
Abstract
Introduction
Verbal workplace violence (WPV) is the most frequent form of aggression experienced by nurses and represents a significant psychosocial risk for professional well-being and workforce sustainability. Although individual resources such as self-efficacy and coping strategies may influence nurses’ responses to verbal WPV, their role should be interpreted within the context of chronic occupational stress.
Objective
This study aimed to examine the prevalence and characteristics of verbal WPV among Italian nurses and to investigate its associations with burnout, psychological distress, perceived self-efficacy, and coping strategies, comparing nurses exposed and not exposed to verbal WPV.
Methods
A cross-sectional quantitative study was conducted using an online self-administered questionnaire. A convenience sample of 384 Italian nurses completed validated measures assessing exposure to verbal WPV, burnout (Oldenburg Burnout Inventory), psychological distress (GHQ-12), perceived self-efficacy at work, and coping strategies (Brief COPE). Descriptive analyses, group comparisons, correlation analyses, and multiple linear regression models were performed, stratified by exposure to verbal WPV.
Results
Overall, 34.4% of participants reported experiencing verbal WPV, most frequently in high-pressure clinical settings. Nurses exposed to verbal WPV reported lower levels of emotional exhaustion but slightly higher psychological distress compared with non-exposed nurses. They also reported higher perceived self-efficacy and greater use of problem-focused and cognitive coping strategies. Among exposed nurses, self-efficacy and coping strategies explained a substantial proportion of variance in exhaustion and disengagement, indicating complex and non-linear psychological adaptation processes. More linear occupational stress patterns emerged among non-exposed nurses.
Conclusion
Verbal WPV is a pervasive occupational hazard in nursing and is associated with differentiated psychological adaptation processes rather than uniformly protective or detrimental outcomes. These findings indicate that organisations cannot rely solely on individual interventions and must take responsibility for preventing violence.
Keywords
Introduction
Workplace violence (WPV) represents a persistent threat to nurses due to their frontline position, the nature of their work, and their close contact with patients and families in high-stress or emotionally charged situations (Pich et al., 2010). Among the forms of WPV, the verbal WPV, i.e. derogatory words, threats, accusatory or abusive language, is the most frequent in this working population (Einarsen et al., 2020; Matthiesen & Einarsen, 2010). Amongst the individual factors that may indicate greater exposure to the phenomenon, age and gender are indicated, with particular reference to the vulnerability of younger nurses. In addition, certain characteristics of nursing staff may contribute to violent episodes by patients or their families, for instance, poor communication, inadequate staffing levels (high patient-to-nurse ratios), or lack of competence in managing violent incidents. The consequences of verbal WPV include anger, irritability, fear, loss of self-confidence, humiliation, anxiety, depressive symptoms, post-traumatic stress disorder, and burnout (Rasouli et al., 2025), and have been shown to negatively affect work engagement and increase emotional exhaustion (Cao et al., 2023; Spector et al., 2014). However, these outcomes do not occur uniformly among exposed professionals.
Review of Literature
The literature indicates that individual responses to verbal WPV are influenced by various psychological resources (including perceived self-efficacy, coping strategies, and organisational support) which modulate the impact of the phenomenon on work-related well-being and the quality of care provided (Atiq et al., 2025). There may also be protective factors that mitigate the perception of the victimisation experience. In a study by Cavallari et al. (2025), it was found that self-efficacy is a central personal resource that helps individuals navigate workplace demands (Bandura, 1982). Within the framework of Social Cognitive Theory, self-efficacy is defined as the belief in one’s ability to exert control over actions and environmental challenges, shaping how people regulate their behaviour, cope with stressors, and respond to situational demands (Bandura, 2001; Wu et al., 2025). Higher self-efficacy has been associated with greater resilience, more adaptive coping, and lower burnout among healthcare professionals (Atiq et al., 2025; Cavallari et al., 2025; Marzocchi et al., 2024). Moreover, several qualitative and quantitative studies (Chapman et al., 2010; Itzhaki et al., 2015; Pien et al., 2025) indicate that nurses respond to WPV through cognitive adaptation processes, often relying on coping strategies to regulate stress (João & Portaleda, 2023; Taylor, 1983). However, evidence integrating psychological resources with adaptation processes under chronic verbal WPV remains limited (Zeng et al., 2025). Particularly in the Italian context, the underlying psychological dynamics have received little attention, as existing studies focus primarily on the prevalence of the phenomenon. This study seeks to address this gap by proposing an integrated perspective linking self-efficacy, coping, and burnout.
Current Study
In Italy, 461,313 nurses are registered in professional registers (data from the National Federation of Nursing Profession, June 2025). The National Federation of Nursing Professions reports that 40.2% of nurses experienced assaults in 2024, an increase from 32.3% in 2021–2022. A study by Cesare et al. (2025) found that, among 3,949 nurses surveyed, 20% reported experiencing one episode of violence in the past 12 months. Perceived self-efficacy at work is expected to be associated with dimensions of burnout, such that higher self-efficacy correlates with lower levels of emotional exhaustion and disengagement (Hypothesis 1). However, consistent with models of psychological adaptation to chronic stress, this relationship may be nonlinear among nurses exposed to verbal WPV. Nurses with higher perceived efficacy are expected to report greater use of cognitive regulation and adaptive coping strategies. However, in contexts of repeated exposure to verbal WPV, even traditionally adaptive strategies may involve greater emotional investment and psychological costs over time (Hypothesis 2). A third aspect concerns whether these associations differ between nurses exposed to verbal WPV and those who are not (Hypothesis 3). Among exposed nurses, burnout is expected to reflect more complex and differentiated coping processes, shaped by efforts to maintain professional functioning under persistent stress. In contrast, among unexposed nurses, the relationships between personal resources and burnout are expected to follow more linear and classical models of work-related stress. The three hypotheses were formulated based on a critical analysis of the existing literature and an integrated theoretical framework combining Social Cognitive Theory (Bandura, 2001), transactional models of occupational stress (Lazarus & Folkman, 1987), and theories of psychological adaptation to chronic violence (Chapman et al., 2010). They are working hypotheses intended to explore the complexity of adaptation processes in contexts of exposure to verbal violence.
Method
A cross-sectional quantitative observational study was conducted using a self-administered questionnaire. Data were collected with a questionnaire that included sociodemographic characteristics, assessment of episodes of verbal violence, coping strategies adopted, psychological distress, perceived self-efficacy at work, and burnout. The first part of the questionnaire outlined the purpose of the research, provided the declaration of informed consent, instructions for completion, a guarantee of anonymity, and the privacy policy. The second part collected sociodemographic data. All psychometric instruments included in the questionnaire are validated scales with established psychometric properties, as detailed in the respective subsections below. The complete questionnaire, including the full text of all items and response scales in the version administered to participants, is provided as Supplementary Material (see Supplementary File 1, 2). To analyse perceived victimisation in the workplace, the Violent Incident Form (VIF) was used. The VIF is a standardised documentation tool for recording and assessing episodes of violence. The instrument typically covers several domains, including classification of the violent act (e.g., physical aggression, verbal abuse, threats, or intimidation), situational and environmental circumstances, and descriptive information about the perpetrator and the consequences of the incident. In this study, only verbal violence (including verbal abuse, threats, and intimidation) was considered.
The questionnaire included the Oldenburg Burnout Inventory (OLBI; Demerouti & Bakker, 2008), used to assess burnout as a two-dimensional construct, consisting of Exhaustion (i.e., physical, cognitive, and emotional fatigue, reflecting chronic depletion of energy resources) and Disengagement from work (i.e., distancing from work, reduced identification, and diminished enthusiasm). It consists of 16 items, with 8 items each measuring Exhaustion and Disengagement. A distinctive feature of the OLBI is its systematic use of both positively and negatively worded items (for example: “I always find new and interesting aspects in my work”), intended to reduce response bias and acquiescence effects while capturing the full continuum of each dimension. Items are rated on a Likert-type scale ranging from 1 “strongly disagree” to 4 “strongly agree” (in this study, Cronbach’s alpha = .81). The General Health Questionnaire-12 items (GHQ-12, Goldberg, 1997) was used to assess current psychological distress. It evaluates respondents’ recent experiences of symptoms related to psychological functioning (for example: “Have you recently felt unhappy and depressed?'). In this study, the bimodal method (0-0-1-1) scoring was used. A score above 3/4 indicates psychological distress and suggests the need for further evaluation for potential mental disorders (Cronbach’s alpha = .80).
To assess victims’ self-efficacy regarding current and future work, the Perceived Self-Efficacy Scale at Work (Farnese et al., 2007) was used, consisting of ten items. The scale identifies two dimensions: Relational Willingness, which refers to the ability to manage relationships with colleagues and superiors, work with diverse teams, and handle conflicts; and Commitment, which concerns the perception of being able to achieve goals, meet deadlines, and face work difficulties. For example, the scale includes items such as “Thinking about a current job... you believe that you have the ability to collaborate with other colleagues” (possible answers ranging from 1–Not at all to 5–Completely) (Cronbach’s alpha = .96 and .97 respectively). To assess coping strategies, the Brief COPE (Carver, 1997; Italian version by; Conti, 1999), consisting of 28 items, was used (for example: “I have been expressing my negative feelings”; possible answers range from “1 = I have not been doing this at all” to “4 = I have been doing this a lot”). Each coping strategy (see Table 2) corresponds to a set of questions presented in random order; the strategy with the highest score (ranging from 2 to 8) is considered the most frequently used (Cronbach’s alpha = .92).
Procedure and Statistical Analysis
The questionnaire was distributed through professional groups on social media platforms dedicated to Italian nurses (e.g., Facebook groups for the profession, online professional forums) and by word of mouth among colleagues. The survey link was shared in multiple waves during the data collection period (June–July 2025), without the possibility of tracking the exact number of individuals initially reached, as the viral mode of dissemination did not allow systematic monitoring of access. No incomplete questionnaires were recorded or excluded from the analysis, as the LimeSurvey platform was configured to allow submission only of questionnaires completed in all mandatory sections. This setting prevented the collection of data on potential dropouts during completion, representing a limitation in assessing the actual response rate. Prior to completing the questionnaire, all participants provided written informed consent in digital form by actively ticking a mandatory checkbox confirming their agreement to participate. Only those who provided consent were able to proceed to the survey. The study was conducted in accordance with current regulations and adhered to the principles of the Declaration of Helsinki. In line with national and institutional guidelines, formal Ethics Committee approval was not deemed mandatory for this type of study. Specifically, according to Italian legislation and European directives, studies conducted on fully anonymised data that do not involve the collection of sensitive personal data, special categories of data, or data relating to vulnerable populations are exempt from mandatory ethical committee review. In the present study, no names, email addresses, telephone numbers, or any other directly or indirectly identifiable information were collected, and no cross-referencing of responses could allow individual identification. No incentives were offered for participation.
IBM SPSS Statistics version 29 was used to produce descriptive and inferential statistics. Descriptive measures (mean ± SD) were calculated for all test variables for the two groups of participants (victims and non-victims). χ2 tests, followed by effect size calculations (Phi and Cramer’s V) to estimate the practical significance of the differences, were used to assess differences in socio-demographic characteristics, burnout (Exhaustion and Disengagement), psychological distress, perceived self-efficacy, and coping strategies between victims and non-victims. As a post hoc test, standardised Pearson residuals (SPRs) were calculated for each cell to determine which cell differences contributed to the χ2 test results. SPRs with absolute values greater than 1.96 indicated that the number of cases in that cell was significantly larger or smaller than expected (in terms of over- or underrepresentation) if the null hypothesis were true, with a significance level of .05 (Agresti, 2013). T-tests were used to examine differences in mean scores between nurses who were exposed to verbal WPV and those who were not. Cohen’s d was used to calculate the effect size. Correlations were calculated to examine relationships between variables. Multiple linear regression analysis was performed: burnout scores (Exhaustion, Disengagement) were considered as dependent variables, while psychological distress, self-efficacy, and coping strategies were used as explanatory variables. Statistical significance was set at p < 0.05.
Participants
As stated above, there are 461,313 nurses registered in professional registers in Italy. The minimum sample size (n = 384) was calculated based on the known size of the Italian nursing population, assuming a conservative expected prevalence of 50%, a 95% confidence level, and a 5% margin of error, using standard sample size estimation formulas for prevalence studies. Eligible participants were nursing professionals currently in employment. Unemployed nurses and individuals who did not provide informed consent were excluded. A non-probability convenience sampling strategy was adopted. As recruitment was conducted using convenience sampling, driven by contextual constraints and available resources, the minimum sample size calculation should be considered a reference for the study’s statistical power rather than a guarantee of the sample’s probabilistic representativeness. The geographical distribution of the sample was determined proportionally to the nursing population registered in the professional register. Specifically, minimum quotas were set at 43% for the North (n=165), 21% for the Centre (n=81), and 36% for the South and Islands (n=138), to ensure adequate territorial coverage. Although this approach does not constitute stratified sampling in the strict sense, it was intended to reduce the risk of geographical over- or under-representation within the sample.
Results
Socio-Demographic Characteristics of the Sample (N = 384)
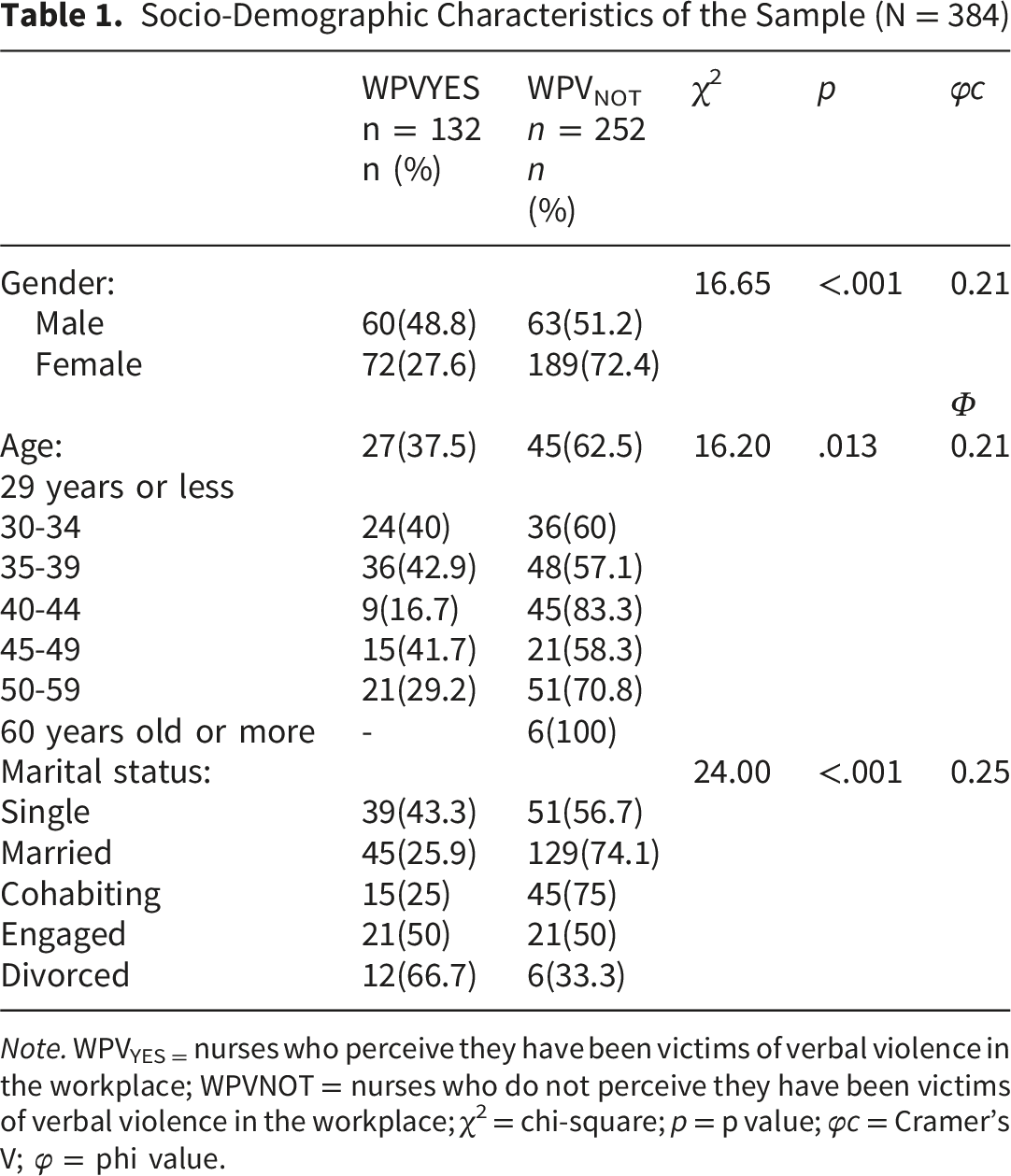
Note. WPVYES = nurses who perceive they have been victims of verbal violence in the workplace; WPVNOT = nurses who do not perceive they have been victims of verbal violence in the workplace; χ2 = chi-square; p = p value; φc = Cramer’s V; φ = phi value.
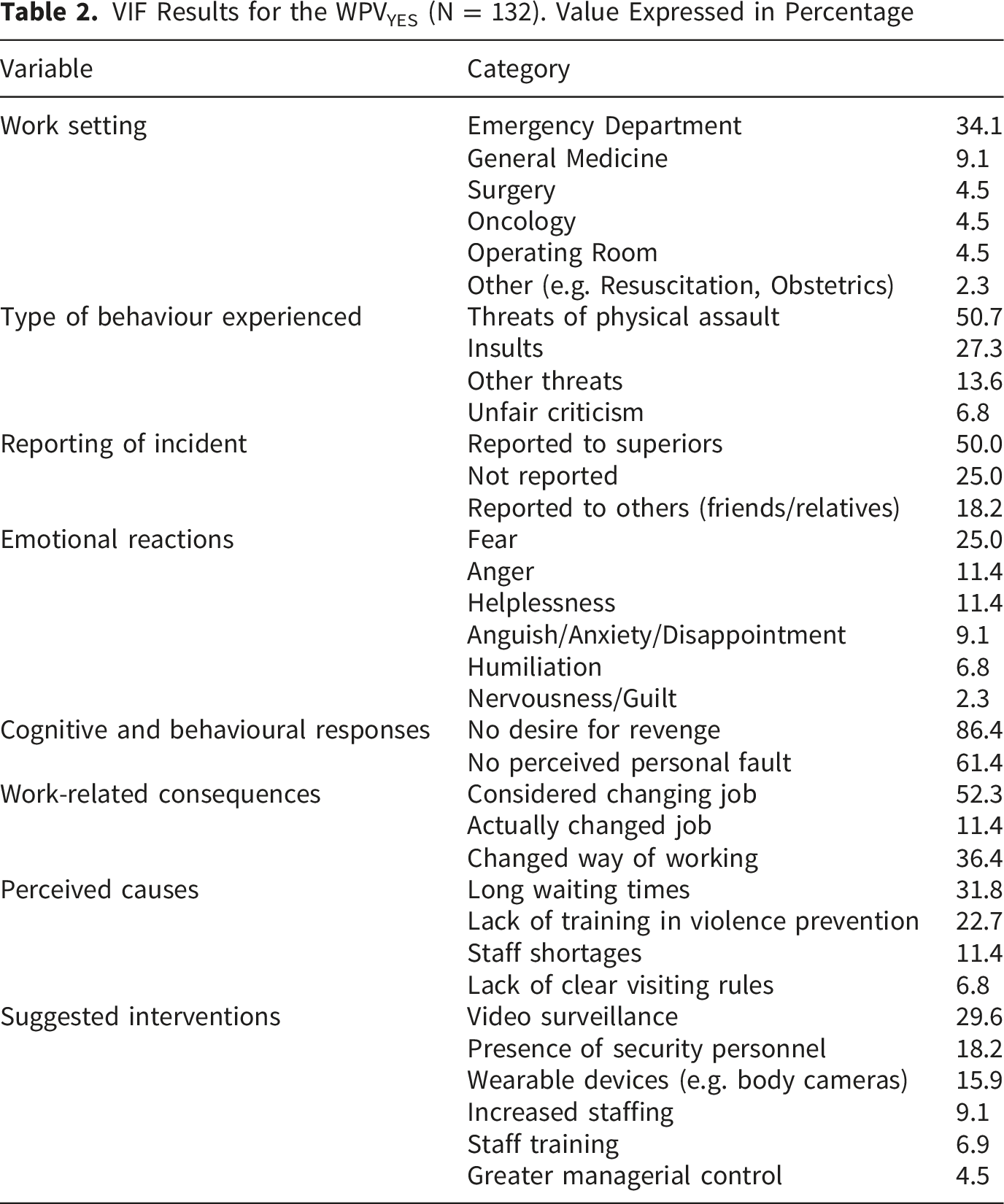
VIF Results for the WPVYES (N = 132). Value Expressed in Percentage
OLBI, GHQ-12, Self-Efficacy and Brief COPE Results (N = 384)
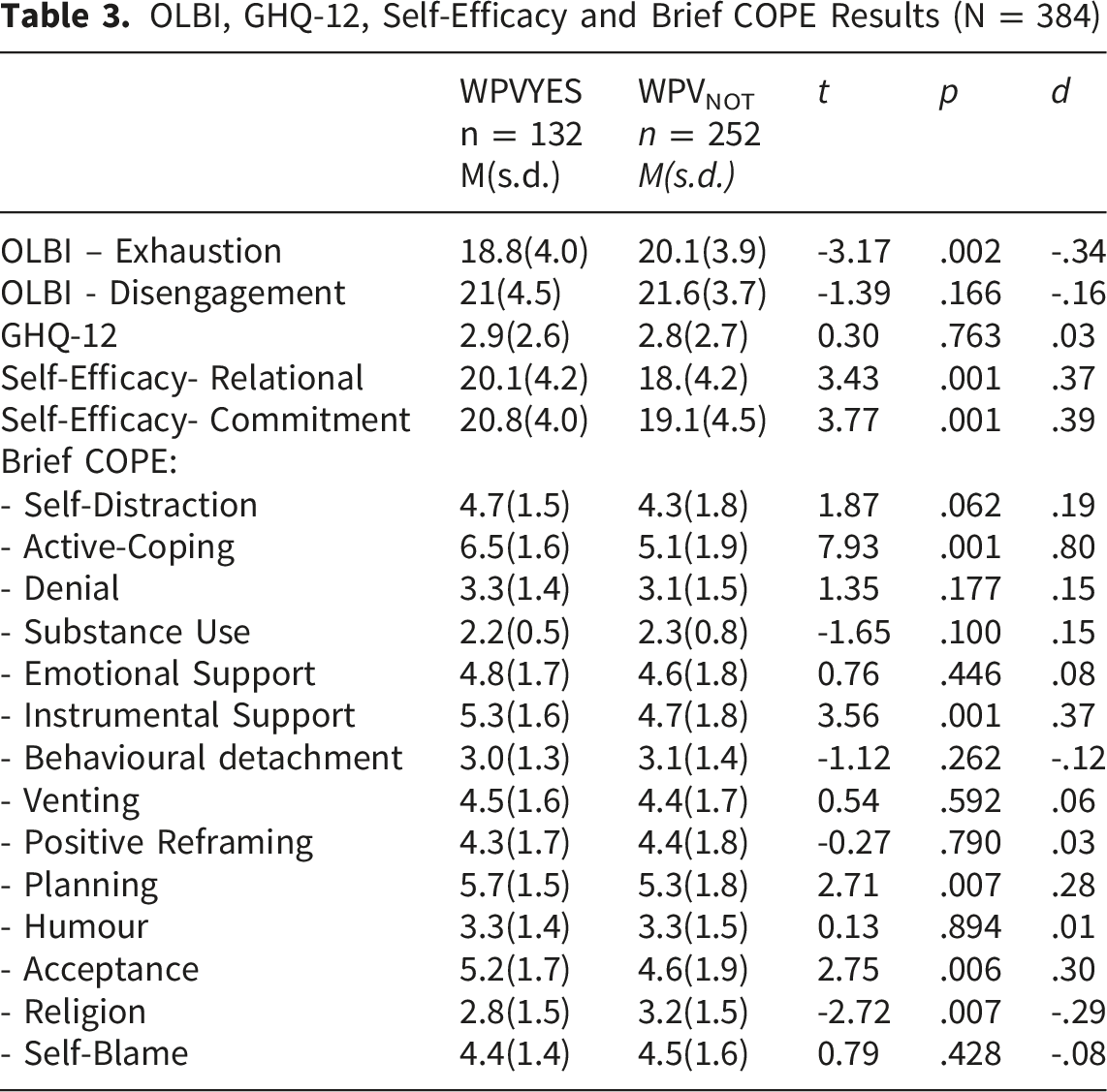
The t-test result indicates that WPVYES score lower on exhaustion than WPVNOT. The perceived psychological distress score does not reach the cut-off of 4, which would indicate possible criticality, although for WPV it is higher and at the attention threshold. Regarding self-efficacy, WPVYES tend to report a greater perception of self-efficacy than WPVNOT, both in relational and commitment aspects. The coping strategies of Active Coping, Instrumental Support, Planning, and Acceptance were reported more frequently by WPVYES than by WPVNOT, while the Religion strategy was reported more frequently by WPVNOT than by WPVYES.
Correlation Analysis in WPVYES and WPVNOT
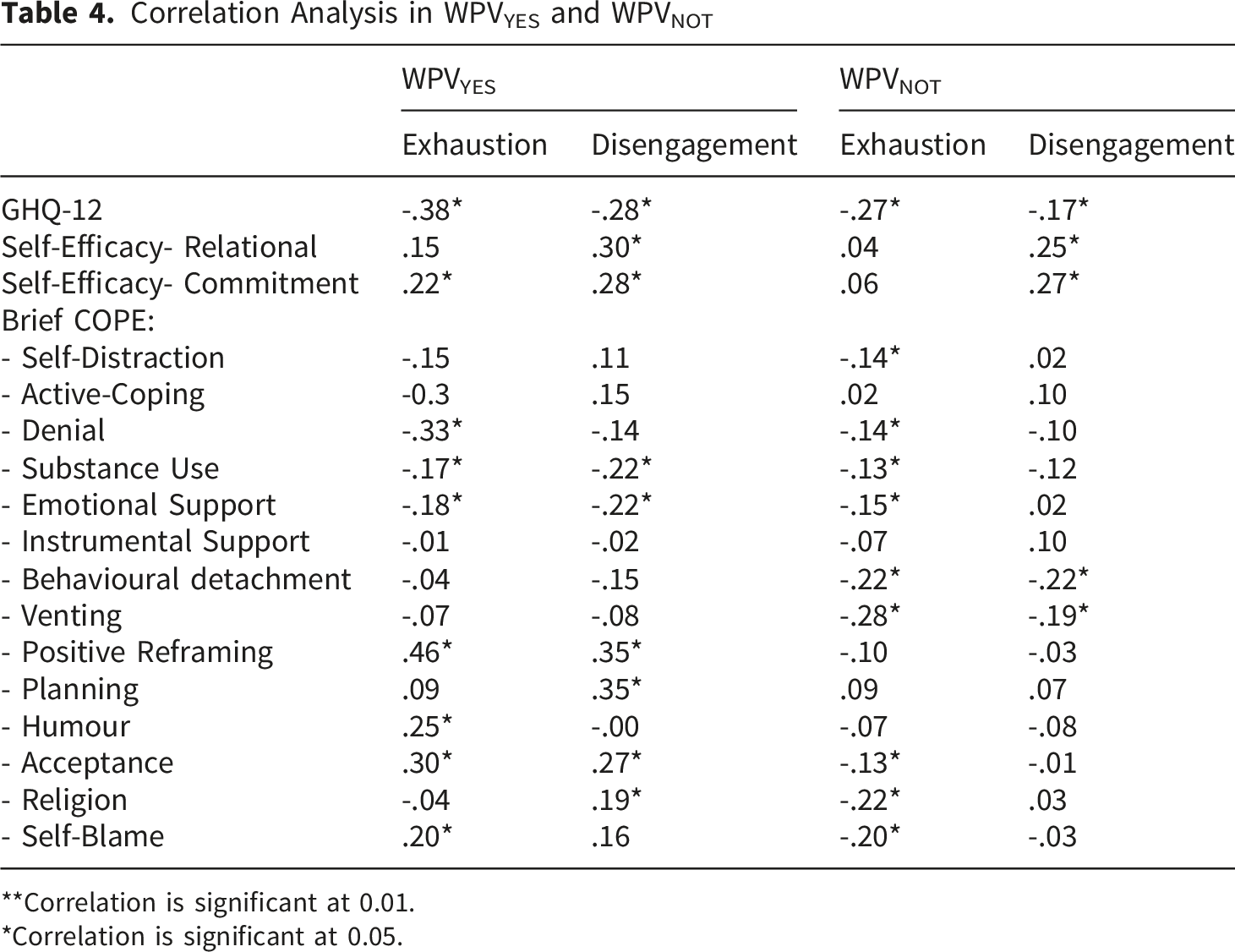
**Correlation is significant at 0.01.
*Correlation is significant at 0.05.
Regression Analysis in WPVYES. Dependent Variable: Burnout Exhaustion
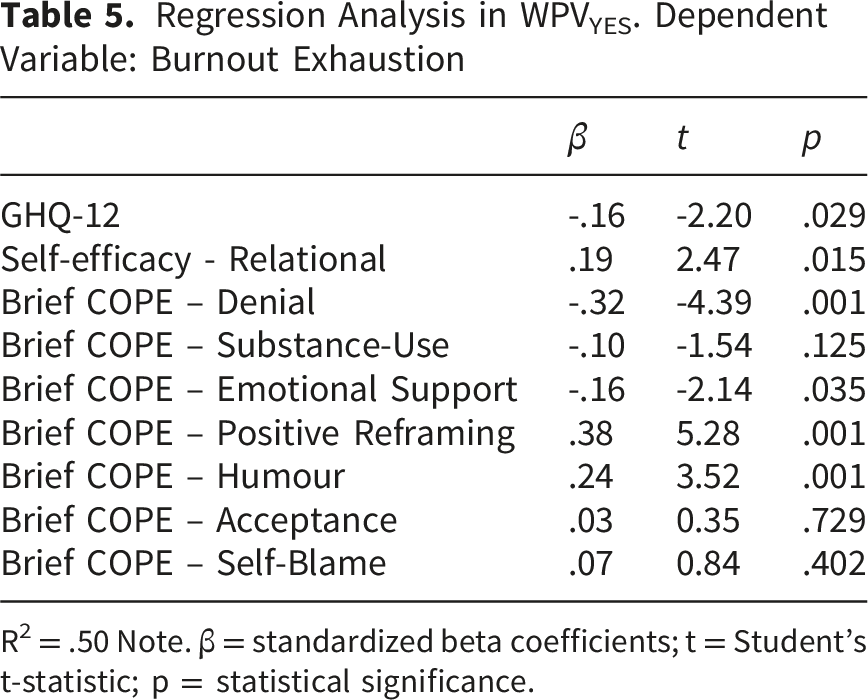
R2 = .50 Note. β = standardized beta coefficients; t = Student’s t-statistic; p = statistical significance.
Regression Analysis in WPVYES. Dependent Variable: Burnout Disengagement
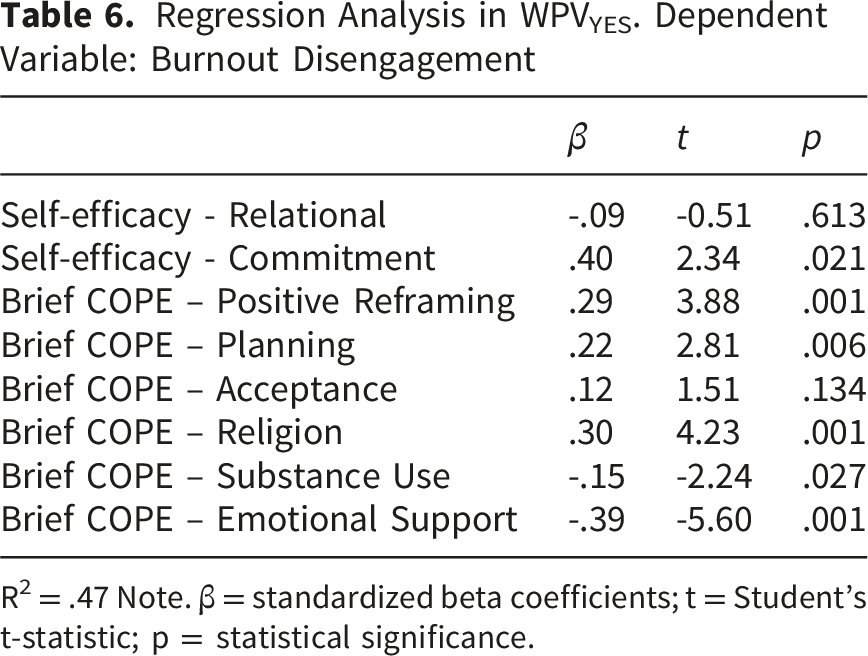
R2 = .47 Note. β = standardized beta coefficients; t = Student’s t-statistic; p = statistical significance.
Regression Analysis in WPVNOT. Dependent Variable: Burnout Exhaustion
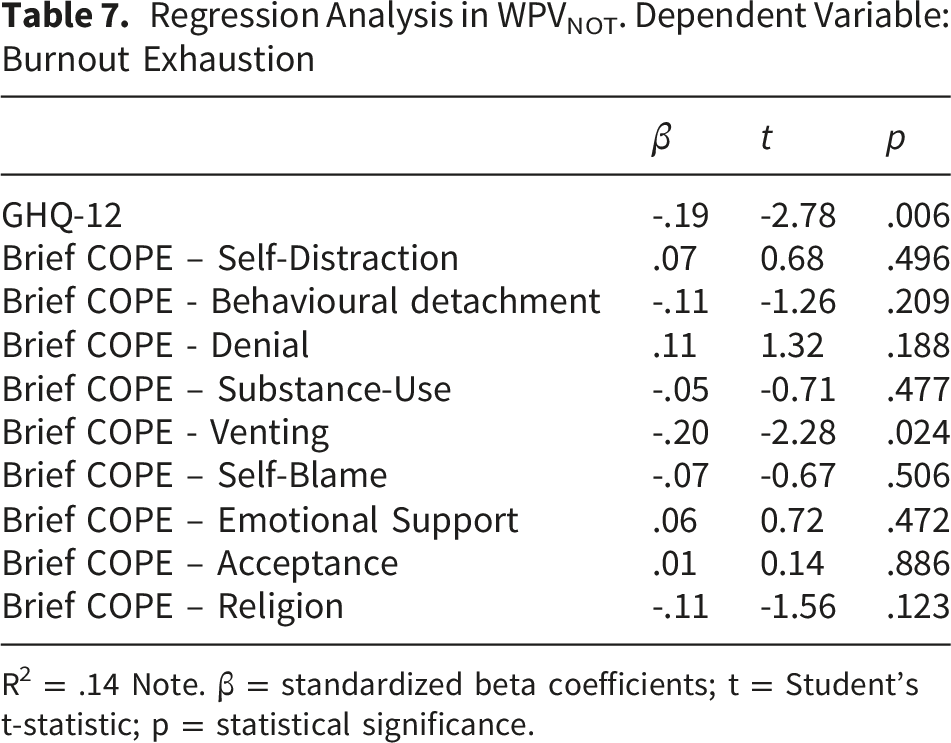
R2 = .14 Note. β = standardized beta coefficients; t = Student’s t-statistic; p = statistical significance.
Regression Analysis in WPVNOT. Dependent Variable: Burnout Disengagement
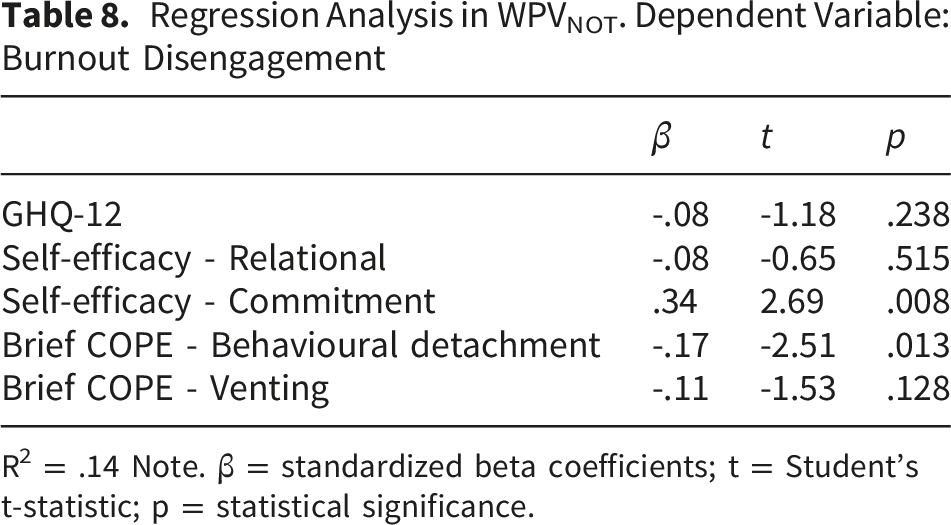
R2 = .14 Note. β = standardized beta coefficients; t = Student’s t-statistic; p = statistical significance.
In the WPVYES group, GHQ-12 emerged as a significant negative predictor of Exhaustion, indicating that as work-related exhaustion increases, the perceived level of psychological distress decreases. With regard to coping strategies, differentiated effects emerged. Denial and Emotional support were negative predictors of Exhaustion, while Positive reframing and Humour were associated with increased Exhaustion.
Commitment-related self-efficacy emerged as a strong positive predictor of Disengagement. Among coping strategies, Positive reframing, Planning, and Religion were positively associated with Disengagement, whereas Emotional support and Substance use showed a negative association.
In the WPVNOT group, the regression model for Exhaustion explained a substantially smaller proportion of variance (R2 = .14). The GHQ-12 was the only significant predictor for Exhaustion. The coping strategy of Venting was negatively associated with Exhaustion.
Commitment-related self-efficacy emerged as the only significant positive predictor. The Behavioural detachment coping strategy showed a negative association with Disengagement.
Discussion
The present study examined the prevalence and characteristics of verbal WPV among Italian nurses, with a specific focus on individual psychological processes involved in the development of burnout and psychological functioning. In line with the literature on occupational violence in healthcare settings (Somani et al., 2021) and within the theoretical framework of Social Cognitive Theory (Bandura, 2001), the study explored how personal resources are associated with burnout dimensions under conditions of exposure and non-exposure to verbal WPV. The findings highlight that the associations between self-efficacy, coping strategies, and burnout differ according to nurses’ experiences of verbal WPV. These results are consistent with the hypothesis that the presence of distinct patterns of association reflect differentiated psychological adaptation processes. More specifically, exposure to verbal WPV appears to shape how personal resources relate to exhaustion and disengagement, showing that their effect is neither linear nor consistently protective, but varies depending on the situation. In the analysed sample, 34.4% of nurses reported experiencing episodes of verbal WPV. This prevalence is consistent with national estimates (Cesare et al., 2025; Nursing Up, 2025) and with international literature (Pien et al., 2025; Wang et al., 2025). A possible underestimation of this figure may be attributable to cognitive adaptation processes to verbal WPV, widely described in nursing contexts, particularly in emotionally intense care settings (Nowrouzi-Kia et al., 2019). Significant sociodemographic differences emerged between WPVYES and WPVNOT groups. Male nurses were overrepresented in the WPVYES group. While numerous studies report a higher prevalence of WPV among women (also reflecting their numerical predominance in nursing; see Al-Qadi, 2021), other evidence suggests that men may be more frequently exposed to confrontational situations, particularly in high-risk units such as emergency departments, or may be more inclined to interpret and label certain interactions and behaviours as violent (Pich et al., 2010). These findings underscore the importance of considering gender in relation to professional roles, social expectations, and subjective attribution processes related to violence.
Age also emerged as a relevant factor: nurses aged between 40 and 44 years reported significantly fewer experiences of verbal WPV. This finding is consistent with models of professional development that attribute a protective role to work experience, facilitating the consolidation of emotional regulation skills, anticipation of critical situations, and cognitive restructuring of aggressive interactions (Chapman et al., 2010; Itzhaki et al., 2015). Conversely, younger or less experienced nurses may be more exposed to feelings of threat and helplessness (Somani et al., 2021). Additionally, divorced nurses reported greater exposure to verbal WPV, a finding that may reflect reduced availability of social support resources (Pandey et al., 2018).
Another interpretative key concerns the subjective nature of verbal WPV perception, which may be substantially modulated by psychophysical fatigue and career stage. During early career phases, when professionals are more exposed to high workload, disrespectful communicative behaviours by patients or relatives are more likely to be appraised as aggressive or violent (Rogers et al., 2016). By contrast, in later career stages, characterised by more consolidated coping resources, the physical and emotional wear and tear associated with prolonged work exposure may foster a reframing of similar behaviours as intrinsic challenges of the care context (Li et al., 2020). This perspective suggests that verbal WPV should be understood as a psychologically mediated experience, shaped by fatigue levels, self-regulatory resources, and cognitive appraisal processes (Roczniewska & Bakker, 2021). This interpretation aligns with transactional stress models (de Cordova et al., 2024; Lazarus & Folkman, 1987).
In line with previous literature, verbal WPV episodes were predominantly reported in high-pressure care contexts (Nowrouzi-Kia et al., 2019; Wang et al., 2025). From a psychological perspective, the reported emotional reactions may indicate a perceived threat to personal and professional integrity, consistent with models of occupational traumatic stress (Kafle et al., 2022).
Contrary to some previous literature (Cao et al., 2023; Chen et al., 2022), WPVYES nurses reported lower levels of emotional exhaustion than WPVNOT nurses. Although this result may seem counterintuitive, it aligns with models of psychological adaptation to chronic stress, which propose a progressive modulation of emotional activation as a functional strategy (Chapman et al., 2010; Pien et al., 2025). In line with models of chronic stress adaptation, repeated exposure to emotionally challenging interactions may lead to reduced emotional reactivity or recalibration of exhaustion thresholds (McFarlane, 2010). Such processes may be functional in the short term but do not necessarily correspond to positive mental health outcomes (Radley & Herman, 2023), as shown by the concurrently higher levels of psychological distress observed among WPVYES nurses. However, this interpretation must be approached with caution. The cross-sectional design of the study does not allow a clear distinction between genuine adaptive processes and potential methodological artefacts. In particular, alternative explanations cannot be ruled out, including social desirability effects, violence normalisation, selection bias, or survivorship phenomena, whereby more vulnerable professionals may have already left high-risk work environments (Hutchinson et al., 2006).
With respect to Hypothesis 1, the results only partially support the expected protective role of self-efficacy. Although nurses exposed to verbal WPV reported higher levels of perceived self-efficacy, both relational and commitment-related self-efficacy were positively associated with disengagement and, to a lesser extent, with exhaustion. This suggests that, under conditions of chronic verbal violence, self-efficacy may reflect a form of functional adaptation aimed at sustaining professional performance, instead of a linear protective factor against burnout. This finding reinforces the role of self-efficacy as a central motivational construct, shaping cognitive appraisal of stressful situations and perceived control (Bandura, 2001). Consistent with Hypothesis 2, higher self-efficacy levels were associated with more frequent use of problem-focused and cognitive regulation coping strategies, which are generally linked to more favourable psychological outcomes (João & Portaleda, 2023). In contrast, greater reliance on Religious coping in the WPVNOT group may reflect stress attribution processes less directly connected to experiences of violence.
Correlation and regression analyses indicated that, in both groups, psychological distress (GHQ-12) is significantly and negatively correlated with Exhaustion and Disengagement, indicating that higher levels of burnout are associated with poorer perceived psychological well-being. However, these associations are stronger in the WPVYES group, particularly for Exhaustion, suggesting that among nurses exposed to verbal WPV, burnout is more closely linked to psychological distress (Grinberg et al., 2022; Zafar et al., 2016). The finding that the GHQ-12 is a negative predictor of exhaustion in the WPVYES group requires methodological clarification. The GHQ-12 score was calculated using the bimodal method (0-0-1-1), which provides a measure of current psychological distress and does not represent a linear continuum of well-being (Comotti et al., 2023). In this context, the negative association between psychological distress and exhaustion may be interpreted as indicating a functional decoupling between the dimensions of burnout measured by the OLBI and the general psychological distress assessed by the GHQ-12. Nurses exposed to chronic verbal violence may report lower levels of perceived exhaustion (reflecting an adaptive recalibration of their emotional threshold) while simultaneously showing indicators of psychological distress. Regarding self-efficacy, notable differences emerge between the two groups. In the WPVYES group, both relational self-efficacy and commitment-related self-efficacy show significant positive correlations mainly with Disengagement, and partially with Exhaustion. This finding suggests that, under exposure to verbal WPV, a strong sense of professional competence and commitment may coexist with emotional distancing from work (Pien et al., 2025). In contrast, in the WPVNOT group, self-efficacy is associated primarily with Disengagement, and more weakly, indicating a more linear relationship between personal resources and burnout, confirming hypothesis 3.
The most pronounced differences concern coping strategies. In the WPVYES group, several strategies traditionally considered adaptive are positively correlated with Exhaustion and/or Disengagement. In contexts of chronic verbal WPV, coping strategies appear to operate in a context-dependent manner instead of being inherently protective or harmful (Yang et al., 2025). Strategies traditionally classified as maladaptive, such as denial or temporary emotional withdrawal, may provide short-term containment in situations perceived as uncontrollable (Needham, 2006). Conversely, cognitively demanding strategies such as positive reframing or planning may sustain professional performance at the cost of increased emotional resource expenditure, thereby contributing to burnout over time (Hobfoll, 1989; Waddill-Goad, 2023). In this study, the effectiveness of stress management strategies seems to depend on the chronicity of the stress, the perception of controllability, and the level of perceived organisational support. In the WPVNOT group, a pattern more consistent with traditional occupational stress models emerges: maladaptive strategies are negatively associated with burnout, whereas most adaptive strategies show no significant associations. This suggests that, in the absence of verbal WPV, burnout dynamics are more “classical” and less shaped by defensive cognitive restructuring processes (Regan et al., 2009). Regression models showed that, in the WPVYES group, self-efficacy and coping explained a substantial proportion of variance in emotional exhaustion and Disengagement (R2 ≈ .47–.50), whereas these relationships were less pronounced in the WPVNOT group. This supports a contextual and process-oriented conception of coping, according to which the effectiveness of strategies depends on stress duration and perceived organisational support (Beh & Loo, 2012).
From a theoretical perspective, these results suggest that self-efficacy should be understood as a context-dependent, and therefore dynamic, resource whose role varies depending on stress exposure and coping processes (Benight & Bandura, 2004; Cabrera-Aguilar et al., 2023). Importantly, focusing on individual psychological resources should not be interpreted as shifting responsibility from organisational to personal levels (Galanti et al., 2024; Hu et al., 2022; Lu et al., 2023).
Implication for Practice
Multilevel interventions should be designed to be complementary and integrated at the individual, team, and organisational levels. At the individual level, interventions should extend beyond developing coping skills to include motivational processes such as self-efficacy and work engagement. Training programs based on Social Cognitive Theory can strengthen the perception of agency and proactive coping. Reflective interventions can also help differentiate between functional adaptation and defensive disengagement (Islam et al., 2023). At the team level, structured initiatives focused on communication, conflict management, and group coping can enhance shared resources and the perception of psychological safety. Peer support can help professionals process experiences of violence and reduce the risk of normalizing aggression (Fujii & Iwasa, 2025; Zhang et al., 2021). This is especially relevant given evidence that adaptive coping with chronic exposure may mask deep-seated distress. At the organisational level, healthcare institutions should implement explicit, structured strategies to prevent and manage verbal WPV, including visible managerial support and targeted training for supervisors (Lim et al., 2022). However, these implications should be interpreted with caution due to the methodological limitations noted above, particularly the cross-sectional design and the non-probability sampling approach.
Strengths and Limitations
This study has several strengths. Firstly, it contributes to the literature on verbal abuse in the workplace among Italian nurses, showing that exposure to this phenomenon is associated with differentiated psychological adaptation processes. Furthermore, the use of validated psychometric instruments with good reliability indices has enabled the identification of distinct patterns of adaptation to work-related stress in healthcare settings affected by verbal WPV. At the same time, this study has several limitations that should be considered when interpreting the results. A primary source of potential bias concerns data collection. Data were gathered exclusively through self-administered questionnaires, which may have introduced response distortions, particularly social desirability bias. Nurses who experienced verbal WPV may have underestimated incidents (see Peach et al., 2023) or downplayed their emotional impact to conform to professional norms that value resilience, emotional control, and competence (Morera et al., 2024). A related methodological concern is the reliance on subjective perceptions of verbal WPV instead of objective or externally verified indicators. As suggested by Nowrouzi-Kia et al. (2019) and Välimäki et al. (2022), the assessment of verbal WPV is inherently subjective and can be influenced by individual differences in fatigue, emotional resources, professional experience, and cognitive evaluation styles. Furthermore, the operational definition used in this study focuses on direct and explicit manifestations of verbal WPV (Nowrouzi-Kia et al., 2019; Wang et al., 2025). It is well known that this operationalization does not include more subtle forms of psychological violence, such as professional devaluation by colleagues (Einarsen et al., 2020). This choice could lead to an underestimation of the actual prevalence of the phenomenon and a partial representation of the experience of victimization. Future research should include measures capable of capturing latent and relational forms of WPV. The cross-sectional design also precludes any causal interpretation of the observed associations. In particular, it is unclear whether higher self-efficacy and certain coping strategies serve as antecedent protective resources or develop as adaptive responses to repeated exposure to verbal WPV. Finally, although efforts were made to ensure geographic representativeness, the use of non-probability sampling and online recruitment may limit generalizability. Therefore, the results cannot be generalized to the entire Italian nursing population and should be interpreted as indicative of trends observed within a specific sample.
Conclusion
This study highlights verbal WPV as a pervasive and structurally embedded occupational hazard in nursing practice. The findings show that nurses exposed to verbal WPV do not necessarily experience higher levels of emotional exhaustion; rather, they display complex psychological adaptation patterns, including increased self-efficacy, selective coping strategies, and partial emotional disengagement from work. These patterns should not be seen as indicators of well-being, but as adaptive or defensive responses that enable continued functioning in chronically demanding environments. Self-efficacy and coping strategies seem to play a key role in shaping nurses’ responses to verbal WPV. However, their role appears context-dependent: strategies considered adaptive can help maintain work performance, but they come with a higher emotional cost. These findings raise concerns about the risk of accepting verbal WPV as “part of the job” (Magnavita et al., 2024) and highlight the ethical and organisational implications of relying solely on individual resilience. From a nursing and managerial perspective, the results reinforce the need to move beyond individual-level interventions and address verbal WPV through organisational responsibility.
Supplemental Material
Supplemental material - Verbal Workplace Violence and Burnout Among Italian Nurses: The Role of Self-Efficacy and Coping
Supplemental material for Verbal Workplace Violence and Burnout Among Italian Nurses: The Role of Self-Efficacy and Coping by Gennaro Laus, Sipontina Rita Zerulo, Antonella Varetto, Maria Michela Gianino, Daniela Acquadro Maran in Sage Open Nursing
Footnotes
Acknowledgements
The authors would like to thank all the nurses who generously participated in this study and shared their experiences. Their contribution was essential to the completion of this research.
Ethical Considerations
The study was conducted in accordance with current regulations and adhered to the principles of the Declaration of Helsinki. An informed consent letter preceded the questionnaire. In line with national and institutional guidelines, formal Ethics Committee approval was not deemed mandatory for this type of study, as it involved anonymous participation and did not include the collection of identifiable or sensitive personal data, in accordance with European Regulation 2016/679 (GDPR).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.