
Abstract
Background
Mindfulness-based cognitive therapy (MBCT), which integrates cognitive therapy principles with mindfulness practices, may address both psychological distress and quality of life (QoL) among women with cancer. However, its specific benefits in this population remain insufficiently synthesized.
Objective
To evaluate the short-term (post-intervention) and longer-term (≥3 months follow-up) effects of MBCT on quality of life and mental health outcomes in women with cancer.
Methods
A systematic search of PubMed, CINAHL, Web of Science, Scopus, and Cochrane CENTRAL was conducted from inception to March 2026. Eligible studies included adult women with cancer receiving MBCT and reporting quantitative outcomes on quality of life or mental health. Risk of bias was assessed using standard tools. Where appropriate, random-effects meta-analyses were performed.
Results
Thirteen studies (n = 766) were included, of which nine contributed to meta-analysis. Participants had a mean age of 49.46 years, with breast cancer being the most common diagnosis (n = 10 studies). MBCT demonstrated improvements in QoL and selected mental health outcomes at both post-intervention and follow-up (all p < 0.05). Improvements were most consistent for fatigue, fear of cancer recurrence, and mindfulness. However, the certainty of evidence ranged from low to very low, primarily due to small sample sizes, heterogeneity, and risk of bias.
Conclusions
MBCT shows preliminary promise in improving QoL and psychological outcomes among women with cancer and may be feasibly integrated into survivorship care. However, findings should be interpreted with substantial caution given the limited certainty of evidence. Larger, methodologically rigorous trials are needed to confirm these exploratory effects.
Keywords
Introduction
Beyond physical burden, cancer is frequently accompanied by substantial psychological distress and deterioration in quality of life (QoL) (Niedzwiedz et al., 2019; Wu et al., 2024). These psychological sequelae negatively influence social functioning, treatment adherence, recovery, and long-term survivorship outcomes (Nguyen, Giap, et al., 2024). Given the central role of mental health in cancer survivorship, effective psychosocial interventions remain a clinical and research priority (Niedzwiedz et al., 2019).
Mindfulness-based cognitive therapy (MBCT) is a structured, manualized intervention that integrates mindfulness practices with cognitive-behavioral techniques to promote nonjudgmental awareness of thoughts and emotions and to reduce maladaptive cognitive patterns, particularly through decentering, reduced rumination, and more adaptive appraisal (Chang et al., 2023; Gkintoni et al., 2025; Schanche et al., 2020; Segal et al., 2012; Sipe & Eisendrath, 2012). In oncology, this therapeutic profile may be relevant because fear of recurrence, persistent worry, depressive symptoms, and fatigue often co-occur and may persist beyond active treatment (R et al., 2024). Emerging evidence suggests that MBCT may improve mindfulness, emotional regulation, fatigue, and psychological resilience among individuals with cancer (Abedini et al., 2021; Xiang et al., 2025; Zhu et al., 2023).
Although existing literature supports mindfulness-based interventions (MBIs) in oncology, these interventions are often synthesized as a broad category, making it difficult to determine whether outcomes attributed to mindfulness are also observed specifically in MBCT. Prior meta-analyses combining multiple MBIs obscure MBCT’s distinct effects (Galante et al., 2013; Kairen McCloy et al., 2022; Lin et al., 2022; Nissen et al., 2020). Even reviews focused on MBCT have frequently included male participants or restricted analyses to immediate post-intervention outcomes, reducing gender-specific relevance and limiting understanding of longer-term effects (Chang et al., 2023).
Women with cancer are disproportionately affected, experiencing higher rates of anxiety, depression, fear of recurrence, post-traumatic stress, and body image disturbances compared with men (Fan et al., 2023; Getie et al., 2025; Lebel et al., 2014;Nguyen et al., 2024). Current oncology guidance also supports mindfulness-based interventions as part of supportive care for anxiety, depression, and fatigue in adults with cancer, making it important to clarify how far the evidence specifically supports MBCT in women with cancer rather than mindfulness-based interventions in aggregation (Carlson et al., 2023; Chang et al., 2023; Peuckmann et al., 2007). Furthermore, evidence regarding QoL outcomes remains inconsistent, and follow-up beyond three months is rarely synthesized (Chang et al., 2023; K. McCloy et al., 2022; Nissen et al., 2020).
This systematic review and meta-analysis; therefore, specifically examined MBCT’s short- and long-term effects on QoL and mental health in women with cancer, addressing gaps in previous literature and clarifying its therapeutic potential in cancer survivorship. The review addressed the question: In women with cancer, how do mindfulness-based cognitive therapy (MBCT), compared to standard care or other psychological interventions, affect their quality of life and mental health outcomes?
Methods
This systematic review and meta-analysis was reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines (Page et al., 2021). This review protocol was registered in PROSPERO (2025 CRD420250634441). Available from https://www.crd.york.ac.uk/PROSPERO/view/CRD420250634441).
Database and Search Strategy
A comprehensive search was conducted in Pubmed, CINAHL, Web of Science, Scopus, and the Cochrane CENTRAL, using MeSH terms and keywords for “women,” “cancer,” “mindfulness-based cognitive therapy,” “quality of life,” and “mental health” (Supplemental Table S0). The searching was implemented without language and time restrictions from the inception date of each database to March, 2026. Reference lists of included studies were also screened manually. Six authors independently screened all identified titles and abstracts, resolving discrepancies through discussion with two senior authors.
Eligibility Criteria
The eligibility criteria were defined using the PICOS framework. (i) Population: Adult women (≥18 years) with any cancer type, stage, or treatment phase (undergoing or completed adjuvant treatment) (ii) Intervention: Mindfulness-based cognitive therapy (MBCT) delivered face-to-face, online, or in hybrid format, either as a standalone intervention or combined with other components (iii) Comparator: Usual care, wait-list, supportive counseling, no intervention, or other non-MBCT comparison conditions. (iv) Outcomes: Quality of life and mental health outcomes measured using validated instruments, including anxiety, depression, fatigue, rumination, fear of cancer recurrence, and mindfulness. (v) Study design: Randomized controlled trials, quasi-experimental studies, and single-arm intervention studies.
Exclusion criteria includes: (i) Studies that did not explicitly describe the intervention as MBCT or did not allow identification of an MBCT-specific component; (ii) studies including mixed populations (combining men and women or patients and caregivers without separate data for women with cancer); (iii) non-empirical studies (reviews, case reports, letters, commentaries, and conference abstracts); and (iv) does not report QoL or mental health outcomes using validated instruments.
Data Extraction
Extracted data included study characteristics (author, year, design, country, sample size, mean age, cancer type and stage, treatment history) and intervention details (type of intervention, delivery mode, duration, therapist involvement, control condition, and measurement tools). Primary outcomes included QoL and mental health (anxiety, depression, fatigue, and rumination). Secondary outcomes included mindfulness and fear of cancer recurrence, with mindfulness conceptualized as a process-related outcome reflecting a proposed mechanism of action of MBCT rather than a direct clinical endpoint. Six authors independently extracted data using a standardized data extraction checklist, verified by two senior reviewers.
Risk of Bias Assessment
Two reviewers independently assessed quality using RoB 2 for RCTs and ROBINS-I for nonrandomized studies (Jüni et al., 2016; Sterne et al., 2019). For RCTs, bias from randomization, deviations, missing data, measurement, and reporting was evaluated. For non-RCTs, bias from confounding, classification, selection, deviations, missing data, outcome measurement, and selective reporting was assessed.
Disagreements were resolved through discussion or consultation with a third reviewer.
Certainty of Evidence
The GRADE approach was used to evaluate overall certainty.
Data Synthesis and Analysis
A narrative synthesis summarized study characteristics. Meta-analysis was performed using Comprehensive Meta-Analysis v2.0 (Biostat, NJ, USA). Hedges’ g and 95% confidence intervals (CI) were calculated using a random-effects model; 0.2, 0.5, and 0.8 represented small, medium, and large effects (Goulet-Pelletier & Cousineau, 2018). Outcomes were analyzed for short-term (post-intervention) and long-term (≥3 months) effects. Heterogeneity was tested using Cochran Q and I2, interpreted as low (25%), moderate (50%), or high (75%) (Higgins et al., 2002). Pooled effects were reported only when ≥2 studies provided comparable data.
Given the limited number of studies per outcome and substantial clinical and methodological heterogeneity across interventions, populations, and outcome measures, subgroup analyses and meta-regressions were not conducted. Performing such analyses under these conditions would risk spurious findings and overinterpretation. Instead, a random-effects model was applied, and pooled estimates with high or extreme heterogeneity were interpreted cautiously as exploratory summaries rather than confirmatory effect estimates. Potential sources of inconsistency, including variation in cancer type and stage, intervention format and duration, comparator condition, and outcome measurement, were examined narratively. Certainty of evidence was therefore integrated into interpretation using the GRADE framework.
Results
Given the substantial variation in internal validity across study designs, evidence from randomized controlled trials (RCTs) was prioritized for meta-analytic pooling and causal inference. Findings from quasi-experimental and single-arm studies were synthesized narratively and interpreted as supportive or exploratory evidence only, without implying causal effects.
Search Summary
A total of 6680 studies were identified; after removing duplicates and screening of titles and abstracts, 13 papers met inclusion criteria and 9 studies were included in the meta-analysis (Figure 1). PRISMA 2020 flow diagram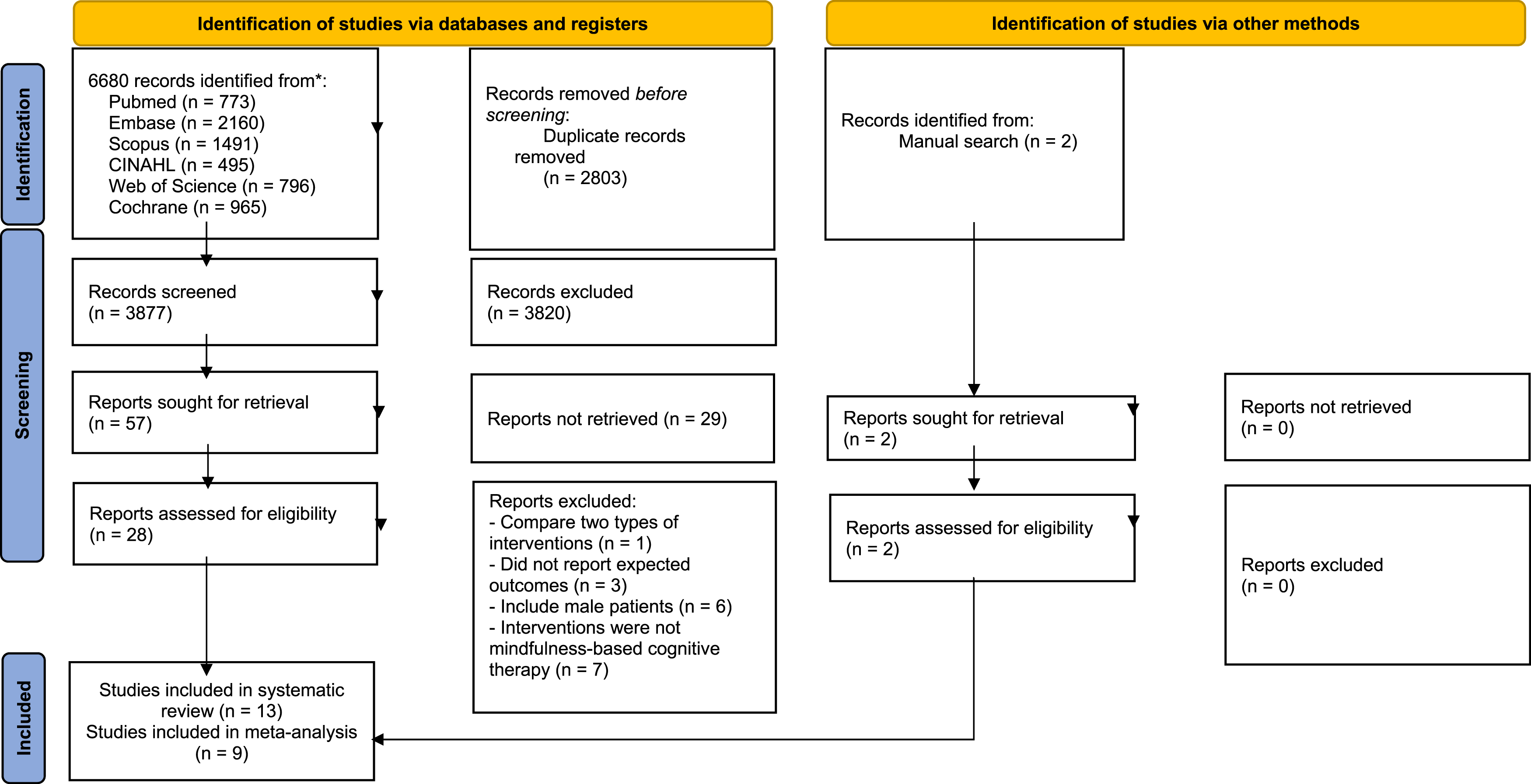
Participant Characteristics
Thirteen studies (N = 766) were included. Five of the thirteen included studies employed randomized controlled trial designs (n = 5) (Chu et al., 2020; Johannsen et al., 2016; Melis et al., 2023; Park et al., 2020; Shao et al., 2021), followed by quasi-experimental (n = 4) (Jodaki et al., 2022; Melati et al., 2024; Olyaie et al., 2016; Vaziri et al., 2017) and single-arm (n = 4) (Bober et al., 2020; Cohen et al., 2022; Park et al., 2018; Stafford et al., 2013). Mean participant age was 49.46 years. Breast cancer was predominant (n = 10) (Bober et al., 2020; Chu et al., 2020; Johannsen et al., 2016; Melati et al., 2024; Melis et al., 2023; Park et al., 2018; Shao et al., 2021; Olyaie et al., 2016; Vaziri et al., 2017), with others including ovarian (n = 1) (Cohen et al., 2022), cervical (n = 1) (Jodaki et al., 2022), and mixed gynecologic (n = 1) (Stafford et al., 2013). Cancer stage ranged from 0 – IV, though reporting was inconsistent. Time since completion of cancer treatment varied substantially across studies (approximately 11 – 42 months), and several studies did not report this variable, limiting subgroup or moderator analyses Most participants had received chemotherapy (Bober et al., 2020; Johannsen et al., 2016; Melati et al., 2024; Park et al., 2018, 2020; Shao et al., 2021; Stafford et al., 2013), radiotherapy (Johannsen et al., 2016; Melati et al., 2024; Park et al., 2018, 2020; Shao et al., 2021; Stafford et al., 2013; Vaziri et al., 2017), and/or surgery (Bober et al., 2020; Chu et al., 2020; Johannsen et al., 2016; Park et al., 2020; Shao et al., 2021; Olyaie et al., 2016).
Intervention Characteristics
Demographic Characteristics of Included Papers (n=13)

Abbreviations: IG, intervention group; CG, control group; N/I, no information.
†Overall mean age was calculated manually by weighting intervention and control group means by sample size. Standard deviations could not be reliably derived, as most primary studies reported age separately by group and did not provide pooled variance estimates.
Risk of Bias
For RCTs, supplemental Figure S1 provides a summary of the risk of bias assessments conducted across the included 5 studies. Overall, the two studies by Chu et al. (Chu et al., 2020) and Park et al. (Park et al., 2020) demonstrated high risk of bias across multiple domains, whereas those by Shao et al. (Shao et al., 2021), Melis et al. (Melis et al., 2023), and Johannsen et al. (Johannsen et al., 2016) exhibited a lower risk.
For Non-RCTs, all eight were rated “critical” overall, primarily due to confounding and subjective outcome measures, though participant selection and intervention classification were generally sound (Supplemental Figure S2).
Primary Outcomes
Quality of Life
In the post-intervention, the quality-of-life outcome was reported in eight studies (Chu et al., 2020; Jodaki et al., 2022; Johannsen et al., 2016; Melati et al., 2024; Park et al., 2018, 2020; Olyaie et al., 2016; Stafford et al., 2013). In Figure 2, the pooled results from six RCTs and quasi-experimental studies reported a statistically significant impact of MBCT intervention on the overall quality of life in women with cancer, with the overall pooled Hedges’ g value of 1.23 (95% CI 0.48-1.98, p = 0.001), indicating a large effect. The studies reported high heterogeneity (I2 = 92.36%, p < 0.001). Additionally, findings from single-arm studies further support the significant positive impact of MBCT on quality of life. Stafford et al. (Stafford et al., 2013) measured quality of life using the Functional Assessment of Cancer Therapy-General and reported a statistically significant improvement (p = 0.001). Similarly, Park et al. (Park et al., 2018) assessed quality of life using the Functional Assessment of Cancer Therapy-Breast Cancer (FACT-B), demonstrating a moderate effect size (d = 0.72, p < 0.01). The certainty of the evidence regarding the short-term effects of MBCT on quality of life was rated as very low (Supplemental Table S3), which is one of the important outcomes for women with cancer. This assessment was downgraded due to concerns related to substantial risk of bias, potential publication bias, and inconsistency across studies. The effects of mindfulness-based cognitive therapy at the post-intervention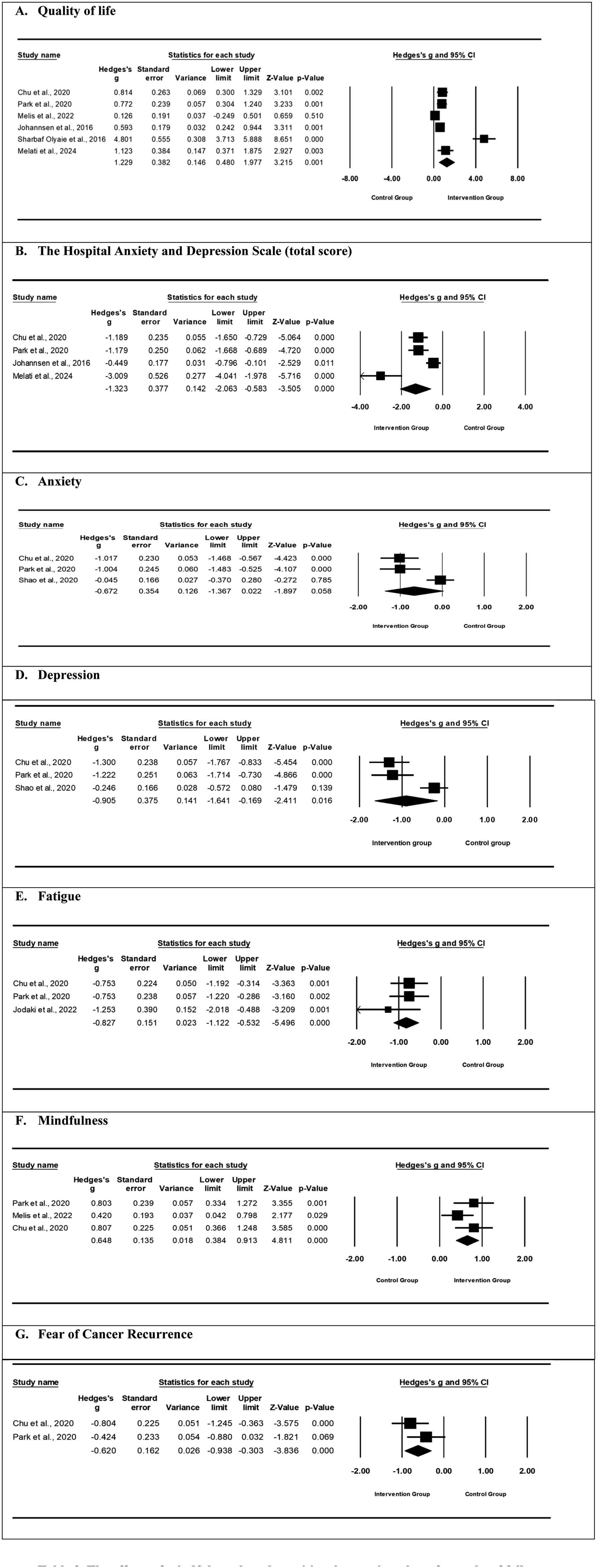
After at least three months of follow-up, six studies showed the effect of MBCT intervention on quality of life (Chu et al., 2020; Johannsen et al., 2016; Melis et al., 2023; Park et al., 2018, 2020; Stafford et al., 2013). The pooled findings from four studies revealed that MBCT still maintained a significant impact on quality of life with a Hedges’ g value of 0.51 (95% CI 0.20-0.82, p = 0.001, Figure 3). No significant heterogeneity was reported (I2 = 57.98%, p = 0.07). A single-arm study also supported these findings, substantially improving QoL, a positive correlation between pre- and 3 months post-intervention, measured by FACT-G with r = 0.45, p < 0.001 (Stafford et al., 2013). Similarly, Park et al. (Park et al., 2018) also reported improvement in QoL (measured by FACT-B, d = 0.86, r = 0.395, p < 0.01). The certainty of the evidence concerning the long-term effects of MBCT on quality of life was assessed as low (Supplemental Table S3), primarily due to risk of bias and inconsistency. The effects of mindfulness-based cognitive therapy in at least 3 months of follow-up
Mental Health (Anxiety and Depression)
At Post-intervention
In the post-intervention analysis, based on the Hospital Anxiety and Depression Scale (total score) reported in 6 studies (Chu et al., 2020; Johannsen et al., 2016; Melati et al., 2024; Park et al., 2018, 2020; Shao et al., 2021), Figure 2 yielded a large effect of MBCT with a Hedges’ g of -1.32 (95% CI: -2.06 to -0.58, p < 0.001). The studies reported high heterogeneity (I2 = 88.08%, p < 0.001). Furthermore, findings from single-arm studies also indicate significant improvements in psychological distress following MBCT interventions. Park et al. (Park et al., 2018) reported a substantial reduction in distress, as measured by the HADS, with effect sizes of 0.74 and 0.71 (p < 0.05). The overall certainty of the evidence for the short-term impact of MBCT on mental health, evaluated using HADS scores, was deemed very low (Supplemental Table S3). This rating was due to serious limitations identified across all GRADE assessment domains.
Regarding the anxiety outcome, which was reported in three studies (Chu et al., 2020; Park et al., 2020; Shao et al., 2021), the findings did not reveal a significant effect of MBCT on anxiety, with Hedges’ g of -0.67 (95% CI: -1.37 to 0.02, p = 0.01) in the post-intervention period (Figure 2). Additionally, single-arm studies further supported these findings, giving significant improvements in anxiety outcomes post-MBCT intervention. Park et al. (Park et al., 2018) reported reductions in anxiety (measured by HADS-Anxiety) with effect sizes of 0.88 immediately post-treatment. Similarly, Cohen et al. (Cohen et al., 2022) observed a consistent decrease in anxiety levels, with HADS scores improving from baseline (M = 8.72, SD = 3.99) to 8 weeks (M = 6.89, SD = 2.98). Bober et al. (Bober et al., 2020) also reported the significant improvement of anxiety from baseline and post-intervention among young breast cancer survivors (Cohen’s d = 0.98, p < 0.001). The certainty of evidence regarding the immediate effects of MBCT on anxiety symptoms was rated as very low (Supplemental Table S3). This judgment reflected downgrading due to notable concerns about risk of bias, imprecision, and inconsistency among included studies.
In terms of depression outcomes, the meta-analysis of three RCTs (Chu et al., 2020; Park et al., 2020; Shao et al., 2021) revealed a large and statistically significant effect favoring MBIs, with a Hedges’ g of -0.91 (95% CI: -1.64 to -0.17, p = 0.02, Figure 2), suggesting a reduction in depressive symptoms following intervention. However, single-armed studies show a different picture. Cohen et al. (Cohen et al., 2022) did not observe a significant change in depression levels post-intervention, with HADS-Depression scores averaging 3.10 (SD = 1.79), p = 0.13 after 8 weeks. Similarly, Park et al. (Park et al., 2018) reported a moderate, though only marginally significant, improvement (HADS-Depression: d = 0.53, p = 0.054). Bober et al. (Bober et al., 2020) also noted a slight decrease in symptoms based on the BSI-18, from baseline (M = 50.37, SD = 8.28) to post-treatment (M = 47.32, SD = 6.91), though this change did not reach statistical significance (p = 0.07). From a quasi-experimental design, Vaziri et al. (Vaziri et al., 2017) also reported a non-significant effect of intervention at either post-intervention (p = 0.49) or follow-up (p = 0.24). The certainty of evidence regarding the short-term effects of MBCT on depressive symptoms was assessed as very low (Supplemental Table S3) due to concerns about risk of bias, inconsistency, and imprecision across studies.
At ≥ 3 Month Follow-Up
The impact of the MBCT intervention on anxiety and depression in at least 3 months of follow-up were presented in Figure 3. The findings from three RCTs (Chu et al., 2020; Johannsen et al., 2016; Park et al., 2020) demonstrated a significant reduction in combined anxiety and depression scores, as measured by the Hospital Anxiety and Depression Scale (total score). The pooled effect size was -0.81 (95% CI: -1.18 to -0.45, p < 0.001), indicating a significant reduction in anxiety and depression. Heterogeneity was moderate (I2 = 54.30%, p = 0.11). The certainty of evidence for the long-term effects of MBCT on mental health, as assessed by HADS scores, was very low due to risk of bias, inconsistency, and imprecision (Supplemental Table S3).
The pooled results from three RCTs (Chu et al., 2020; Park et al., 2020; Shao et al., 2021) demonstrated a significant reduction in anxiety among participants who received MBCT compared to the control groups. The overall Hedges’ g was -0.58 (95% CI: -1.089 to -0.070, p = 0.026), indicating a moderate effect. However, heterogeneity across studies was substantial (I 2 = 78.42%, p = 0.01). Meta-analytic estimates were derived exclusively from randomized controlled trials. Findings from quasi-experimental and single-arm studies are reported separately and narratively to provide contextual insight but should be interpreted with caution due to limited internal validity. In Park et al. (Park et al., 2018), participants reported significant improvements at three months (Cohen’s d = 1.06, p < 0.001). Cohen et al. (Cohen et al., 2022) reported sustained reductions from post-intervention (mean = 6.89, SD = 2.98) to six months of follow-up (mean = 7.06, SD = 3.87) with p < 0.01. The certainty of evidence for the long-term effects of MBCT on anxiety was rated low, primarily due to risk of bias and imprecision (Supplemental Table S3).
Our meta-analysis of three RCTs (Chu et al., 2020; Park et al., 2020; Shao et al., 2021) demonstrated a statistically significant benefit of MBCT on depressive symptoms, yielding a Hedges’ g of -0.74 (95% CI: -1.35 to -0.14, p = 0.02). Despite the overall effect, heterogeneity among these studies was considerable (I 2 = 84.28%, p = 0.002). Findings from single-arm studies reported inconsistent impact of MBCT on depressive symptoms. Cohen et al. (Cohen et al., 2022) observed non-significant change in depression scores between post-intervention (mean = 3.10, SD = 1.79) and six months later (mean = 2.73, SD = 1.88) with p = 0.13. In Park et al. (Park et al., 2018), a trend toward improvement in depression was reported at three months (Cohen’s d = 1.28, p < 0.001). The certainty of evidence for the long-term effects of MBCT on depression was judged very low, reflecting serious concerns about risk of bias, inconsistency, and imprecision (Supplemental Table S3).
Fatigue
At post-intervention, our meta-analysis of three RCTs (Chu et al., 2020; Jodaki et al., 2022; Park et al., 2020) assessed the effectiveness of MBCT on fatigue symptoms. The pooled effect size was statistically significant, with a Hedges’ g of -0.83 (95% CI: -1.12 to -0.53, p < 0.001, Figure 2). Notably, no heterogeneity was observed across the included studies (I 2 = 0.00%, p = 0.49). The overall certainty of the evidence on the short-term effects of MBCT in alleviating fatigue was considered low, owing to substantial concerns about risk of bias and publication bias (Supplemental Table S3).
At least 3 months of follow-up, our meta-analysis of the same three RCTs (Chu et al., 2020; Jodaki et al., 2022; Park et al., 2020) reported a reduction in fatigue. The pooled effect size was Hedges’s g = -0.62 (95% CI: -0.91 to -0.33, p < 0.001, Figure 3). Heterogeneity was very low (I 2 = 0.00%, p = 0.925). The certainty of the evidence for the long-term effects of MBCT on fatigue was assessed as moderate, primarily due to concerns regarding risk of bias (Supplemental Table S3).
Rumination
Cohen et al. (Cohen et al., 2022) reported a decrease in rumination scores from 9.37 ± 2.56 at baseline to 8.11 ± 1.45 post-intervention. Jodaki et al. (Jodaki et al., 2022) observed a notable reduction in the intervention group, with mean scores dropping from 52.4 (SD = 7.45) to 37.4 (SD = 7.76), while the control group remained relatively stable. Vaziri et al. (35) also found a reduction in rumination scores in the intervention group, from 15 (SD = 3.16) to 14.62 (SD = 4.83).
Secondary Outcomes
Mindfulness
In the post-intervention, our meta-analysis of three studies (Chu et al., 2020; Melis et al., 2023; Park et al., 2020) revealed a medium statistically significant effect of MBCT on mindfulness. The pooled Hedges’ g was 0.65 (95% CI: 0.38–0.91, p < 0.001, Figure 2). Heterogeneity was low (I2 = 13.49%, p = 0.32). The results suggested numerical reductions in anxiety and depressive symptoms following MBCT; however, these changes were not consistently statistically significant, and findings should be interpreted cautiously, particularly as several results were derived from non-randomized or single-arm studies. Stafford et al. (Stafford et al., 2013) demonstrated a significant improvement in mindfulness (r = 0.60, p < 0.001) as measured by the Freiburg Mindfulness Inventory. Similarly, Cohen et al. (Cohen et al., 2022) reported a strong correlation (r = 0.6) using the same instrument. Park et al. (Park et al., 2018), using the Five Facet Mindfulness Questionnaire, observed significant improvements in mindfulness scores (r = 0.43, p < 0.01), with a post-intervention mean of 125.6 (SD = 23.7). The certainty of the evidence for the short-term effects of MBCT on mindfulness was rated moderate, with downgrading due to concerns about risk of bias (Supplemental Table S3).
In at least 3 months of follow-up, the pooled results indicated a significant effect of MBCT on mindfulness, with a Hedges value of 0.81 (95% CI, 0.30 to 1.33, p = 0.002, Figure 3). The studies were highly heterogeneous (I2 = 76.16%, p = 0.02). Further supporting these results, findings from single-arm studies also indicate significant improvements in mindfulness following MBCT interventions. Park et al. (Park et al., 2018) reported significant improvements in mindfulness, as measured by the FFMQ, with an effect size of 1.73 and p < 0.01. Similarly, Cohen et al. (Cohen et al., 2022) reported improvements in mindfulness at the 6-month follow-up (M = 41, SD = 6.21) compared to baseline (M = 34.37, SD = 7.56). Additionally, Stafford et al. (Stafford et al., 2013) assessed mindfulness using FMI, with a moderate effect size (d = 0.363, p < 0.001). The certainty of the evidence for the long-term impact of MBCT on mindfulness was assessed as low due to limitations related to risk of bias and inconsistency (Supplemental Table S3).
Fear of Cancer Recurrence
In the post-intervention period, Figure 2 revealed that our meta-analysis of FCR outcomes from two studies (Chu et al., 2020; Park et al., 2020), demonstrated a moderate reduction in FCR following MBCT. The pooled Hedges’ g was -0.62 (95% CI: -0.94 to -0.30, p < 0.001, Figure 2), indicating a statistically significant improvement. The heterogeneity was low (I2 = 27.54%, p = 0.240). Additionally, Cohen et al. (Cohen et al., 2022) reported a significant reduction in FCR at 8 weeks, with the FCR inventory mean score decreasing from 71.03 (SD = 31.01) at baseline to 63.00 (SD = 27.90) post-intervention (r = 0.21). The certainty of the evidence on the short-term impact of MBCT on fear of cancer recurrence was rated as low, reflecting limitations arising from notable risk of bias and imprecision (Supplemental Table S3).
In at least 3 months of follow-up, the pooled results indicated a significant effect of MBCT on the FCR, with a Hedges value of -0.68 (95% CI, -0.99 to -0.36, p < 0.001) indicating a medium effect (Figure 3). No significant heterogeneity was observed (I2 = 0.0%, p = 0.577). Additionally, in a single-arm study, the effect in a study by Cohen et al. (Cohen et al., 2022) was not maintained at the 6-month follow-up (M = 63.65, SD = 30.08). The certainty of the evidence on the long-term effects of MBCT on fear of cancer recurrence was judged as low, reflecting limitations arising from notable risk of bias and imprecision (Supplemental Table S3).
Discussion
This systematic review and meta-analysis suggests potential benefits of MBCT in improving quality of life (QoL), depression, fatigue, mindfulness, and fear of recurrence among women with cancer, with some evidence of effects potentially sustained up to three months. However, anxiety was non-significant post-intervention but became significant at three-month follow-up, suggesting a delayed effect.
Effects on Primary Outcomes
Quality of Life
QoL was a primary outcome of interest in this review, given that cancer and its treatments often profoundly affect patients’ physical, emotional, and social well-being (Niedzwiedz et al., 2019). This meta-analysis represents the first review to independently evaluate the specific effects of MBCT on QoL among women with cancer, thereby addressing a gap in the existing literature where MBCT has often been examined alongside other types of mindfulness, resulting in unclear evidence regarding its distinct effectiveness. Our analysis yielded statistically significant pooled effects suggesting possible improvement in overall QoL scores for women with cancer, both immediately after the intervention and at the three-month follow-up. Similar to a cost-utility study, which found a medium improvement in utility-based QoL using Euro Qol-5D-3L utility scores and quality-adjusted life years when comparing MBCT to usual care (Compen et al., 2020), it’s possible that in more distressed populations, MBCT yields an appreciable lift in QoL that could be considered clinically significant (for instance, moving a patient from a state of serious impairment to moderate impairment). Although the direction of effect was generally favorable, the magnitude varied markedly across studies, and the considerable heterogeneity of the pooled outcome suggests that the magnitude of MBCT’s effect may depend on specific contextual factors, such as cancer type and stage, or differences in the delivery format of the MBCT program. These differences suggest the need for additional studies to identify which subgroups of cancer patients are most responsive to MBCT. For instance, meta-analysis synthesized evidence from 18 RCTs and reported a significant effect of MBSR/MBCT interventions on QoL, with the most pronounced improvements observed in patients with early-stage cancer (Lin et al., 2022).
Depression, Anxiety, Rumination, and Fatigue
For mental health outcomes, the pattern of findings is compatible with positive effects of MBCT. Our findings align with prior meta-analyses that have highlighted the efficacy of MBCT in alleviating symptoms of depression and anxiety when compared to control groups (Nissen et al., 2020; Seshadri et al., 2021). Gowin et al. (2025) discuss MBCT as part of integrative therapies for cancer patients, emphasizing its role in reducing anxiety, depression, and fatigue (Gowin et al., 2025). However, the observed effect sizes in our analysis were in the low-to-moderate range, which raises the question of clinical significance. Previous meta-analyses in breast cancer have likewise found statistically significant yet modest improvements, noting that these averages often fall below thresholds for minimally important clinical differences (Haller et al., 2017; Pe et al., 2018). Notably, for anxiety, the immediate post-intervention effects in our analysis were non-significant; however, significant improvements emerged at follow-up. Possible reasons for this could be the gradual nature of skill acquisition and behavioral adaptations facilitated by mindfulness practices, as follow-up periods provide sufficient time for these mechanisms to unfold and demonstrate their efficacy fully. Additionally, anxiety may be part of a symptom cluster, where various interrelated symptoms interact in complex ways (Nguyen & Nguyen, 2022). These interactions might not immediately manifest as significant changes following an intervention but could become apparent over time. The sustained nature of mindfulness practices allows for deeper engagement with the interconnected symptoms, facilitating gradual improvements. As these symptoms work together within the cluster (Nguyen & Nguyen, 2022), they may require a longer period to show collective and substantial changes, which explains the significant reduction in anxiety observed at follow-up. This suggests that MBCT’s benefits for anxiety develop gradually as participants continue to practice mindfulness skills in their daily lives. Nevertheless, even modest changes in emotional well-being and coping abilities can meaningfully enhance patients’ survivorship experiences (Lim et al., 2022; Salsman et al., 2023). Additionally, the findings from our systematic analysis on fatigue reduction indicate that MBCT helps patients manage cancer-related exhaustion, possibly by promoting energy conservation, reducing stress, and improving sleep. Given the strong association between psychological distress and fatigue (Ekels et al., 2025), MBCT may support emotional regulation among female cancer survivors, a population at heightened risk for anxiety, depression, and fear of recurrence, and may be feasibly integrated into nursing-led survivorship and psychosocial care programs (Zhang et al., 2022). MBCT was also found to reduce rumination, a maladaptive cognitive process closely linked to anxiety and depression in women with cancer. By encouraging participants to observe their thoughts nonjudgmentally and disengage from automatic negative thinking, MBCT interrupts the ruminative cycle that often exacerbates emotional distress. These findings align with MBCT’s cognitive framework (Lubbers et al., 2022), which targets thought patterns more explicitly than other mindfulness-based interventions. However, limited studies assessed rumination as a primary outcome, warranting further research to explore its mediating role in psychological recovery (Öcalan & Üzar‐Özçetin, 2021).
Effects on Secondary Outcomes
Mindfulness facilitates the development of a compassionate perspective and enhances self-awareness regarding one’s cognitive and emotional states (Khoury et al., 2025; Miller & Verhaeghen, 2022). For individuals with cancer, it may offer a profound insight into the meaning and purpose of life (Khoury et al., 2025; Park et al., 2020). Our review revealed that MBCT significantly enhanced mindfulness skills, reinforcing the intervention’s effectiveness in cultivating self-awareness and present-moment focus (Luberto et al., 2019). Previous research involving patients diagnosed with cancer has similarly demonstrated that MBCT interventions significantly enhance mindfulness, with particular benefits for individuals with high levels of rumination (Frostadottir & Dorjee, 2019). Increased mindfulness is associated with better emotional regulation, reduced psychological distress, and improved coping mechanisms, making it a critical mediator of MBCT’s benefits. Additionally, MBCT significantly reduced FCR, a prevalent source of anxiety among survivors. Cincidda et al. (Cincidda et al., 2022) conducted a review of remote psychological interventions for FCR and found that MBCT was one of the most effective methods. By promoting acceptance of uncertainty and reducing cognitive avoidance behaviors, MBCT provided patients with a structured way to manage FCR, allowing them to engage more fully in their daily lives (Moghadam et al., 2023).
Strengths and Limitations
In addition to assessing the immediate effects of MBCT, our study also examines its long-term outcomes, addressing a critical gap in existing literature. The findings suggest that MBCT not only improves quality of life and mindfulness but also could reduce symptoms of depression, fatigue, and FCR in the long-term. These results underscore the sustained psychological benefits of MBCT, highlighting its potential as an effective intervention for enhancing the mental well-being of cancer patients.
However, some limitations in this study should be noted. The review included both RCTs, quasi-experimental, and single-arm studies in meta-analysis. While RCTs are considered the gold standard for evaluating intervention effectiveness due to their ability to minimize bias through randomization and allocation concealment, quasi-experimental and single-arm studies often lack methodological design, and non-randomized studies were frequently at risk of bias therefore cannot support strong causal inference. As a result, the pooled estimates may be affected by selection bias and confounding, potentially reducing the accuracy and reliability of the overall findings. Additionally, several included studies exhibited a high risk of bias and a certainty of evidence ranging from low to moderate, which may have compromised the robustness of the findings. Several outcomes demonstrated substantial heterogeneity, with I2 values exceeding 90% in some analyses. This heterogeneity likely reflects meaningful clinical and methodological diversity rather than statistical noise, including variation in cancer type and stage, baseline psychological distress, MBCT delivery format (face-to-face vs. online), intervention duration, comparator conditions, and outcome measurement instruments. Importantly, high heterogeneity is common in psychosocial intervention meta-analyses and does not invalidate pooled estimates when random-effects models are used; however, it necessitates cautious interpretation focused on directionality rather than magnitude of effects.
Implications for Practice
Standardizing MBCT delivery and conducting high-quality RCTs with adequate power and long-term follow-up is essential to strengthen the evidence base and facilitate integration into psycho-oncology care pathways. Nurses can lead MBCT implementation by training in protocol delivery, embedding 8-week group sessions into survivorship clinics, and monitoring adherence through weekly check-ins to support emotional regulation and reduce fatigue in female cancer survivors. Depending on local service models, nurse-led or nurse-supported delivery formats may also improve accessibility and continuity of care. These findings further suggest a need for professional education in evidence-based psychosocial interventions, including mindfulness-informed approaches, so that nurses can competently support patients experiencing persistent distress during and after cancer treatment. Future trials should include subgroup analyses to explore moderators such as cancer type and stage, treatment phase, baseline psychological distress, and sociodemographic characteristics, which may influence intervention effectiveness. To improve methodological rigor, future meta-analyses should focus exclusively on RCTs, report adherence to intervention protocols, and include core outcome sets to enhance comparability across studies.
Conclusion
This systematic review and meta-analysis suggests that mindfulness-based cognitive therapy may offer potential benefits for quality of life and selected mental health outcomes among women with cancer. However, the certainty of the evidence was predominantly low to very low, reflecting substantial heterogeneity, methodological limitations, and risk of bias across included studies. While improvements in quality of life, fatigue, fear of cancer recurrence, and mindfulness were observed, these findings should be interpreted cautiously and primarily as indicative rather than definitive. The delayed effects observed for anxiety further suggest that benefits of MBCT may emerge over time as mindfulness skills consolidate. Overall, MBCT represents a promising psychosocial intervention within nursing-led cancer survivorship care, but well-designed, adequately powered randomized controlled trials with standardized outcomes and longer follow-up are required to establish the magnitude and durability of its effects.
Supplemental Material
Supplemental material - Effects of Mindfulness-Based Cognitive Therapy on Quality of Life and Mental Health Among Women With Cancer: Systematic Review and Meta-Analysis
Supplemental material for Effects of Mindfulness-Based Cognitive Therapy on Quality of Life and Mental Health Among Women With Cancer: Systematic Review and Meta-Analysis by Huyen Thi Hoa Nguyen, Hien Thi Bui, My Huyen Hac, Tran Ngoc Tran, Anh Chau Nguyen, Thanh Chau Nguyen, Quyen Thu Do, Quyen Ngoc Bao Nguyen, Anh Quynh Dang in Sage Open Nursing
Footnotes
Ethical Considerations
This systematic review and meta-analysis was conducted using previously published studies available in the public domain. No new data were collected from human participants or animals. Therefore, ethics approval and informed consent were not required.
Author Contributions
Funding
This research was supported by VinUniversity.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The raw data will be provided upon the appropriate request by the researcher. All data generated or analyzed during this study are included in this published article and its supplementary information files.
Registration
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.