Jurgens et al., 2017; Türker et al., 2025) and higher than earlier Arabic version (Massouh et al., 2025), Iranian version (Vajargah et al., 2023), or the Italian version, whose reliability increased (0.75 to 0.91) when the two-item chest discomfort subscale was removed (Pucciarelli et al., 2019). Despite three subscales having only two items in the five-factor model, all showed acceptable to high reliability (α = .70–.87), reflecting stable measurement with low random error. The reliability of HFSPS subscales has been reported in only three studies (Antonio-Oriola et al., 2023; Hayashi et al., 2025; Pucciarelli et al., 2019), and HFSPS subscale α across studies ranged from acceptable to good for dyspnea, early/subtle symptoms, edema, and chest pain, though the chest pain subscale was omitted in the Italian version to optimize reliability (Pucciarelli et al., 2019).
As for criterion validity, the HFSPS correlated with the KCCQ-12 symptom frequency dimension same as in former studies in which it correlated with similar health status and symptom measures such as all KCCQ domains (Antonio-Oriola et al., 2023; Pucciarelli et al., 2019), Minnesota Living With Heart Failure Questionnaire (Massouh et al., 2025; Türker et al., 2025), symptom status questionnaire-HF (Vajargah et al., 2023), and global physical health of the Patient-Reported Outcomes Measurement Information System (Hayashi et al., 2025). Similar to the results, a single study reported a negative correlation of the HFSPS total score with the CAS-R (Massouh et al., 2025). This study is the first to examine HFSPS criterion validity in relation to depression. High symptom burden was associated with emotional negativity and low perceived control, underscoring the value of psychological assessment and support to improve self-care and prognosis in depressed patients.
Implications for Practice
The results indicate usefulness of overall scale score and subscale scores in the assessment of physical symptoms of HF. This study is the first to spot weight gain as a distinct symptom dimension, with implications for using targeted treatments that would reduce fat accumulation or improper fat deposition and promote safe fat transformation, including physical activity and nutritional modalities such as intermittent fasting and Mediterranean diet (Ali & Kunugi, 2020b; Ali, Hori et al., 2021). Eemotional negativity and low perceptions of control emerged as eminnant determinants of physical symptom burden.
Strengths and Limitations
While most studies opt to evaluate the four-factor structure originally described by Jurgens et al. (2017), this study is the first to evaluate seven competing structures of the HFSPS and its measurement invariance. It underscores the role of depression and low perceived control in HF symptom burden and highlights weight gain as an independent factor warranting careful integration into HF care planning.
The findings may be interpreted with caution due to external validity threats such as including a convenience sample of patients from one small Arab country in the Gulf region, which may possess characteristics (cultural, economic, dietary, etc.) different from patients in other Arab countries. The absence of longitudinal data limits causal inferences regarding the influence of depression and low perceived control on symptom perception and reporting. It also precluded test–retest reliability and longitudinal invariance analyses, given the progressive nature of HF. The small numbers in all NYHA classes except for class II prevented testing measurement invariance and ANOVA-based differences in HFSPS scores across NYHA classes. Subjects were recruited from inpatient and outpatient settings. Although hospitalized HF patients typically report more severe symptoms and poorer prognosis, hospitalization status was not recorded due to low numbers, precluding subgroup analyses. Further studies in more diverse samples are needed to confirm the findings.
Conclusion
The Arabic HFSPS is best described by a second-order structure that is based on four or five factors. This indicates usefulness of the scale's total scores as an indicator of symptom burden while its subscales may be targeted individually to prevent exacerbations specific to certain symptom clusters as well as to establish and maintain complex interventions. Weight gain emerged as an independent factor, and it was not synonymous with edema. It would probably reflect aspects of physical activity, nutritional habits, or metabolic irregularities that would require further investigations and treatment. The four- and five-factor structures were invariant across genders and marital status. Meanwhile, greater symptom perceptions were associated with greater levels of depression and lower levels of perceived control, suggesting a need for mental support to empower patients to actively monitor their symptoms and contribute to their self-care. Replications of the study in different contexts are warranted.
Supplemental Material
sj-doc-1-son-10.1177_23779608261426824 - Supplemental material for Psychometric Properties of the Arabic Version of the Heart Failure Somatic Perception Scale (HFSPS) in an Omani Sample
Supplemental material, sj-doc-1-son-10.1177_23779608261426824 for Psychometric Properties of the Arabic Version of the Heart Failure Somatic Perception Scale (HFSPS) in an Omani Sample by Amira Mohammed Ali, Saeed A. Al-Dossary, Maha Atout, Carlos Laranjeira, Maryam Alharrasi, Ahmed Ayed, Heba Emad El-Gazar, Mona Metwally El-Sayed, Haitham Khatatbeh, Mohamed Ali Zoromba, Amal Diab Ghanem Atalla, Rasmieh Alamer, Maha Subih and Annamaria Pakai in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608261426824 - Supplemental material for Psychometric Properties of the Arabic Version of the Heart Failure Somatic Perception Scale (HFSPS) in an Omani Sample
Supplemental material, sj-docx-2-son-10.1177_23779608261426824 for Psychometric Properties of the Arabic Version of the Heart Failure Somatic Perception Scale (HFSPS) in an Omani Sample by Amira Mohammed Ali, Saeed A. Al-Dossary, Maha Atout, Carlos Laranjeira, Maryam Alharrasi, Ahmed Ayed, Heba Emad El-Gazar, Mona Metwally El-Sayed, Haitham Khatatbeh, Mohamed Ali Zoromba, Amal Diab Ghanem Atalla, Rasmieh Alamer, Maha Subih and Annamaria Pakai in SAGE Open Nursing
Supplemental Material
sj-xlsx-3-son-10.1177_23779608261426824 - Supplemental material for Psychometric Properties of the Arabic Version of the Heart Failure Somatic Perception Scale (HFSPS) in an Omani Sample
Supplemental material, sj-xlsx-3-son-10.1177_23779608261426824 for Psychometric Properties of the Arabic Version of the Heart Failure Somatic Perception Scale (HFSPS) in an Omani Sample by Amira Mohammed Ali, Saeed A. Al-Dossary, Maha Atout, Carlos Laranjeira, Maryam Alharrasi, Ahmed Ayed, Heba Emad El-Gazar, Mona Metwally El-Sayed, Haitham Khatatbeh, Mohamed Ali Zoromba, Amal Diab Ghanem Atalla, Rasmieh Alamer, Maha Subih and Annamaria Pakai in SAGE Open Nursing
Footnotes
Acknowledgments
The authors thank the patients who took part in the study.
ORCID iDs
Ethical Approval
Ethics approval was obtained from the Ethics Committee of Sultan Qaboos University (CON/EA/43/2019) and Research Committee of the Omani Ministry of Health (MOH/CSR/20/11605).
Consent to Participate
Informed consent was obtained from all participants before data collection, ensuring data anonymity and confidentiality.
Author Contributions
Amira Mohammed Ali: conceptualization (lead), methodology (lead), project administration (lead), resources (equal), validation (equal), visualization (lead), writing—original draft (lead), and writing—review and editing (lead). Saeed A. Al-Dossary: formal analysis (lead), resources (supporting), and writing—review and editing (supporting). Maha Atout: data curation (lead), resources (supporting), and writing—review and editing (supporting). Carlos Laranjeira: methodology (equal), validation (equal), and writing—review and editing (supporting). Maryam Alharrasi: investigation (lead), supervision (lead), and writing—review and editing (supporting). Ahmed Ayed: data curation (equal), resources (equal), and writing—review and editing (supporting). Heba Emad El-Gazar: formal analysis (supporting), resources (equal), and writing—review and editing (equal). Mona Metwally El-Sayed: data curation (equal), investigation (supporting), resources (equal), and writing—review and editing (equal). Haitham Khatatbeh: writing—original draft (lead) and resources (equal). Mohamed Ali Zoromba: methodology (supporting), resources (equal), and writing—review and editing (supporting). Amal Diab Ghanem Atalla: writing—original draft (supporting), project administration (supporting), and writing—review and editing (supporting). Rasmieh Alamer: resources (supporting) and writing—review and editing (supporting). Maha Subih: writing—original draft (equal), validation (supporting), and visualization (equal). Annamaria Pakai: conceptualization (equal), methodology (equal), project administration (equal), validation (supporting), visualization (equal), and writing—review and editing (equal).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data would be available upon reasonable request from the principal investigator.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.