
Abstract
Background
Pain assessment is a fundamental aspect of nursing care. Problems in applying pain assessment principles are more severe in low-income countries. This study aimed to assess pain assessment practice and associated factors among nurses working at the adult care unit at a public Hospital in West Hararghe Zone, Eastern Ethiopia, 2023.
Methods
An institution-based cross-sectional study was conducted from July 15 to August 15, 2023, among 394 randomly selected nurses working in adult care units at public hospitals in West Hararghe Zone. A structured self-administered questionnaire and chart review were used for data collection. Pain assessment practice was evaluated using 8 “yes/no” questions, and total scores were computed. Nurses scoring ≥70% were categorized as having adequate practice, while those scoring below 70% were considered to have poor practice. Data was entered into EpiData version 3.1software and exported to the Statistical Package for Social Science (SPSS) version 26 for analysis. Bivariate and multivariable logistic regression were used to identify factors associated with pain assessment practice, with significance interpreted at p-value <0.05.
Results
The overall self-reported pain assessment practice among study participants was found to be 63.5% (95% CI: 59.0% - 68.0%). Work experience of >5 years [AOR: 3.13 (95% CI: 1.21-8.14)], knowledge of pain assessment [AOR: 4.25 (95% CI: 2.51-7.18)], attitude towards pain assessment [AOR: 3.43 (95% CI: 2.05-5.72)], and having in-service training on pain assessment [AOR: 3.58 (95% CI: 1.05-12.23) were significantly associated with pain assessment practices.
Conclusion
The study revealed that a moderate level of pain assessment practice was reported among participants, indicating room for improvement in clinical settings. Work experience, knowledge, positive attitudes toward pain assessment, and in-service training are significantly associated with pain assessment practice. These findings highlight the importance of enhancing healthcare workers’ knowledge, attitudes, and training programs to improve pain assessment practices.
Introduction
Pain is always a uniquely individual response that is to varying degrees influenced by biological, psychological, and social factors, whereas all people feel pain at some time in their life as a subjective reaction to biological and psychological pressures (Rajaa S.N et al., 2020). Globally, hospital-wide pain prevalence obtained ranged from 37.7 to 84%, and severe pain prevalence ranged from 9-36% (Gregory & McGowan, 2016). According to the evidence, one of the main reasons patients seek medical care is pain (Cox, 2018; Onianwa et al., 2017).
Emerging literature highlights that assessment is not merely a preliminary step but a fundamental component of comprehensive pain management (Eull et al., 2023). Pain that is not assessed or treated by nurses can have a debilitating effect and can significantly impact a patient’s quality of life by significantly impacting their physical, emotional, and mental health, causing uncontrollable pain, delaying healing, increasing the risk of several complications, and prolonging stay in the Hospitals (Belay Bizuneh et al., 2020; Kotfis et al., 2018).
Nurses are in a unique position to support patients who are experiencing pain and play a vital role in providing pain assessment and management (Cox, 2018; Samarkandi, 2018). While utilizing assessment methods and tools, nurses should take the pain assessment concepts into mind (I. Kizza & Muliira, 2015). Subjective data, objective data, and evaluation tools are all necessary for a comprehensive pain assessment (Melile Mengesha et al., 2022). Behavioral observations, such as facial expressions and movements, are also considered, while changes in vital signs may provide supportive cues, but are not reliable indicators of pain assessment (Gélinas, 2016).
According to the most recent study and quality improvement initiatives, nurses should incorporate pain assessment tools into their routine practice (Puntillo, 2016). Standardized pain assessment tools/scales are available for different patient groups, which enhance communication by promoting consistency and making a subjective experience measurable (Das et al., 2020; I. B. Kizza et al., 2016). The right tool should be selected; if patients are unable to communicate, tools may involve a review of a critical ill pain observation tool (CPOT) and the behavioral pain scale (BPS), which are valid and reliable tools (Pasero & Herr, 2015; Thompson et al., 2017). Pain scales for patients able to communicate include a Visual Analogue scale (VAS), a 0-10 Numerical Rating Scale (NRS), and a Verbal Rating Scale (VRS), which are valid and reliable tools (Edra F, 2016). There are additional interview methods available to gather a complete pain history, including location, onset, nature, radiation, associated factors, aggravating or relieving factors, and intensity (Breivik et al., 2008). Salivary biomarkers, such as cortisol and alpha amylase, are gaining recognition as promising noninvasive tools for pain assessment, offering valuable insight into pain perception and physiological stress response (Sobas et al., 2020; Stendelyte et al., 2023).
Review of Literature
In Rwanda, 20% of nurses had a good practice pain assessment (Umuhoza, 2017), in Addis Ababa, 55.9% did, and only 17.74 % of them used tools routinely (Ayenew et al., 2021). Overall, pain-assessment remains poor across settings due to a lack of guidelines and tools, high workload, limited experience and training, unfamiliarity with assessment instruments, and weak organizational support (Ayenew et al., 2021; Gélinas, 2016).
Most studies in Ethiopia focus on pain management practices among nurses and associated factors. However, a recent systematic review and meta-analysis reported that only about 48% of nurses demonstrated adequate pain management practice, underscoring the inconsistency and gaps in clinical practice nationwide (Munie et al., 2025). By contrast, the present study investigates pain assessment practice among nurses working in medical and surgical wards in Eastern Ethiopia, a region where empirical evidence is scarce. Importantly, this study incorporates organizational and patient-related factors alongside knowledge, attitude, and practice domains, and uniquely integrates chart review to capture documented evidence of pain assessment. Chart review is an objective way to assess nurses’ documentation and adherence to pain assessment protocols, capturing practice patterns such as assessment frequency, use of standardized tools, and intervention records. Nevertheless, there is still a significant gap between past study findings and current realities in clinical practice. This study aimed to assess pain assessment practice and associated factors among nurses working at the adult care unit at a public Hospital in West Hararghe Zone, Eastern Ethiopia.
Methods and Material
Study Design
An institution-based cross-sectional study design was used.
Study Setting and Period
This study was conducted in the public hospitals of the West Hararge Zone, Eastern Ethiopia. West Hararge Zone is one of the 20th zones in the Oromia region, which is located in Eastern Ethiopia. Administratively, West Hararge Zone is subdivided into 15 districts and 5 rural towns. Chiro town serves as the capital of the West Hararge Zone administration. According to the 2007 Ethiopian Census projection for 2020/2021, the Zone has an estimated total population of 2,667,000 (CSA & International, 2012).
There are seven public hospitals, 80 health centers, 44 private clinics, and 446 health posts in the zone. The total number of nurses working at adult care units of each hospital was 550. Two general Hospitals provide a multidimensional aspect of care to patients who need highly qualified/specialized healthcare services, and the remaining five hospitals provide inpatient, outpatient, emergency, and delivery services. (Source: West Hararge Zonal Health Bureau Office). The study was carried out from July 15 to August 15, 2023.
Population
Source Population
All nurses working in the adult care unit in public hospitals in West Hararge Zone.
Study Population
All nurses working in the adult care unit of public hospitals in West Hararge Zone during the data collection period.
Eligibility Criteria
The study included all nurses working in adult care units. Nurses who were present during the data collection period and had been working in these units for at least six months were included.
Sample Size Determination
A single population proportion formula was used to calculate the sample size by using the following assumptions: the proportion of good nurses’ pain assessment practice was found to be 38.2% in Wolaita Zone, Southern Ethiopia (Melile Mengesha et al., 2022), with a margin of error of 5%, 95% confidence interval, and a 10% non-response rate. The final sample size of 400 is yielded.
Sampling Procedure and Sampling Technique
All seven hospitals in the West Hararge Zonal Administration were included in this study. The total number of nurses working at adult care units of each hospital was considered to proportionally allocate the sample size for each hospital. Following the proportional allocation of sample size to each hospital, study participants were selected using a simple random sampling technique (Figure 1). Schematic presentation of sampling procedure to assess pain assessment practice and associated factors among nurses working at adult care unit in public hospital in West Hararge Zone, Eastern Ethiopia, 2023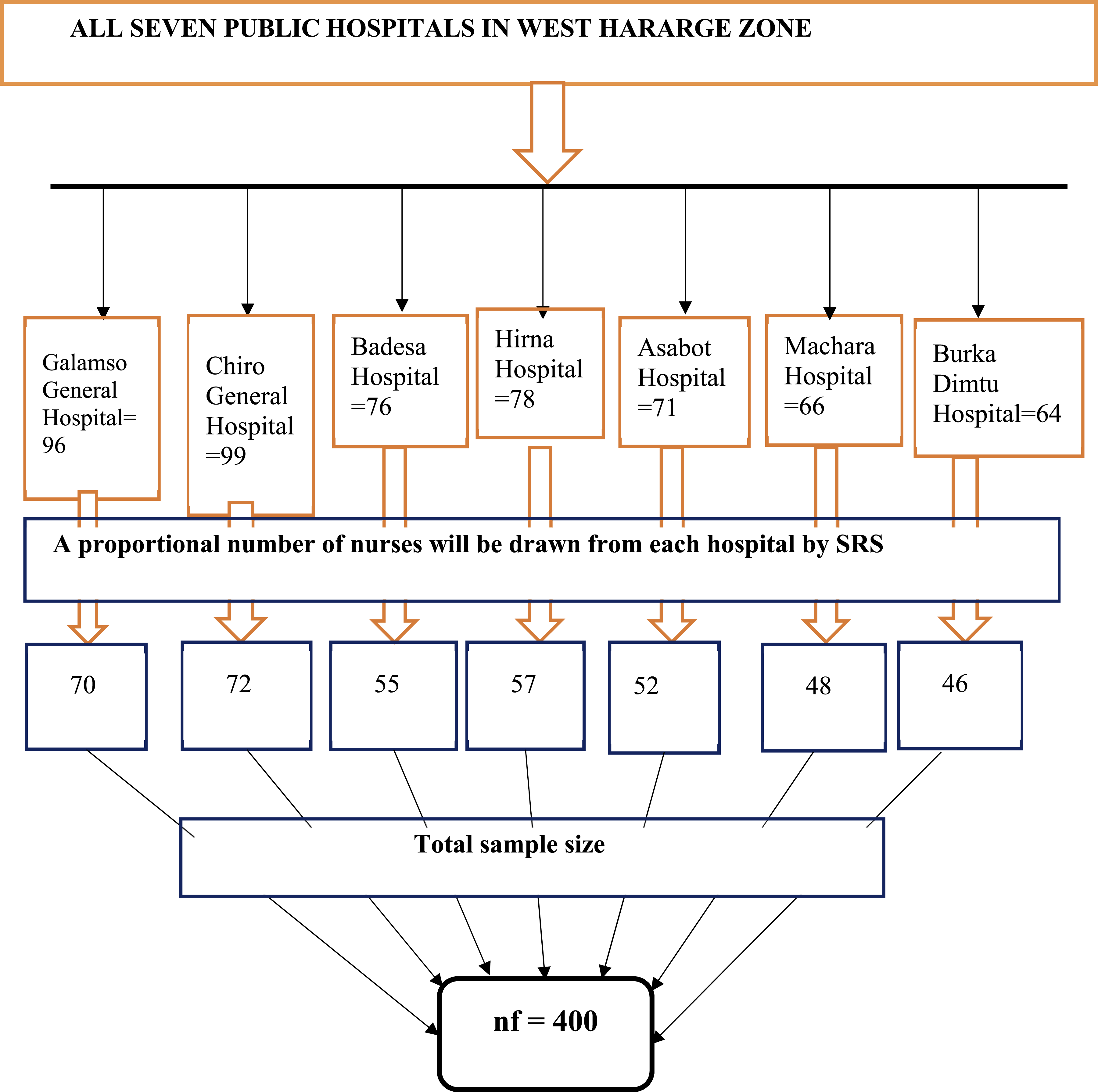
Data Collection Tools and Procedures
Data were collected using a pretested, structured, self-administered questionnaire and checklist. The data collection tool for the self-administered questionnaire was developed by reviewing different literature (Ayenew et al., 2021; Liyew, Dejen Tilahun, & Habtie Bayu, 2020; Melile Mengesha et al., 2022; Negese et al., 2020). The questionnaire contains six parts: sociodemographic information, knowledge-related questions, practice-related questions, attitude-related questions, organization-related factors, and patient-related factors.
The questionnaire was adapted from previously validated instruments used in similar studies. Content validity was established through expert review by senior nursing faculty and public health professionals, who assessed the relevance and clarity of each item. Reliability was tested during the pre-test phase on a sample of nurses outside the study area. Internal consistency was confirmed using Cronbach’s alpha, which demonstrated acceptable reliability across all domains: knowledge (α = 0.82), attitude (α = 0.79), and practice (α = 0.84).
Chart Review Checklist
A structured and pre-tested English version standard checklist was adopted from different reviewed literature and the Health Sector Transformation in pain guidelines (Angeletti et al., 2018; Ortiz et al., 2014; Rajaa S.N et al., 2020) to collect data regarding nurses’ pain assessment practice through chart review. The checklist contained 11 items with “Yes” and “No” responses.
Study Variables
Dependent Variable
The dependent variable in this study was nurses’ pain assessment practice.
Independent Variables
Age, sex, marital status, educational level, work experience, presence of protocols and guidelines, availability of standardized tools, perceived organizational support, working unit, training on pain management, knowledge, attitude, nurse workload, and patient-related factors such as patients unable to self-report and patients’ instability.
Operational Definition of Terms
Knowledge of Nurses
It was measured using 10 “yes/no” questions, and the total scores were computed. Nurses who correctly answered above or equal to 70% of knowledge questions are considered to have adequate knowledge on pain assessment in the adult care unit, and those who correctly answered below 70% of knowledge questions are deemed to have inadequate knowledge (Ayenew et al., 2021).
Attitude of Nurse
It was measured using 7 “yes/no” questions, and the total scores were computed. Nurses who scored 70% and above on attitude-related questions were considered to have a favorable attitude, but, on the contrary, those who answered below 70% were considered to have an unfavorable attitude (Liyew et al., 2020).
Good Practice
The measurement was conducted using 8 “yes/no” questions, and the total scores were calculated. Nurses who correctly answered above or equal to 70% of practice questions were considered to have adequate practice on pain assessment in adult care unit patients, but on the contrary, those who correctly answered below 70% were considered to have poor practice (Melile Mengesha et al., 2022).
Nurse Workload
If one nurse provides for more than six patients in inpatient service other than ICU and emergency per shift, it is considered nurse work overload (Fekede et al., 2023).
Patient Instability
Those patients with a clinical presentation of either an altered level of consciousness, systolic BP < 90 mmHg, shortness of breath, pulse rate > 120 bpm, pulmonary edema, and poor skin sign (Haregeweyn Kibret et al., 2022).
Data Quality Assurance and Management
The study involved a structured questionnaire prepared in English. Before the actual one-week data collection, the items were tested on 20 (5 % of 400) nurses working out of the study area (Chelanko Hospital), and the result was used to check the clarity and completeness of the questionnaire, and any ambiguities or differences in understanding were revised. Each questionnaire was coded with a unique identification number. Data collectors and supervisors received adequate training on the study’s objectives, data collection methods, ethical considerations, and the impact of data on participants. Regular meetings were held between data collectors, supervisors, and the principal investigator to address any issues arising from respondents. Data was kept in a secure shelf to protect against unauthorized access, loss, and tampering while ensuring confidentiality by not recording personal identities.
Data Processing and Analysis
After data collection, the data were coded, checked, cleaned, and entered into EpiData version 3.1 Software and then exported to SPSS version 26 for analysis and interpretation. Descriptive statistical analysis, such as simple frequencies, measures of central tendency, and measures of variation, was computed to summarize and describe the characteristics of study participants, and the information was presented using frequencies, summary measures, graphs, tables, and figures. Bivariate analysis was used to assess the association between independent and outcome variables using binary logistic regression. Independent variables with a p-value of < 0.25 at 95% CI in bi-variable analysis were retained for multivariable logistic regression analysis. AOR with 95% CI was estimated to show the relationship between the independent variables and the dependent variable after controlling for the effects of confounders with 95% CI. Variables with a P-value ≤ 0.05 were declared as having a statistically significant association with the outcome variable.
Ethical Considerations and Informed Consent Statements
This study was approved by the Institutional Health Research Ethics Review Committee. Letters of cooperation were obtained from each participating hospital to facilitate the conduct of the research. Written informed consent was secured from all study participants after providing an adequate explanation of the study’s purpose, procedures, potential risks, and anticipated benefits. Participants were assured of their right to withdraw at any stage without consequence, and confidentiality was strictly maintained by anonymizing responses and restricting data access to the research team. The study adhered to the principles of the Declaration of Helsinki and national research ethics guidelines.
Results
Socio-Demographic Characteristics of Nurses
Socio-Demographic Characteristics of Nurses Working at Adult Care Units in Public Hospitals, West Hararge Zone, Eastern Ethiopia, 2023 (n=394)

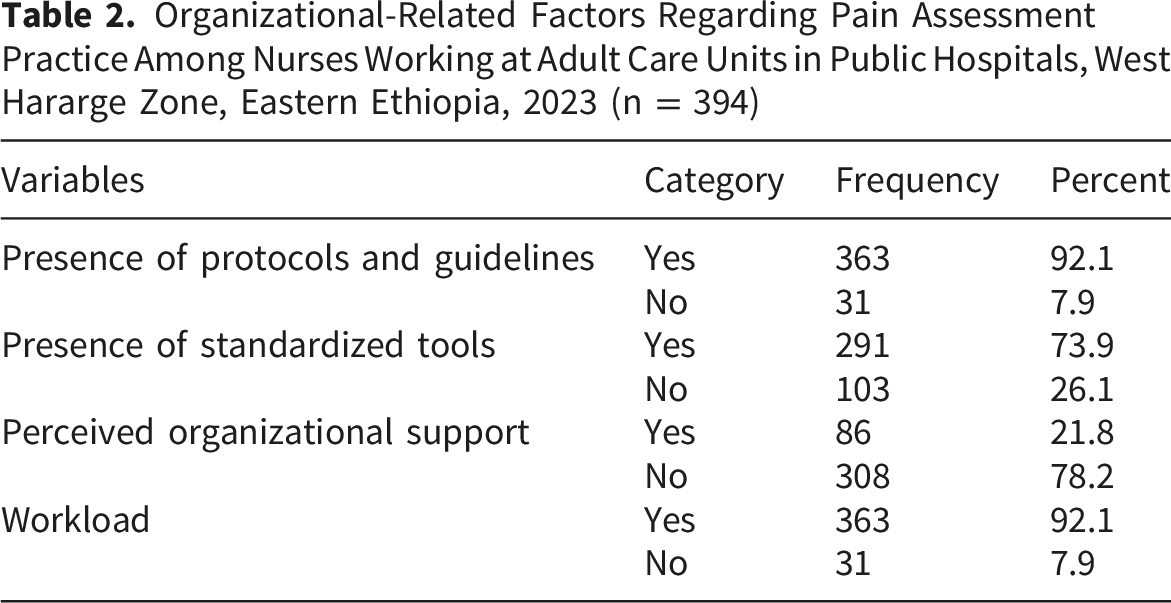
Organizational Related Factors
Organizational-Related Factors Regarding Pain Assessment Practice Among Nurses Working at Adult Care Units in Public Hospitals, West Hararge Zone, Eastern Ethiopia, 2023 (n = 394)
Knowledge of Nurses About Pain Assessment
Knowledge of Nurses Regarding Pain Assessment Among Nurses Working at Adult Care Units in Public Hospitals, West Hararge Zone, Eastern Ethiopia, 2023 (n = 394)

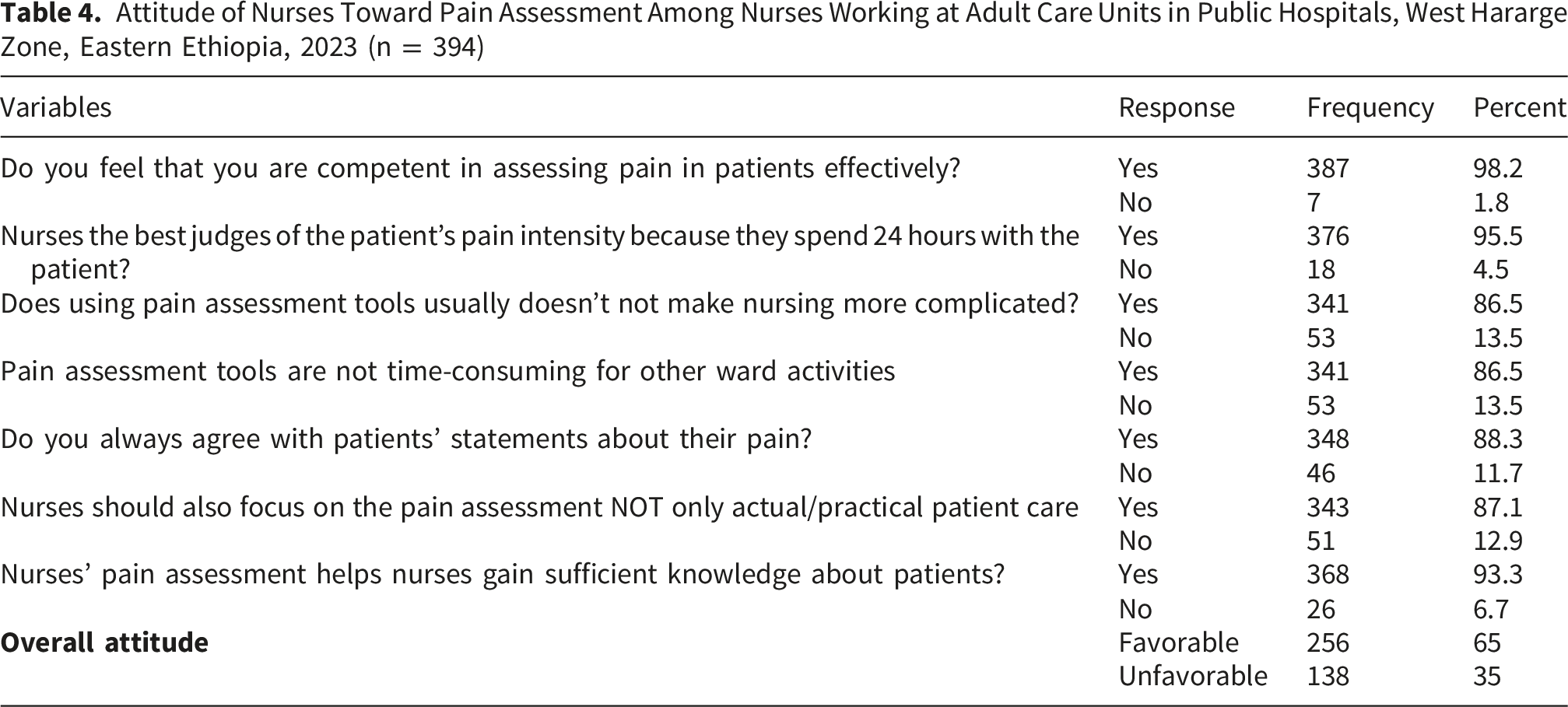
Attitude of Nurses Toward Pain Assessment
Attitude of Nurses Toward Pain Assessment Among Nurses Working at Adult Care Units in Public Hospitals, West Hararge Zone, Eastern Ethiopia, 2023 (n = 394)
Patient-Related Factors Impacting Pain Assessment Practice
The majority of nurses 90.6%, reported that patient self-reporting influences their ability to quantify pain, whereas 9.4% indicated that it does not. Additionally, 91.4% of nurses believe patient instability affects their pain assessment, while only 8.6% claim it doesn’t.
Nurses’ Pain Assessment Practice
Pain Assessment Practice Among Nurses Working at Adult Care Units in Public Hospitals, West Hararge Zone, Eastern Ethiopia, 2023 (n = 394)

Results From the Chart Review
Checklist on Pain Assessment Practice and Associated Factors Among Nurses Working at Adult Care Units in Public Hospitals, West Hararge Zone, Eastern Ethiopia, 2023 (n=394)

Factors Affecting Pain Assessment Practice Among Nurses Working in Adult Care Units
In the bivariable analysis, age, work experience greater than five years, availability of standardized tools, organizational support, nursing workload, having in-service training on pain assessment, patient instability, absence of protocols or guidelines, patient inability to self-report, patient pain and distress, nurses’ knowledge, and nurses’ attitude were identified. Finally, multivariable regression analysis showed that work experience >5 years, nurses’ knowledge, nurses’ attitude, and in-service training on pain assessment were significantly associated with nurses’ pain assessment practice in the adult care unit.
Bivariate and Multivariate Analysis on Factors Associated With Nurses’ Pain Assessment Practice Among Nurses Working at Adult Care Units in Public Hospitals, West Hararge Zone, Eastern Ethiopia, 2023 (n=394)
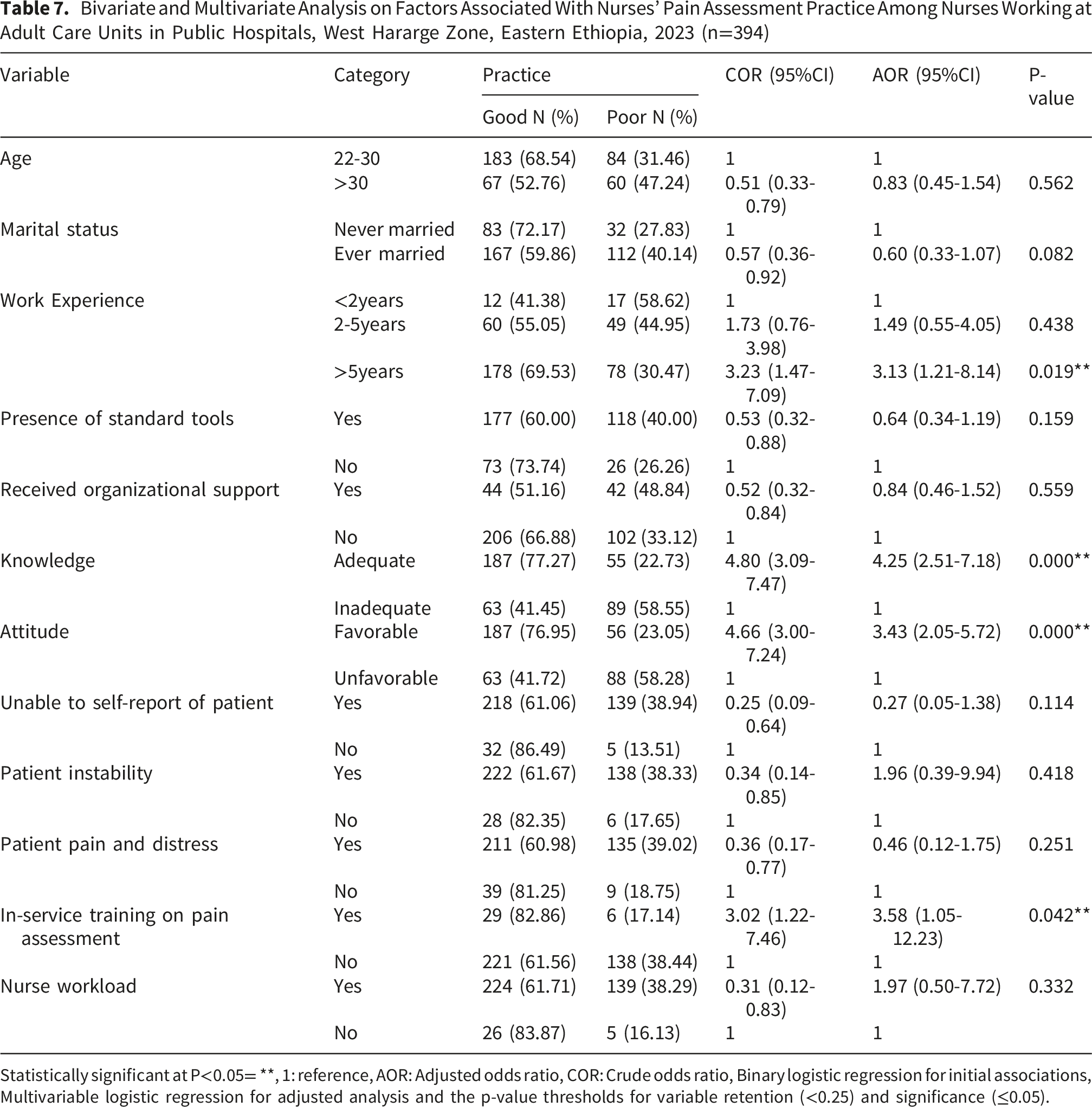
Statistically significant at P<0.05= **, 1: reference, AOR: Adjusted odds ratio, COR: Crude odds ratio, Binary logistic regression for initial associations, Multivariable logistic regression for adjusted analysis and the p-value thresholds for variable retention (<0.25) and significance (≤0.05).
Discussion
This cross-sectional study was conducted to evaluate nursing pain assessment practices and identify factors influencing these practices among nurses working in the adult care unit of a public hospital in the West Hararge Zone, Ethiopia. Based on the study findings, nearly all nurses (98.5%) reported engaging in pain assessment practices. Upon reviewing the charts, it was found that a pain assessment tool was attached in just 81.8% of cases. Even though the findings from the self-administered questionnaire and the reviewed chart support each other, the magnitude of pain assessment practice from the result of the self-administered questionnaire was higher than the magnitude of pain assessment practice from the result of the reviewed chart. A possible reason for this is that the effect of social desirability bias is that nurses may over-report their usual behavior in the self-administered questionnaire. The study identified experience, good knowledge, positive attitudes, and training on pain assessment as significant factors positively influencing nurses’ pain assessment practices.
This study found that 63.5% of nurses demonstrated good pain assessment practices, which is a promising yet incomplete adherence to best practices in patient care. When compared to a similar study conducted in Wolaita Zone, Southern Ethiopia, the proportion of nurses with good pain assessment practices was 38.2%, significantly lower than the findings of the current study (Melile Mengesha et al., 2022). This suggests that pain assessment practices may vary across different regions, possibly due to differences in training, institutional support, or workload. Another study focusing on Comprehensive Specialized Hospitals in Ethiopia found that only a quarter of nurses had good pain management practices, indicating a broader challenge in ensuring effective pain assessment and management across healthcare settings (Fekede et al., 2023). Additionally, research on pain assessment in intensive care units highlighted that only 60% of nurses assessed pain in patients who could report it, and 50% did so for patients unable to communicate (Alnajar et al., 2021). These comparisons suggest that while Ethiopia has made progress in improving pain assessment among nurses, there is still a need for standardized training, institutional support, and policy interventions to ensure consistent and effective pain management practices nationwide.
According to this study, nurses with more than five years of work experience had significantly higher odds of demonstrating good pain assessment practice. This finding is in line with recent evidence and new trends in pain assessment practice (Gélinas, 2016). This may be because professional experience increases the likelihood that nurses working in elderly patient care units would conduct thorough and efficient pain assessments.
Good pain assessment practice was observed among nurses who possessed strong knowledge of pain assessment. This is supported by the study conducted in Ethiopia, Rwanda, and Saudi (AL-Sayaghi et al., 2022; Ayenew et al., 2021; Tuyishimire, 2017), which showed an association between knowledge and practice of the nursing staff regarding pain assessment. This may be since good knowledge improves the confidence and readiness of the nurses to do their routine activities and increases their ability to choose appropriate pain relief measures (Dagnew & Tewabe, 2021; Innab et al., 2022; Kibret et al., 2022; Wondimagegn et al., 2021). While theoretical knowledge of pain management is essential, it does not always translate into a positive attitude or improved practice. Previous research suggests that professionals may possess sufficient knowledge but still not properly practice pain management strategies (Ahmadi et al., 2023; Kahsay & Pitkäjärvi, 2019). This disconnect highlights the need to assess critically how knowledge influences practice and attitude.
This study’s findings showed that nurses with a favorable attitude towards pain assessment demonstrated good pain assessment practices. Previous studies support this (Bell & Duffy, 2009) which identified that the attitude of a caregiver is a significant barrier to effective pain assessment and has a statistically significant and positive relationship with the practice of nurses regarding pain assessment. This may be due to the reason that, as nurses have a favorable attitude, they will be motivated to provide care, to update themselves, and there will be a strong tendency to practice properly (Ahlstedt et al., 2020; Wang et al., 2024).
Nurses who received in-service training showed significantly better pain assessment practice. This was consistent with what has been found in other African countries (I. B. Kizza, 2012; Tuyishimire, 2017). However, having training on pain management was not associated with pain assessment practice, according to the study (Melile Mengesha et al., 2022). A similar conclusion was reached by previous studies, wherein a lack of training on pain management leads to poor pain assessment practice (Dutt, 2020; Onianwa et al., 2017), which found that caregiver training is a significant barrier to effective pain assessment and that it has a statistically significant positive relationship with nurses’ pain assessment practices. This may be due to the reason that, as nurses have training, they will be good at providing care, and there will be a big tendency to practice properly (Ahlstedt et al., 2020; Wang et al., 2024). Combining didactic sessions, practical demonstrations, and case discussions boosts knowledge, confidence, and routine use of standardized tools, so continuous professional development is essential to sustain improvements.
This study found that the majority of nurses reported the presence of standardized pain assessment tools (73.9%) and nearly all were aware of pain scales (97.7%), but less than half (43.1%) actually used these tools in practice. Structured assessments are hindered by heavy workloads, limited training, and weak organizational support, leaving nurses to rely mainly on judgment or patient self-report (Hamadeh et al., 2025; Olufunke, 2018; Rababa et al., 2021). Despite most nurses (86.5%) viewing pain tools as efficient, barriers such as poor bedside access, lack of chart integration, and limited supervisory support hinder their use. Improving practice requires workflow integration, leadership backing, and continuous training to ensure consistent application
Strengths and Limitations
On the strengths side, including self-reported data alongside patient chart reviews enhances the comprehensiveness of the findings. However, the cross-sectional design limits the ability to infer causality, and the exclusion of specialized units, coupled with the lack of direct observational data, restricts a full understanding of pain assessment practices. Additionally, this study may be subject to response bias, as some nurses might have provided socially desirable answers. Although anonymous data collection and confidentiality were ensured, the inherent limitations of self-reporting should be taken into account when interpreting the findings. These factors should be considered and highlight future research and methodological improvement.
Implications of the Study
This study underscores the need for hospitals to prioritize comprehensive in-service training programs that enhance nurses’ competencies and strengthen their approach to pain management through targeted behavioral training. Establish policies that mandate routine pain assessment and integrating monitoring systems will promote consistency and adherence to best practices. Additionally, leveraging technology such as digital pain scales and AI-driven tools can improve assessment accuracy, evaluation processes, and minimize subjectivity in clinical decision-making.
Conclusion
The study showed that while most nurses reported assessing pain, only two-thirds demonstrated adequate practice. Key factors significantly associated with better pain assessment practices included work experience exceeding five years, adequate knowledge of pain assessment, positive attitudes toward pain assessment, and receiving in-service training. These findings highlight the importance of enhancing healthcare workers’ knowledge, attitudes, and training programs to improve pain assessment practices. Addressing these factors through targeted educational interventions and regular training could lead to more consistent and effective pain management in clinical settings.
Supplemental Material
Supplemental material - Pain Assessment Practice and Associated Factors Among Nurses Working in Public Hospitals of West Hararge Zone, Eastern Ethiopia, 2023
Supplemental material for Pain Assessment Practice and Associated Factors Among Nurses Working in Public Hospitals of West Hararge Zone, Eastern Ethiopia, 2023 by Abdella Mohammed, Rudwan Yasin Abrahim, Kadir Abdu, Nesredin Ahmed, Daniel Alemu, Sisay Habte in Sage Open Nursing
Footnotes
Acknowledgments
We would like to acknowledge the data collectors, supervisors, study beneficiaries, health institution administrators, and data clerks
Ethical Considerations
This study was approved by the Institutional Health Research Ethics Review Committee (Approval no: IHRERC/116/2023). A letter of cooperation was written to each hospital to allow the execution of the research.
Consent to Participate
A written, signed informed consent was obtained from all study participants following adequate explanation on the study’s purpose, risk and benefits. The respondents were assured that the information obtained from them would be kept confidential.
Authors’ Contributions
AM, RY, NA, KA, DA, and SH conceived the review, all authors participated in the literature research and data analysis. All Authors participated in drafting, critically revising, and approving the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data used for the current study will be available upon submitting a reasonable request from either the corresponding author or the principal investigator.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.