
Abstract
Introduction
Workplace social capital (WSC) represents an essential resource for improving nurses’ efficiency and well-being; however, limited attention has been paid to this concept within Iranian healthcare setting.
Objectives
This study explored Iranian clinical nurses’ experiences and perceptions of WSC.
Methods
A qualitative design was used based on conventional content analysis. Data were collected through in-depth, semi-structured interviews with hospital-based nurses selected via purposive sampling. Data analysis was conducted concurrently with data collection following Graneheim and Lundman’s content analysis approach.
Results
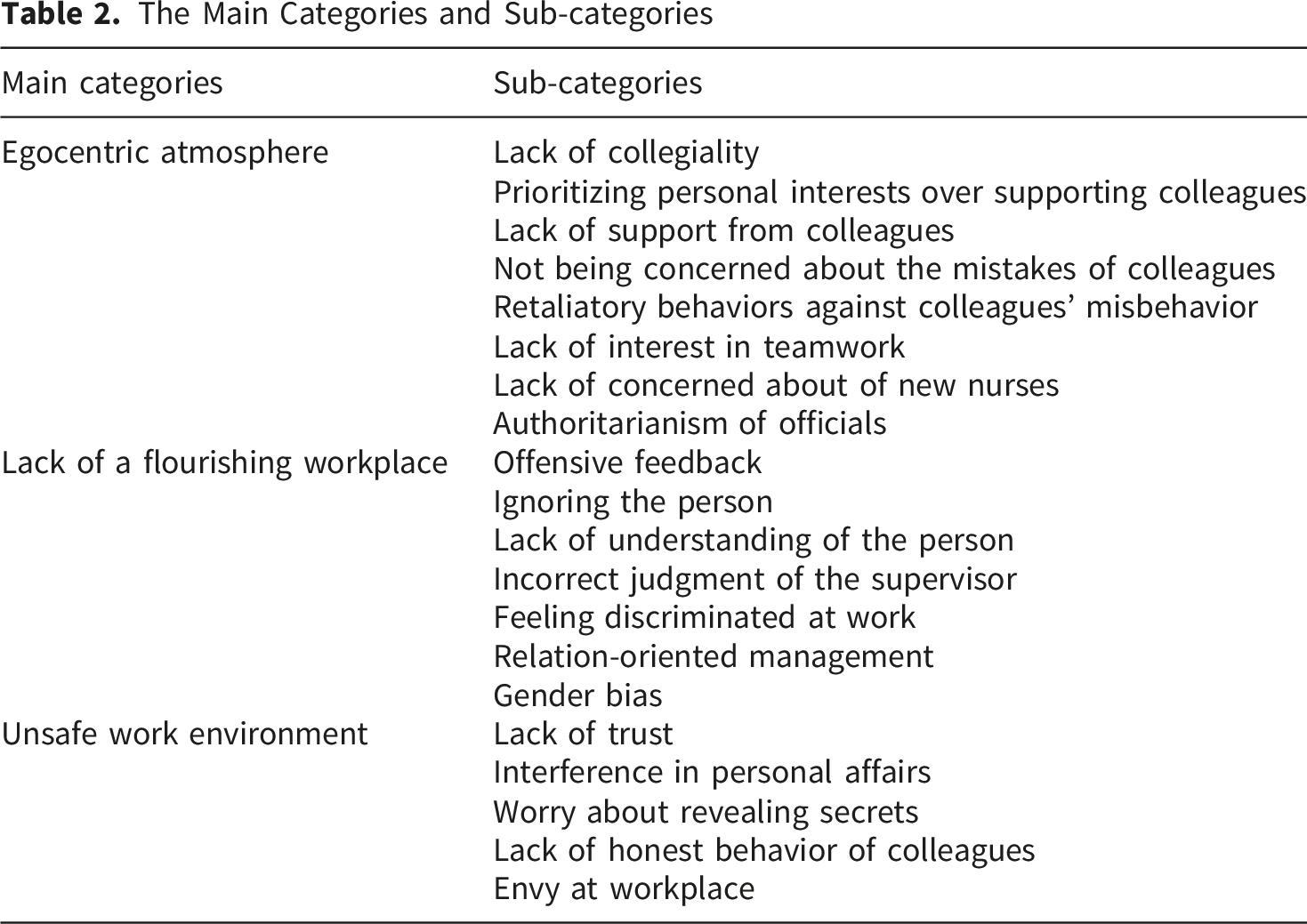
The analysis yielded three main categories: (1) an egocentric atmosphere, (2) lack of a flourishing workplace, and (3) an unsafe work environment, each with its respective subcategories.
Conclusion
The findings provide valuable insights for nursing policymakers and managers aiming to strengthen nurses’ workplace social capital. Key recommendations include promoting teamwork, fair performance appraisals, equitable career advancement, and a stronger ethical climate.
Introduction
Social capital, defined as the strength of an individual's social network and community, has been recognized as a potential determinant of outcomes across various domains, including education and health (Tsounis et al., 2023). It encompasses the social organization of trust, norms, and networks that benefit society at large (Materne et al., 2017). Workplace social capital (WSC), which refers to the relational network formed through respectful interactions among members of a workforce, plays a crucial role in shaping a positive psychological work environment within an organization (J. M. Xu et al., 2022).
Although WSC is intangible, it serves as a significant resource that can enhance the effectiveness and productivity of a workforce (Kida et al., 2021). It acts as a powerful force in attracting employees who are part of the relational network and fosters their interactions, thereby contributing to the development of a healthy and productive workforce (Zhang et al., 2022).
Promoting WSC by establishing connections and nurturing relationships is essential for fostering shared knowledge in clinical settings (Materne et al., 2017). In nursing, effective communication and positive leadership have been identified as key antecedents for the cultivation of WSC (Hossain et al., 2023).
Review of Literature
Previous studies have indicated that WSC offers numerous benefits, such as enhancing the health status of nursing professionals and promoting quality and safety in healthcare delivery. Furthermore, these positive effects can extend beyond nursing professionals to other stakeholders in the healthcare system (Norikoshi et al., 2020; Xu & Stark, 2021).
Nurses’ WSC can be examined from three perspectives: (a) Type, including bonding, bridging, and linking; (b) Component, encompassing structural and cognitive aspects; and (c) Level, which involves group and individual dimensions. Bonding and bridging refer to horizontal relationships, while linking pertains to vertical relationships. Structural social capital refers to the arrangement of the relational network, while cognitive social capital denotes the resources embedded within the network. Nurses’ WSC can be categorized into individual and group levels (J. Xu et al., 2020).
Effective leadership, communication, and trust are commonly recognized as precursors to nurses’ WSC (Kizuki & Fujiwara, 2020). However, challenges persist in understanding how these fundamental elements are implemented and maintained in clinical settings (Pattussi et al., 2016). Therefore, it is imperative to address nurses’ WSC and explore strategies to enhance it.
Despite existing research on nurses’ WSC in international literature (Kida et al., 2021; Kizuki & Fujiwara, 2020; Norikoshi et al., 2020; Xu et al., 2020; Xu & Stark, 2021), little attention has been given to this phenomenon among Iranian nurses. Findings from studies conducted in Western contexts may not be applicable to a distinct cultural setting like Iran.
Studying nurses’ encounters with WSC is crucial as it provides insights into their perceptions of interactions in the work setting. Such exploration helps identify areas requiring improvement within nursing teams. By examining nurses’ experiences with WSC, nurse managers can design strategies to enhance the overall work environment atmosphere.
Given that WSC is relatively understudied in Iran, qualitative research is an appropriate methodology for delving into and gaining a deeper understanding of real-world issues concerning WSC. Qualitative methods allow researchers to uncover the behaviors, perspectives, emotions, and experiences of individuals, groups, and cultures, with the aim of comprehending their social realities (Hassanian et al., 2018). Hence, a qualitative research design using conventional content analysis was utilized to investigate the experiences of a sample of Iranian clinical nurses regarding WSC. Although workplace social capital has been widely studied in Western contexts, its conceptualization and manifestation may differ in non-Western cultures such as Iran. This study contributes context-specific insights that can inform culturally sensitive management practices.
Methods
Design
In this study, a qualitative descriptive research design was applied using a conventional content analysis approach. In conventional content analysis, the researcher does not use preconceived categories because existing theory or literature is limited (Kleinheksel et al., 2020).
Research Question
How do Iranian clinical nurses perceive and describe workplace social capital in their professional environment?
Sample
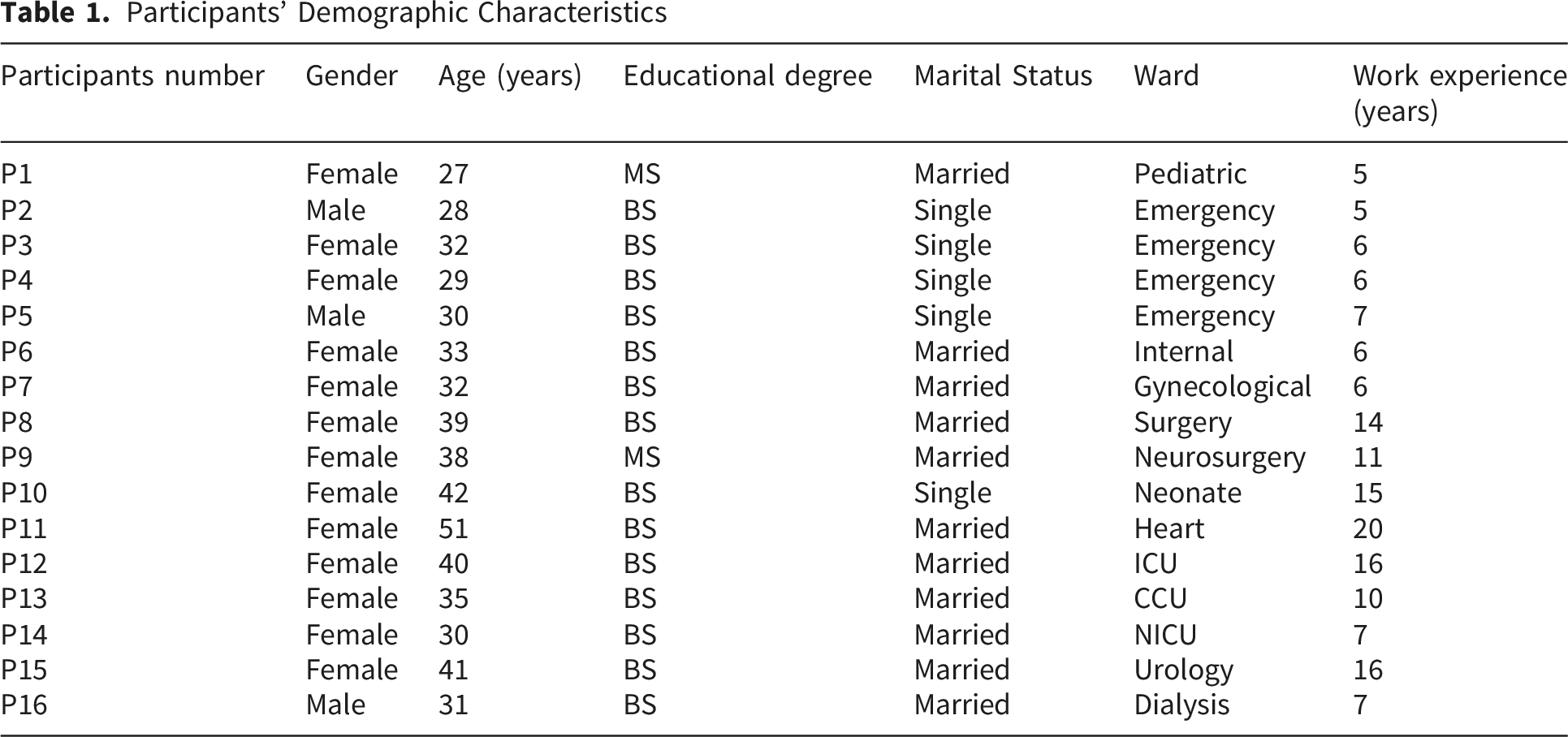
In this study, purposive sampling with maximum variation in terms of age, sex, job tenure, and type of ward was used to ensure a comprehensive representation of different nurses’ perspectives.
Inclusion/Exclusion Criteria
The inclusion criteria were: 1) willingness to participate in the study; 2) having at least a bachelor’s degree in nursing; 3) not having a managerial position, and 4) having a minimum of 3 years of clinical experience. It is worth noting that this study, nurses in managerial positions were excluded in order to focus on exploring the experiences of clinical nurses. This decision was made to ensure that the perspectives gathered were representative of the general experiences of clinical nurses, rather than potentially skewed by the possibly extreme perspectives of managers. Furthermore, nurses with less than three years of clinical experience, those without a bachelor’s degree in nursing, and individuals unwilling or unable to participate due to time constraints or personal reasons were also excluded. In this study, the researchers invited 19 clinical nurses to participate in interviews. Three of the nurses declined to participate citing their busy schedules. Therefore, 16 participants were interviewed.
Institutional Review Board Approval
This study was approved by the Institutional Review Board (IRB) of Birjand University of Medical Sciences, under the ethics code [code no. IR. BUMS. REC.1402.113).]. All procedures were conducted in accordance with the ethical standards of the institutional research committee and the Declaration of Helsinki.
Informed Consent
Prior to data collection, the participants were informed about the purpose of the study, the voluntary nature of their participation, and their right to withdraw at any time without any consequences. Confidentiality and anonymity were assured, and written informed consent was obtained from all participants before conducting the interviews.
Qualitative Data Analysis
Data were collected between February 2023 and February 2024. Data were collected through individual, face-to-face and unstructured interviews, conducted in a quiet and private location, such as a room in the working ward. After warm-up questions like “Please introduce yourself” or “Please tell me about the experience of one working day” the participants were asked to describe their experiences regarding connections and networks within their hospital as well as the supports they receive through these networks. Next, the interview was followed up with exploratory questions based on the experiences expressed by the participants. These questions were asked to obtain deeper information and clarify the meaning of experiences presented by the participants. Examples of such questions included: “Please make this clearer”, “Can you give an example in this case?”, and “What did you mean by …”. To further enrich the interview, the participants were allowed to raise any topic that they personally considered important The duration of the interviews ranged between 60 to 90 minutes. All interviews were audio-recorded with the participant’s consent and later transcribed. The interview transcripts were read several times by the researchers to get a general understanding of the participants. Then, these interviews were compiled in a Word file along with non-verbal field notes about non-verbal cues such as laughter, pauses, and sighs. The transcribed interviews were entered into the MAXQDA 2020 qualitative analysis software. In the present study, the qualitative content analysis method of Graneheim and Lundman (2020) was used to analyze the collected data. Following this approach, the researchers read the interviews and field notes several times to get a general understanding of the participants’ experiences. At the next step, meaning units were determined for different parts of the transcribed interviews. Then, condensation of meaning units was done, during which the text corresponding to meaning units was shortened while preserving the meaning. Then, each of the condensed meaning units was labeled with a code. Next, the codes were grouped into subcategories based on their semantic similarities and differences. Then, the sub-categories that correspond to a common concept were then determined as categories (Lindgren et al., 2020). The criteria proposed by Lincoln and Guba, including credibility, dependability, transferability, and confirmability were used to evaluate the rigor of this study (Lincoln & Guba, 1985). In the present study, audit trail helped to increase the credibility of the study. In this regard, all the decisions and discussions made during data collection and analysis were documented. Also, for member checking, three transcribed and coded interviews were returned to the participants and their feedback was taken into consideration by the research team and the necessary corrections were made. Furthermore, the authors conducted peer checking on coding of transcribed interviews and emerged categories with the assistance of a PhD candidate in nursing and a nursing faculty member from the Nursing and Midwifery College. To ensure the confirmability, the researchers used reflective notes. These notes helped the researchers to avoid personal biases throughout the data collection and analysis stages. Also, to establish confirmability, coding of the transcribed interviews was done by the researcher (first author) and all the codes were assessed by all authors in this study. This process continued until a consensus was reached. Taking into account the transferability, the researchers’ rich description of the participants, the process of selecting the participants, their characteristics and the description of the research context were considered. Given that all participants were recruited from a single city, the transferability of findings may be limited to similar cultural and organizational contexts.
Results
Sample Characteristics
Participants’ Demographic Characteristics
Research Question Results
The Main Categories and Sub-categories
Egocentric Atmosphere
The majority of participants complained about the existence of a work environment where colleagues and supervisors did not understand their perspectives and concerns, nor were they willing to collaborate. In this regard, one nurse described her experience of the lack of cooperation among colleagues as follows: “During one shift, my patient became critically ill, but I remember none of my colleagues helped me. When I protested, they said, ‘It’s your patient; you should do their work yourself.’... Some colleagues are really like this—if someone else’s patient becomes critically ill, they won't touch them, saying, ‘It’s not my patient.’…”, (Participant 1).
Nurses believed that, in most cases, colleagues prioritized their personal interests while supporting and collaborating with others were not their priority. One participant stated: “I feel like their own interests are the priority. Of course, this applies to everyone. Obviously, my personal interests are a top priority for me too, but I try, if I’m close to someone, to support them no matter the situation. But my colleagues aren’t like this’, (Participant 5).
Additionally, nurses expressed dissatisfaction by the lack of collective solidarity. One nurse shared her following experience: “Unlike doctors, nurses don’t support each other.... I had a pediatric patient who suddenly experienced respiratory distress... Even though I wasn't at fault, the head nurse blamed me.... My colleagues, despite being aware of the situation, didn't support me.... This upset me for a long time, even when I went home, I kept thinking about it”, (Participant 6).
Participants emphasized that patient care is a team process and its outcomes are not the result of individual nurses’ efforts, yet they stated that their colleagues were indifferent to others’ mistakes. One nurse remarked: “...Whenever I try to openly talk about the mistakes that happen during my shift, my colleagues don’t help me prevent errors but instead often pretend they've never made such a mistake in nursing”, (Participant 9).
Intolerance emerged as another sub-category in the data analysis. Instead of trying to address annoying behaviors of their colleagues, participants tended to resort to retaliatory actions. One participant’s experience reflected this sub-category: “If I see my colleague isn't helping much in the ward, I also limit my work to the same extent. Or if they take a couple of hours off, I try to leave earlier with some excuse... So they understand how rude and bothersome their behavior is”, (P14). Another nurse shared: “Our ward supervisor schedules tougher shifts for nurses who don't have good relations with them or have conflicts. Those who are on good terms with them get lighter shifts”, (P10).
When nurses shared their experiences of starting their nursing career in the current ward, one of the distressing experiences was the lack of guidance and support from experienced nurses. According to participants’ experiences, supporting new nurses was not a concern for experienced nurses and they preferred to focus on their own advancement. One nurse commented: “When I started working in the pediatric ward, since I lacked experience, I sometimes made mistakes or wasn't fully proficient in procedures... One time, I forgot to include a nursing diagnosis in the report, and my experienced colleague said, ‘How clueless are you? Forget it, I’ll fix it myself.’... Teaching me probably wasn’t beneficial for them”, (P12).
Finally, authoritarianism among supervisors was the last sub-category. Participants believed that supervisors showed little concern about their individual or organizational problems. Rather than empowering nurses and giving them decision-making autonomy, supervisors aimed to exert power and impose their personal preferences, with decisions in the hospital typically being made unilaterally by supervisors. One participant stated: “The hospital director is entirely in their own world and takes care of their own interests and benefit... They reduce the number of staff, and when we protest, saying there should be more staff on shifts, they don't listen at all.... I think the problems of nurses and other hospital staff don't matter to them.... We also report our problems to the head nurse, but they prefer not to get involved in these issues... They seem to be more supportive of them”, (P16).
Lack of a Flourishing Workplace
Participants believed that the feedback they received from colleagues, doctors, and supervisors in the workplace was insulting and caused them distress. One participant shared: “The hospital director is also the physician of my department... He came to visit his patients... I was talking to him, and the ward supervisor was present too. The hospital director asked why I wanted to leave this department. I said that my mental health was deteriorating here, and my colleagues were making me upset... The supervisor spoke to me in an insulting tone right there, saying, ‘Well, if you can manage to leave, then go”, (Participant 1).
Additionally, nurses acknowledged that despite their significant efforts, their hard work was overlooked and unappreciated. One nurse stated: “For example, a nurse works hard all night, but then the morning supervisor comes and nitpicks over every little thing. This isn't right... I don’t think this behavior towards me is fair, especially in front of patients or other colleagues...”, (P 13).
Nurses expressed dissatisfaction with not being understood in the workplace by colleagues and supervisors. One nurse shared: “Whenever there are staff shortages in shifts, they assign us saying, ‘You’re single and don’t have responsibilities.’... They don’t care about our interests or issues as singles. Whenever there’s a problem for others, they assign those shifts to us. They don't see our problems... Just like other employees, we should be able to pursue our interests outside the workplace”, (P 4).
Furthermore, nurses mentioned that they are often subjected to unfair and inappropriate judgments. One nurse recounted their experience: “If a mistake happens in the ward, because I’m younger than my colleagues, the error is attributed to me. While most of the tasks in the ward should be done by those with less work experience. But if they make a mistake, their error is considered major by colleagues and completely unforgivable”, (Participant 3).
Regarding the experiences of discrimination among nurses by supervisors, one nurse said: “For instance, you put your all into your work in the ward... But you see that you’re still being criticized, or a nurse with more experience or seniority, even though they work less, their opinions are more valued. Even if they make a mistake, nothing is said to them, but the blame is placed on you”, (P 11).
Nurses believed that in their workplace, informal connections held more significance than organizational regulations. One nurse commented: “Unfortunately, that’s not how it works here... Relationships take precedence. If you have good connections with the supervisors, you’re fine. If not, you won’t have any career advancement and will just stay stuck”, (P 2).
In the present study, many female nurses reported experiences of biased attitudes and behaviors from colleagues and supervisors. One participant recounted: “Some male colleagues don’t cooperate much in ward tasks... When you ask them to do something, they say they’ll do it later, or they complete the task reluctantly or with delays. When you report this to the supervisor, the female supervisor remains silent and doesn’t address it. One of our female colleagues started her internship six months ago and hadn’t fully adjusted yet... She tried hard to be good at her work. Despite this, the supervisor would constantly criticize her and find faults with her”, (Participant 1). Another participant stated: “For example, in our hospital, most managerial positions are given to men instead of women, even though women have both the capability and strength for such roles. There’s always resistance against women taking organizational positions”, (Participant 10).
Unsafe Work Environment
According to the nurses participating in the study, due to the lack of trust among colleagues, they were unwilling to establish intra-organizational or external relationships with their peers in the workplace. One of them mentioned: “I have no interaction with any of my colleagues outside the hospital, and I don’t feel close to them. Outside the hospital, I don't feel a sense of closeness with my colleagues... The trust and confidence I should have in them, unfortunately, do not exist... I feel like keeping my distance from them makes me feel more comfortable”, (Participant 3).
Nurses stated that one reason for keeping their distance and avoiding closeness with colleagues was their interference in personal matters. For example, one nurse said: “Some of our male colleagues meddle unnecessarily. They even interfere in personal matters, like how you dress. These interferences are not pleasant for me. I feel a certain distance should be maintained to minimize such interferences”, (Participant 3).
Nurses expressed dissatisfaction regarding the disclosure of their secrets by colleagues. One nurse shared her experience as follows: “Most of our colleagues are not discreet... We’re not trustworthy... We lack empathy... Anything they hear, they share and spread. I wish even if we can’t help each other, at least by refraining from revealing others' secrets, we wouldn’t add more pain to their hardships”, (Participant 4).
Nurses were also dissatisfied with the dishonesty of colleagues and supervisors. One nurse stated: “Just a couple of months ago, one of my colleagues wanted to take the night shift off and spoke to the supervisor. The supervisor told them, ‘Sure, I’ll give you the night off, but find someone to take your place for this shift.’ My colleague then called me and told me my shift for tonight had been canceled, even though my shift hadn’t been canceled, and they themselves were taking my place. Then they said the supervisor told me to take the next night’s shift, but they never mentioned that the next night's shift was actually their own. Later, I realized they hadn't been honest”, (P 15).
In some cases, participants complained that their colleagues did not acknowledge their successes and discouraged them through their behavior. A nurse shared the following experience: “It was during the early years of the COVID pandemic when I got accepted into a master's program. Most classes were online. We had two young colleagues who constantly said, ‘You’re so lucky your classes are online.’ Eventually, I got upset and said, ‘Well, you could’ve studied and gotten accepted into a master’s program too.’ They replied, ‘What difference will getting a master’s degree make for you”, (P 6).
Discussion
The purpose of this study was to explore nurses’ experiences regarding workplace social capital through a qualitative content analysis of their narratives. The findings revealed three main categories:
The category of
Previous studies have highlighted the detrimental effects of such environments. For example, lack of collegiality and mutual support has been associated with increased isolation, occupational stress, and burnout, particularly in high-stress settings such as hospitals (Johnson & Lee, 2020). This aligns with findings related to insufficient colleague support and indifference toward errors. Nurses frequently report low workplace social capital, poor communication, and limited collaboration, all of which negatively affect job satisfaction and morale.
International evidence supports these findings. Studies conducted in Japan have shown that low levels of trust, reciprocity, and information sharing are associated with reduced workplace social capital and weaker organizational engagement (Matsumoto et al., 2023; Takayama et al., 2017). Similarly, research in Belgium and Australia has demonstrated that poor intra-organizational communication and lack of collaboration contribute to higher burnout, increased turnover intention, and reduced job satisfaction among nurses (Manias et al., 2023; Vandenberghe et al., 2017). In addition, retaliatory behaviors and intolerance toward coworkers have been identified as key contributors to hostile work environments and reduced job satisfaction (Kumar et al., 2018).
From a practical perspective, these findings highlight the importance of fostering a culture of mutual support, empathy, and collaboration in healthcare settings. Addressing egocentric behaviors and promoting collegial relationships can enhance teamwork, reduce conflict, and improve employee well-being. Supportive communication and collaborative practices have been shown to reduce burnout and improve the quality-of-care delivery (Edmondson, 2019; Hakanen et al., 2020; Laschinger & Read, 2016). Interventions such as team-building programs, conflict management training, and supportive leadership development may therefore strengthen workplace social capital.
The category of
Previous studies have confirmed the negative consequences of these factors. Offensive or non-constructive feedback can undermine self-esteem and reduce performance improvement (Brown & Levinson, 2020). Organizational structures with rigid hierarchies and weak leadership support have been linked to feelings of isolation and reduced professional empowerment (Alghamdi & Alharthy, 2022; Bouwmans et al., 2016). Furthermore, lack of recognition significantly decreases organizational commitment and motivation (Lee et al., 2020), while supervisors’ failure to understand employees’ perspectives increases workplace tension and reduces trust in leadership (Thompson & Walker, 2019). Inaccurate evaluations have also been associated with decreased engagement and increased turnover intention (Chen et al., 2018). Discrimination contributes to perceptions of injustice and lower morale (García-González et al., 2021), while gender bias remains a persistent barrier to career advancement and psychological well-being (Peterson & Fauth, 2019).
Additionally, supportive communication and mutual respect have been identified as key factors in developing workplace social capital among nurses (Materne et al., 2017). When these elements are absent, motivation and morale decline, negatively affecting patient care quality.
Collectively, these findings emphasize the critical role of organizational culture and leadership in shaping nurses’ professional experiences. Strategies such as structured communication tools (e.g., SBAR), team-building initiatives, flattening hierarchical structures, and strengthening leadership support may enhance workplace social capital and organizational effectiveness.
The category of
These findings are consistent with the experiences of nurses in the present study. In the Iranian context, such issues may be intensified by cultural norms and hierarchical organizational structures, making the development of trust and psychological safety particularly essential.
The findings highlight the need for interventions aimed at improving workplace environments in healthcare settings. Managers should establish clear boundaries between personal and professional domains, ensure confidentiality, and promote ethical behavior. Transparent evaluation systems, equitable opportunities, and anti-discrimination policies are essential. Leadership training focused on trust-building, conflict management, and ethical decision-making is also critical.
Overall, the identified categories reflect negative experiences of Iranian nurses regarding workplace social capital; however, they also indicate opportunities for organizational improvement. Future studies should evaluate the effectiveness of targeted interventions in improving workplace social capital. Culturally sensitive strategies, including inclusive leadership, gender-sensitive policies, and mentorship programs, may further enhance nurses’ professional experiences.
Strengths and Limitations
To date, relatively few studies have explored Iranian clinical nurses’ experiences of workplace social capital (WSC). Examining WSC within a specific cultural context, such as the Iranian healthcare system, contributes to the enrichment and diversification of the international literature. The use of a qualitative design enabled an in-depth exploration of nurses’ lived experiences of WSC, which may not be fully captured through quantitative approaches. In addition, purposive sampling with maximum variation enhanced the diversity of perspectives and strengthened the rigor of the findings.
Despite these strengths, several limitations should be considered when interpreting the results. The study was conducted within a single regional and cultural context, which may influence participants’ experiences and limit the transferability of the findings to other settings. Moreover, the use of purposive sampling and the relatively small sample size, although appropriate for qualitative content analysis, may not fully reflect the breadth of nurses’ perspectives. As data were collected through self-reported interviews, the findings may also be subject to recall bias or social desirability bias.
Implications for Practice
This study underscores the significant challenges Iranian clinical nurses face concerning workplace social capital, offering valuable insights for nursing policymakers and healthcare managers. To foster a more supportive and effective professional environment, several practical implications emerge:
Firstly, to counteract an egocentric atmosphere, it is recommended that managers actively cultivate a team-oriented culture. This involves shifting the emphasis from individual competition to collective achievement, encouraging collaboration, and recognizing shared successes. Such an approach can help build stronger interpersonal bonds and a sense of unity among nurses.
Secondly, addressing the lack of a flourishing workplace necessitates the establishment of fair and transparent performance appraisal systems and equal opportunities for professional advancement. These measures can enhance a sense of equity and motivation, fostering an environment where nurses feel valued and see clear pathways for growth, thereby contributing to a more vibrant and engaging workplace.
Finally, the transformation of unsafe work environments into healthy and supportive workplaces requires a concerted effort to strengthen the ethical climate, build trust, and enhance psychological safety. Implementing strategies that promote ethical decision-making, ensure confidentiality, and encourage open communication without fear of reprisal are crucial steps in creating an environment where nurses feel secure and supported.
By addressing these key areas, healthcare organizations can significantly enhance workplace social capital, leading to improved nurse experiences, increased job satisfaction, and potentially better patient care outcomes.
Conclusions
This study highlights the significant challenges faced by Iranian nurses regarding workplace social capital. The findings provide valuable insights for nursing policymakers and healthcare managers to enhance social capital in clinical settings.
For example, to address an egocentric atmosphere, managers can foster a team-oriented culture that emphasizes collective achievement over individual competition. To mitigate the lack of a flourishing workplace, the establishment of fair and transparent performance appraisal systems and equal opportunities for professional advancement is recommended. Finally, transforming unsafe work environments into healthy and supportive workplaces requires the implementation of strategies aimed at strengthening ethical climate, trust, and psychological safety.
Supplemental Material
Supplemental Material - Iranian Clinical Nurses’ Experiences of Workplace Social Capital: A Qualitative Content Analysis
Supplemental Material for Iranian Clinical Nurses’ Experiences of Workplace Social Capital: A Qualitative Content Analysis by Mehrangiz Ghabimi, Seyyed Abolfazl Vagharseyyedin in Sage Open Nursing
Footnotes
Acknowledgments
We thank the participants that were involved in the study.
Ethical Considerations
The study was approved by the ethics committee of Birjand University of Medical Sciences (code no. IR. BUMS. REC.1402.113). All the participants were informed about the study’s purpose and method. They were informed that participation in the study was voluntary and that they were allowed to withdraw from the study at any moment without any penalty. Moreover, they were assured that information gathered from them would be kept confidential. Lastly, informed written consent was obtained from those nurses who were willing to participate in the study. l audio recordings and transcripts were stored in encrypted files accessible only to the research team. Participants’ identities were anonymized using coded identifiers.
Author Contributions
Mehrangiz Ghabimi designed the study, collected and analyzed the data, and drafted the manuscript.Seyyed Abolfazal Vagharseyyedin supervised the study, provided methodological and editorial guidance, and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.